By Celia Kitzinger, 7th April 2021
UPDATE (9th February 2024): The General Medical Council (GMC) has investigated Dr Pullicino’s conduct + decided that no action is needed in respect of his registration. The Christian Legal Centre welcomes the GMC findings and says: “We need more doctors + experts who are prepared to be fearless in defending the patient’s right to life”.
I’ve observed more than thirty expert witnesses give oral evidence in the Court of Protection – but never one so manifestly out of his depth as retired neurologist, Dr Patrick Pullicino, at a hearing before Mr Justice Cohen (Z v University Hospitals Plymouth NHS Trust & Ors (Rev 1) [2020] EWCOP 69).
According to Lord Justice Peter Jackson, one of the Court of Appeal judges who reviewed the case, Dr Pullicino’s evidence “lacked every characteristic of credible expert evidence and it is not surprising that the Judge rejected it as effectively worthless”.
So what went wrong? Why did an experienced neurologist provide “effectively worthless” evidence, and how was it possible for this to be admitted to court and to take up many hours of court time with senior barristers and a Tier 3 judge sitting until past 8pm one evening? How did this application leapfrog to the front of the hearings list, when many other vulnerable disabled people are waiting many months for decisions about fundamental aspects of their lives?
Background
The evidence Patrick Pullicino gave, if accepted, had the potential to reverse the court ruling just over a fortnight before that life-sustaining treatment could be withdrawn from the person at the centre of the case – a middle-aged man known in published judgments as “RS” (University Hospitals Plymouth NHS Trust v RS & Anor [2020] EWCOP 70).
RS had suffered a cardiac arrest on 6th November 2020 during which his heart stopped for at least 45 minutes, and he would surely have died but for cardio-pulmonary resuscitation. The inevitable consequence was severe and irreversible brain damage.
His treating clinician and the independent expert appointed by the court (Dr Dominic Bell, a Consultant in Intensive Care Medicine) diagnosed him as being first in a ‘coma’ and then later in a ‘vegetative state’ (i.e. unconscious, unaware of himself or his surroundings). The clinicians agreed that he was likely to remain completely unconscious, but there was a small possibility (the independent expert put it at between 10% and 20%) that he might in future reach a state known as ‘minimally conscious minus’.
Dr Pullicino’s evidence, by contrast, was that RS either was already, or was showing signs of becoming, minimally conscious. He said that RS moved his eyes towards people by the bedside who called his name and showed “a clear emotional response to the presence of the family members”. This meant that his prognosis was much better than previously suggested. Dr Pullicino even said in court that “this man has a 50% chance of being independent in his own home”.
The difference in diagnosis and prognosis had huge implications for RS’s treatment, because, in English law, considerable weight is attached to what the patient would decide for themselves if they could. RS’s wife had given evidence that RS would want, as a minimum, to be able to interact with her and with his children – even if only to squeeze their hands or move a finger to acknowledge their presence. According to the court’s expert witness, Dr Dominic Bell, this was very unlikely ever to happen. At most, he might in future be able to acknowledge the presence of a human being, but there would be no means of knowing whether he was responding to a particular person or simply to someone, anyone, for example, holding his hand.
On that basis, RS’s wife had come to the view that RS would not want to continue to receive the clinically assisted nutrition and hydration (via a naso-gastric feeding tube) that was keeping him alive.
By contrast, if Patrick Pullicino’s diagnosis was correct, then it seems certain that RS would want life-sustaining treatment to continue.
At a previous hearing, before Pullicino’s evidence became available, Cohen J had ruled that it was not in RS’s best interests to be given nutrition and hydration and that such treatment could be lawfully discontinued. At this second hearing, he was being invited to reconsider this decision in the light of new evidence that RS may be showing more evidence of recovery than previously thought.
However, in his judgment (Z v University Hospitals Plymouth NHS Trust & Ors (Rev 1) [2020] EWCOP 69), Mr Justice Cohen said he had “severe misgivings” about Pullicino’s evidence and concluded “I do not think I can place any weight on the evidence of Dr Pullicino“, adding, “I was concerned about the level of his objectivity”.
I don’t want to rehearse the scientific reasons for dismissing Patrick Pullicino’s evidence: they are presented by Cohen J in his judgment (paras. 24-30) and they reflect the professional opinion of the independent expert who also looked at Dr Pullicino’s evidence and subsequently re-examined the patient, and found him still to be vegetative – as well as the judge’s own assessment of Dr Pullicino’s evidence in the (virtual) witness stand. The science behind the diagnosis, and the problems with Dr Pullicino’s evidence, are also discussed more broadly in the previous blog post (here) by Jenny Kitzinger, from the Coma and Disorders of Consciousness Research Centre.
Instead, I want to consider the basis for Mr Justice Cohen’s concern with Dr Pullicino’s “objectivity”, and in particular the way in which religious beliefs and ethical commitments have infused this case.
A Roman Catholic perspective on clinically assisted nutrition and hydration
The Roman Catholic faith was central to the family’s disagreement about what RS would want in this situation.
Mr Justice Cohen said, “The issue is focused around RS’s religious faith, his adherence to the tenets of the Catholic religion and their application in these circumstances.”
According to the birth family (RS’s mother, sisters and niece), RS:
“… was religiously conservative, opposed to abortion, even for an unborn child likely to be medically compromised and opposed to euthanasia. It was a matter of upset to him that he and his wife were unable to obtain an annulment of her previous marriage and thus marry in church and that thereafter he was unable to take Holy Communion. That many Catholics would not stop taking Communion in such circumstances shows, they say, his adherence to his religion. Taking all these factors together, they say, would show that he would not want his life terminated if it could be sustained. The preservation of life would outweigh all other factors in his thinking.” (University Hospitals Plymouth NHS Trust v RS & Anor [2020] EWCOP 70 (15 December 2020))
According to his wife, although RS was religious and went to church at least once a month, this:
“… did not mean that he, certainly by 2020, adhered strictly to all aspects of the doctrine of his faith. He had married her, a divorcee. He pursued their relationship in the full knowledge of her status and they began their family life before marrying in a registry office.” (University Hospitals Plymouth NHS Trust v RS & Anor [2020] EWCOP 70 (15 December 2020))
In recent years there had been relatively little contact (how much, exactly, was disputed) between RS and his birth family, many of whom lived in Poland – and RS had not seen those of his family who live in England, since about 2011. That was one reason why the judge placed much greater weight on his wife’s evidence of RS’s views because it was (he said) she who knew him best.
Stating that “I do not accept that his religious beliefs make him unlikely to have said what his wife says that he said“, the judge ruled that clinically assisted nutrition and hydration could be withdrawn. (University Hospitals Plymouth NHS Trust v RS & Anor [2020] EWCOP 70 (15 December 2020))
When the birth family sought permission to appeal, they did not initially challenge the medical consensus about RS’s diagnosis and prognosis. Instead, they said the judge’s decision was unjust because he hadn’t considered how RS would have wanted to be treated against the backdrop of the tenets of his Catholic faith. In their view, Mr Justice Cohen moved far too swiftly to the conclusion that this devout Catholic man would have wanted something that was in conflict with the teaching of the Church – that the end of life is a matter for God and not for Man. ( para. 13, Z v University Hospitals Plymouth NHS Trust & Anor (Rev 3) [2020] EWCA Civ 1772 (23 December 2020))
For many Catholics, food and water – whether provided orally or via a feeding tube – are part of basic care, and not a form of medical treatment. (I note, parenthetically, that in my experience, this is true for many people, both those with and those without any specific faith: it is, in fact, not widely known – even among health care professionals – that a feeding tube is defined by English law as a medical treatment.)
Pope John Paul II clearly stated that the Catholic Church regards nutrition and hydration (however provided) as a natural means of preserving life:
“I should like particularly, to underline how the administration of water and food, even when provided by artificial means, always represents a natural means of preserving life, not a medical act. Its use, furthermore, should be considered, in principle, ordinary and proportionate, and as such morally obligatory, insofar as and until it is seen to have attained its proper finality, which in the present case consists in providing nourishment to the patient and alleviation of his suffering. The obligation to provide ‘the normal care due to the sick’ in such cases includes, in fact, the use of nutrition and hydration.” (John Paul II Address on “Life-sustaining treatments and the vegetative state” (20 March 2004), 4)
The view of Pope John Paul II, who was – like RS – Polish, is particularly pertinent because one of RS’s treasured possessions was a photograph of himself as a young man during an audience with this pope. This image was used by LifeFunder (“a platform created to serve the pro-life, pro-family, and Christian communities”) to raise money to fund the legal challenge to the court decision.
Figure 1: LifeFunder (Note: I’ve replaced a small black band over RS’s eyes in the original with a large black square to ensure anonymity).

This same view of clinically assisted nutrition and hydration as ‘basic care’ has been expressed by the Catholic Bishops’ Conference of England and Wales.
“… the administration of water and food, even when provided by tube is a natural means of preserving life. Feeding someone or quenching their thirst is a fundamental expression of solidarity and care. Hence nutrition and hydration, even when clinically assisted, should be understood as elements of care which should be provided so long as they are needed and effective.” ( A Practical Guide to The Spiritual Care of the Dying Person. The Catholic Bishops’ Conference of England & Wales, Dept. for Christian Responsibility & Citizenship London: CTS, 2010, 2.6-2.10)
Although it’s not specifically reported in the judgments, it seems reasonable to assume that his birth family took the view that, as a Catholic, RS would have seen withdrawal of nutrition and hydration as a way of actively ending life, or as a form of euthanasia.
It’s not, in principle, contradictory to believe that you’d only want a life where you could interact (at least minimally) with your wife and children, and at the same time to believe that nutrition and hydration should never be withdrawn so long as they are sustaining life (even if it’s a life you wouldn’t otherwise want to be living).
In the Court of Appeal judgment, however, RS’s wife is reported as saying that RS did not regard ceasing treatment as “removing life” (quoted at paragraph 7, of the judgment), but it’s not clear whether or not, for RS, clinically assisted nutrition and hydration would have constituted “treatment” (as opposed to basic care).
In any case, permission to appeal against Mr Justice Cohen’s decision on the grounds that RS’s Roman Catholic faith had not been adequately scrutinised was refused. Clinically assisted nutrition and hydration was again withdrawn (having been reinstated to allow for this application to appeal).
It was after this, eight days later, that the case then returned to the Court of Protection, this time with a challenge to RS’s diagnosis, and with Dr Patrick Pullicino as an expert witness for the birth family.
Introducing Rev Dr Patrick Pullicino
Although the details aren’t entirely clear (since he was – the judge said – “unaccountably vague” on the matter), it seems that Dr Pullicino first learned about what was happening to RS through Pavel Stroilov, a consultant to the Christian Legal Centre. (Note: Stroilov has written an analysis of this case for Christian Concern here.) Dr Pullicino had also (either shortly before or shortly afterwards) read an article about RS’s case via what he described as an “American pro-life” organisation (LifeSiteNews, here).
After these initial sources of information, Dr Pullicino then had a conversation with RS’s niece, who subsequently went to the treating hospital on Christmas Day 2020 to “say goodbye” to RS. When at his bedside, she made videos of him while under instruction from Dr Pullicino on a Facetime call. He told her how to try to elicit responses from RS and she later sent him the video clips. The videos were made without the knowledge or permission of the court, the hospital or RS’s wife (described as a “deplorable ruse” in the Court of Appeal judgment (para 21)).
Dr Pullicino then emailed Pavel Stroilov as follows:
“I have just facetimed with RS and his daughter [sic: it was in fact his niece]. He looks to me to be in MCS.
He does appear to move his eyes preferentially to one side to voice but he would need time to be assessed by the MCS[1] or WHIM.
There is no way he should be left to die.
Fr Patrick”
(quoted in the published judgment here, para. 17)
As co-director of the Coma and Disorders of Consciousness Research Centre (alongside Jenny Kitzinger), I have carried out research and advocacy in the field of prolonged disorders of consciousness for more than a decade. I have never met any neurological expert who would provide even a preliminary diagnosis of the MCS (Minimally Conscious State) simply on the basis of a single brief FaceTime conversation with a family member at the patient’s bedside – and particularly not one intended to carry weight as evidence in court.
Dr Pullicino does say, both in the email to Pavel Stroilov and in a later letter addressed to RS’s niece, that further assessment is needed, with the implication that his initial diagnosis cannot be definitive. Nonetheless, he was apparently sufficiently confident of his own analysis to allow it to be used to challenge the diagnoses of the treating clinician and independent expert, both of whom had access to the patient’s records (including nursing records, MRI scans, and EEG), which Dr Pullicino did not.
On 27th December 2020, the birth family again applied to the Court of Protection asking to rely on Dr Pullicino’s evidence. The following evening, the duty judge, Mr Justice Holman, put a stay on Mr Justice Cohen’s order (that it was not in RS’s best interest to continue to receive clinically assisted nutrition and hydration) and treatment was restarted pending another hearing before Cohen J, on 30th December 2020.
Prompted by Dr Pullicino’s re-diagnosis of the patient, the independent expert Dr Bell carried out a full reassessment of RS (see paras. 32 and 33 of the judgment), and found that:
“RS is now established in VS [the Vegetative State] with no evidence of progression along the spectrum of PDOC [Prolonged Disorders of Consciousness] towards a MCS [Minimally Conscious State].” (para. 34 of the judgment).
An EEG recording made the day before this court hearing confirmed “a lack of brain activity to various types of stimulation” (para. 34 of the judgment). Dr Bell also examined the video-clips which Dr Pullicino claimed indicated possible consciousness.
“He did not interpret the video evidence as indicative of anything other than a VS [Vegetative State]. Observed features of VS do include brief eye movements towards people and objects, a startle reflex to loud noise and changes in facial expression without apparent cause.” [2]
How is it, then, that Dr Patrick Pullicino, an experienced and appropriately qualified neurologist, came to give “essentially worthless” evidence about RS’s diagnosis and prognosis in a court of law?
Being ‘open to God’ in medicine
In addition to being an experienced neurologist, Patrick Pullicino is a devout Roman Catholic. On 20th July 2019, he was ordained in St George’s Cathedral, Southwark as a new diocesan priest.
I do not know the religious faiths, if any, of the treating clinician or the independent expert who provided medical evidence in this case – nor that of the judge: internet searches have not turned up any information. It is however readily apparent that Patrick Pullicino’s faith has been central to the way he has lived his life and to the views he has publicly expressed in lectures, professional journals, and in other publications – including the mass media – over many years.
In 2013, in an interview with the Catholic Herald, he reflected on the importance of being open about his spiritual life in the medical context:
“A couple of years ago I started wearing a little crucifix on my lapel, not when I see patients, but just around the hospital. If you do believe in the spiritual, I think it is important to declare yourself.”
The interviewer commented on Pullicino’s rejection of the idea that science can explain everything.
“’That is a very limited view, especially in medicine, when one should be most open to God and a lot of the decisions have to come from the heart as well as from the mind,’ he says. ‘Today there are challenges all around [for doctors] because people are re-defining what is an acceptable quality of life.’” (Catholic Herald, 22nd March 2013)
Pullicino went on to describe his ethical concerns about “switching off” people in a vegetative state:
“A particular challenge in neurology is the question of consciousness and patients with ‘unresponsive wakefulness syndrome’ – previously described as being in a ‘persistent vegetative state’. In the past, many of these people simply wouldn’t have survived, but now that they do there is uncertainty over how they should be treated.
“People say these patients don’t actually have consciousness. The law even suggests they’re not really persons,[4]” says Dr Pullicino. “Modern magnetic resonance scanning shows that some of these patients do have thought patterns. But what do you do as a physician if you have a patient like this and perhaps their family says they want them to be switched off, but you don’t think that’s right?… I think it’s really important as a physician to have your own yardstick and say: ‘That’s as far as I’m willing to go.’” (Catholic Herald, 22nd March 2013)
Dr Pullicino has been clear about the importance of maintaining “the moral centre of the physician” (Neurology, 2014).
“In my opinion, the treating physician should have a subjective line drawn, over which they will not cross, even if the patient and the majority-driven respect for autonomy, demand it. Every physician has the right to exercise their own conscience. … [P]art of a physician’s role is to identify for the patient ‘what is or is not good and right for them’ even if it is perceived as paternalistic.” (Pullicino, 2014)
Withholding or withdrawing fluids is “euthanasia”
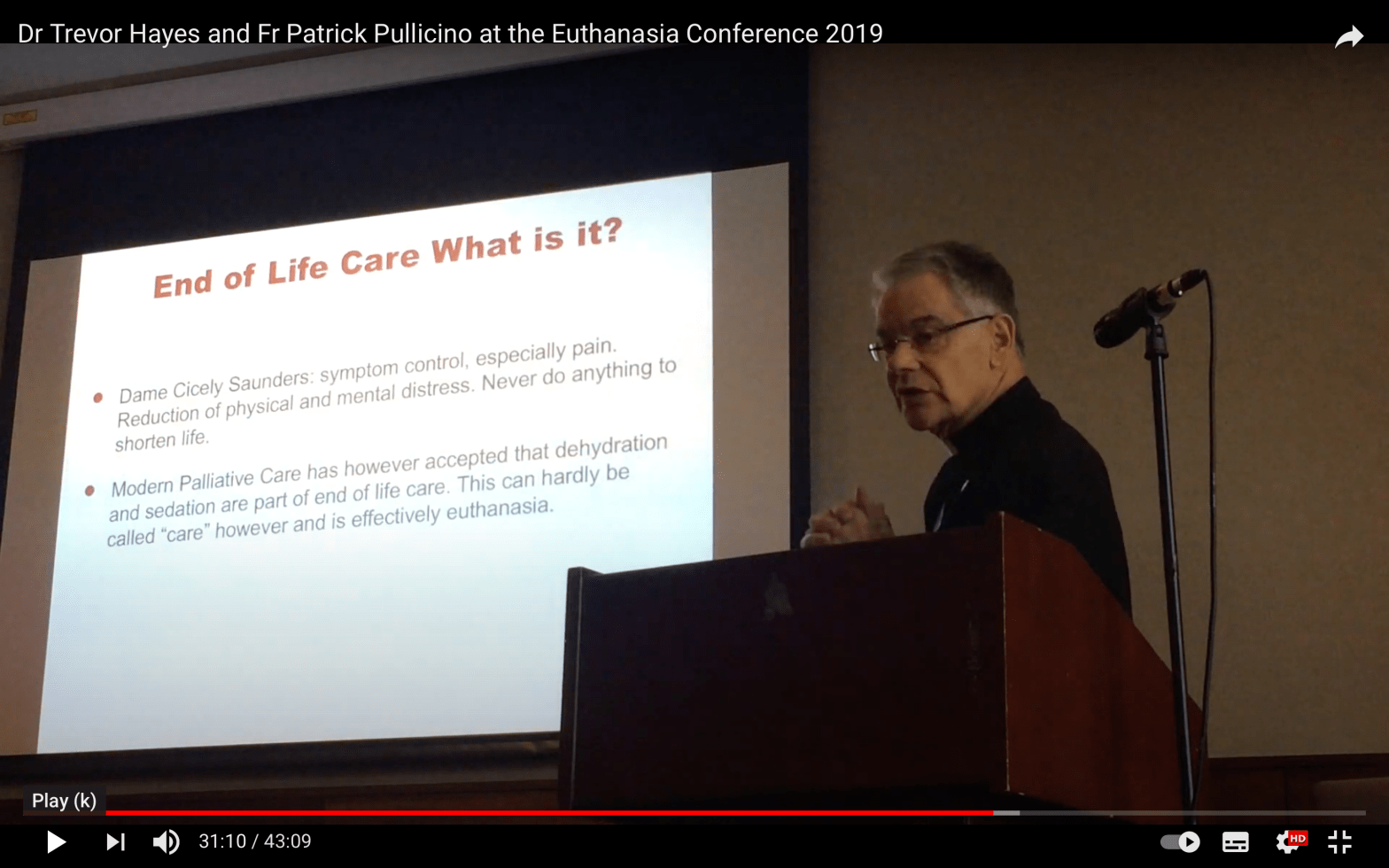
The illustration at the top of this blog post is a still from the YouTube video of a talk by Patrick Pullicino at a conference called “The Case Against Euthanasia”, organised by Doctors for Life Ireland in 2019.
He was introduced to the audience as “Father Patrick Pullicino”, “a newly ordained Catholic priest” and “chaplain at Springfields Psychiatric Hospital in London” – foregrounding (as he often does himself) his religious – and now clerical – position. He was also described as “a recently retired NHS neurologist and Professor of Clinical Neurology at the University of Kent” and “adjunct Professor of Neurology at Rutgers University of New Jersey” (02:50-03:33 minutes).
His talk on end-of life care is largely a criticism of the Liverpool Care Pathway (LCP) and of the approaches to end of life care that have succeeded it which, like the LCP, also limit clinically assisted nutrition and hydration at the end of life. One of his slides (23.01 minutes) advises that “Stopping hydration will kill”.
As he displays the slide in the illustration at the top of this blog post (31 minutes into the video), Patrick Pullicino describes dehydration and sedation as “effectively euthanasia”.
At the end of his talk, he was challenged by an audience member, Jane Fleming, a Consultant in Palliative Medicine at Health Service Executive Ireland (35 minutes into the video). She said that to align palliative care with euthanasia was “offensive”, pointing out that many people stop drinking at the end of life and that to send everyone to hospital for fluids would simply result in “the medicalisation of dying”. In response, Patrick Pullicino made clear the extent to which he is personally as well as professionally invested in providing fluids at the end of life.
In terms of dying with fluids, I’d say “yes’: if the alternative is that you may be killing somebody off from dehydration, then you do give everybody fluids. My wife, for example, died at home, and she was being looked after by the team that visits. And she was getting drowsy. And they said, “Oh well, she’s getting drowsy, we don’t want to give her any fluids”. I said, “Yes, I want her to have fluids. I don’t want her to die of dehydration.” In the end, I had to go to my ward, get a bag, and give her fluids. The last thing I was going to do was see my wife die of dehydration in front of me. You cannot- Patients, when they’ve stopped drinking, if you don’t give them fluids, you know, you dehydrate them and you hasten their death. […] The fact is that if somebody is drowsy and you don’t give them fluids … effectively what you do is you kill them off.” (Video: 37:35mins -39:10 mins)
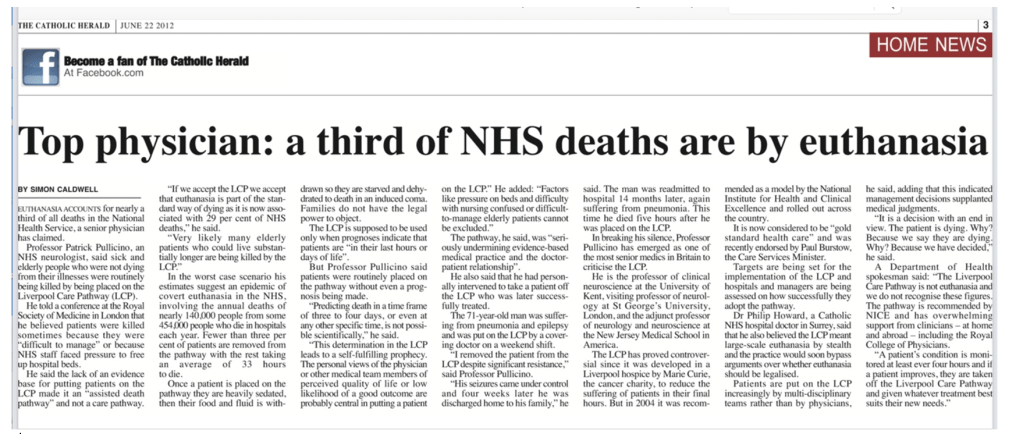
Pullicino has not been reticent about using words like “kill” and “euthanasia” when referring to withdrawal of life-sustaining treatment, or food and fluids. He told a conference at the Royal Society of Medicine that “euthanasia” accounts for nearly a third of all deaths in the National Health Service (Pullicino in Catholic Herald 22 June 2012) “Patients were killed sometimes because they were ‘difficult to manage’ or because NHS staff faced pressure to free up hospital beds”.
Figure 2: Catholic Herald, 22 June 2012
Dr Pullicino believes that fluids and nutrition should be given to all patients “at all times” – including patients with advanced dementia and those in comas (see Figure 3).
Figure 3: Extracts from “Death: Natural or assisted? A guide to medical end-of-life issues”, by Patrick Pullicino, published by the Catholic Education Resource Centre, 2018)

His position is that “the doctor has a moral obligation” (Figure 3) to continue to give fluids and nutrition in situations where death is highly likely to follow withdrawal; this means that Dr Patrick Pullicino has found himself fundamentally opposed to the policies and practices of many medical institutions.
He’s criticised the American Academy of Neurology for “leading [its] membership to accept ever more extreme forms of de facto euthanasia” by sanctioning withdrawal of clinically assisted nutrition and hydration under some circumstances – and draws a chilling parallel with murder in Nazi Germany via a quote from the Office of the Chief Counsel for War Crimes at Nuremberg (Burke, W, Pullicino, P & Coverdale, J. 2007. “The controversy over artificial hydration and nutrition” (letter). Neurology 68(5): 391-2.)
He’s criticised the British Medical Association guidance on decision-making about clinically assisted nutrition and hydration, as “terrible”, because it “facilitates the extension of end-of-life pathways to people with neurological diseases who are not dying” and “perpetuates the myth of ‘best-interests’ which has been shown to be erroneous” (Christian Concern, 15 August 2018)
In a letter to the American Academy of Neurology journal (dealing here primarily with extubation rather than withdrawal of nutrition and hydration), he wrote:
“We have lost the true understanding of how precious life is, regardless of its perceived quality. Neurologists, in particular, who daily care for patients with severe disability should be resolute in resisting that euthanasia become the answer to chronic disabling disease, even when the prognosis appears hopeless. […] Physicians must also not allow the absolute ethical imperative to save life to be subjugated to quality-of-life judgements made on the patient’s behalf. “(Pullicino, P & Burke, W. 1999. “Withdrawal of life support in the neurological intensive care unit” (letter). Neurology 53(9): 2215-6)
Dr Pullicino has spoken up clearly and confidently over the course of two decades for what he believes to be right – even when it flies in the face of medical consensus. He holds fast to the absolute ethical imperative to save life. He opposes withholding or withdrawing fluids because to do so is to hasten death, and this – for him – constitutes euthanasia and is morally unacceptable.
Dr Pullicino as Expert Witness
It is difficult to square Dr Pullicino’s strong and consistently expressed views over at least the last two decades with some of the answers he gave in court.
For example, in response to a question from the judge about what information he had available to him about this case in advance of seeing the patient, he explained that he’d read an article in LifeSiteNews, which – as it turned out – was headlined “UK hospital removes food, water from unconscious Polish Catholic euthanasia victim on Christmas Eve.” This was followed by an exchange with the judge which went like this:
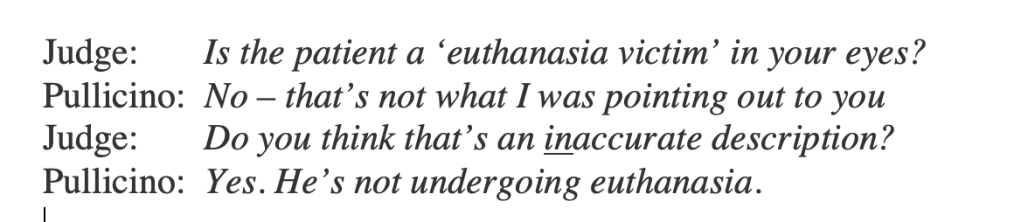
And yet from everything Dr Pullicino has written in the past, I would absolutely have expected him to see withdrawal of nutrition and hydration from RS as a paradigmatic case of “euthanasia” as he’s named it in the Catholic Herald, in the Catholic Education Resource Centre, and in his YouTube talk to Doctors For Life Ireland. A third of all NHS deaths (he’s said) are “euthanasia”. How could this one not be among them?
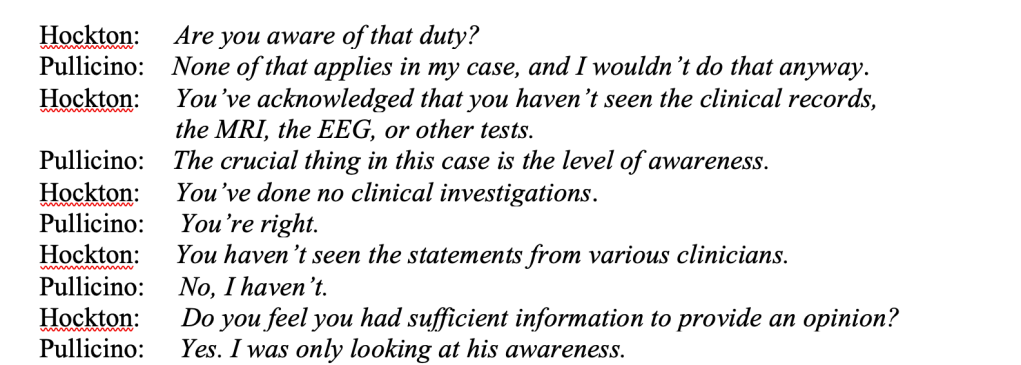
Then there was this exchange, under cross-examination from Andrew Hockton (counsel for RS via the Official Solicitor):

This doesn’t sound like the man who believes that “it is important to declare yourself” as a doctor with strong spiritual values; the man who said, “it’s really important as a physician to have your own yardstick and say: ‘That’s as far as I’m willing to go’”; the man who writes of the physician’s “moral centre” and “the absolute ethical imperative to save life”.
Patrick Pullicino is registered with the General Medical Council (GMC No. 1627457). According to their website, he’s been on the Specialist Register for Neurology since 2005 with a licence to practice since 2009: he’s also a recognised GMC trainer. The General Medical Council accepts that doctors have ethical values that inform their medical practice, but also requires that they act with honesty and integrity and within the guidance for good medical practice.
Figure 4: General Medical Council Guidance on “Personal Beliefs and Medical Practice” (downloaded from this GMC webpage here, in effect as of 22nd April 2013)

During the hearing Andrew Hockton (counsel for RS via the Official Solicitor) asked Dr Pullicino whether he had read the GMC Guidance on providing evidence as an expert witness: Pullicino said that he had not. “It may bear some reading”, said Hockton, and quoted from it:
“You must give an objective, unbiased opinion and be able to state the facts or assumptions on which it is based. If there is a range of opinion on an issue, you should summarise the range of opinion and explain how you arrived at your own view. If you do not have enough information on which to reach a conclusion on a particular point, or if your opinion is qualified (for example, as a result of conflicting evidence), you must make this clear.” (from “Acting as a Witness in Legal Proceedings”, para. 13 GMC)
The subsequent cross-examination, which was clearly an uncomfortable experience for Dr Pullicino, went something like this (as best I can report it, given that we are not allowed to record court hearings, so I have to rely on notes made at the time[3]).
This doesn’t reflect well on Dr Pullicino as an expert witness. He doesn’t appear to recognise that his opinion about RS’s diagnosis should be qualified – in part because he is (through no fault of his own) missing key diagnostic information, and in part because there is conflicting evidence (in the reports from other doctors) which he has not attempted to explain or understand in relation to his own findings.
Court of Protection Practice Direction 15A is aimed primarily at lawyers who instruct expert witnesses, so in this case it should have informed the actions of the legal team behind Charles Foster, who acted as counsel for the birth family, whose witness Dr Pullicino was. It sets out some rules concerning expert evidence, including the following:
- The expert’s report should provide: “objective, unbiased opinion on matters within the expert’s expertise, and should not assume the role of an advocate” (§ 4).
- An expert should make clear when they are “not able to reach a definite opinion, for example because the expert has insufficient information” (§ 6(b)).
I don’t agree with Pavel Stroilov’s assertion (in an article for Christian Concern) that Pullicino’s evidence “was severely criticised for not being a full expert report” (which it obviously wasn’t). Rather his evidence was criticised for being, as the judge said, “unqualified” (para. 25) in the sense that he failed to qualify his conclusion that RS was displaying behaviours indicative of the minimally conscious state, simply restating this without reservation, and without explaining the reasoning that led him to this position. He did not acknowledge any ways in which his own knowledge of RS’s medical condition might be limited or circumscribed in ways that could perhaps affect his assessment, nor did he attempt to explain why it might be that other experts considered RS to be vegetative. It is widely recognised that differentiating between the reflex movements of the vegetative patient and the purposeful movements of a person in a minimally conscious state (at the lower end) can be challenging, even for trained professionals with all the information at their disposal (see our article on the ‘diagnostic illusory’), yet Dr Pullicino seemed confident he’d achieved this with 3 minutes of video-recording. This was simply unconvincing to me, and (clearly) also to the court.
Dr Pullicino also declined (as evidenced above) to engage in any discussion of the ways in which his diagnosis of RS might or might not have been influenced by his Catholic values, and in particular by his oft-stated conviction that withdrawing clinically assisted nutrition and hydration would constitute “euthanasia”. Instead, incomprehensibly to me – having read his publications and listened to his lectures – he stated that RS is “not undergoing euthanasia” if food and hydration were again withdrawn, and that his own religious beliefs had no bearing at all on his approach to the evidence and on his “objectivity” as a doctor.
Reflections
From what I know from reading his professional publications, Dr Pullicino would have been a good witness in court for anyone wanting evidence about the ethics of continuing or withdrawing life-sustaining treatment (especially nutrition and hydration) from a Catholic perspective.
Instead, he found himself in court as an expert witness on a very different matter: whether a particular patient was correctly diagnosed as vegetative, or whether he was displaying behaviours indicative of the minimally conscious state. I don’t know (because I don’t have access to the court bundle which would surely have included his CV) what previous experience Dr Pullicino has of diagnosing where a patient falls along the spectrum of prolonged disorders of consciousness. Perhaps he is simply inexperienced in this quite specialist area, and mistook (as many people do) random reflexive movements for purposive ones.
In court, Dr Pullicino said several times that he wanted to “give the patient the benefit of the doubt”. I took this to mean that if there were any doubt as to RS’s diagnosis (although in fact, there wasn’t), then he saw it as beneficial to RS to proceed as though RS was conscious, which he took to mean continuing life-sustaining treating and ensuring to RS the opportunity for recovery and rehabilitation. On another occasion, he said: “I’m batting for the patient, because they won’t have a chance to do further tests if the court order goes through”. I got the impression that, for Dr Pullicino, what was most salient in this case was not in fact the correct diagnosis for RS (i.e. whether he was vegetative or minimally conscious) but that his focus was instead (as he said in the email) on his commitment to the view that “[t]here is no way he should be left to die”. The diagnostic claim advanced by Dr Pullicino seemed to me subordinate to his more fundamental ethical position that all human life matters and that no patient should have food and hydration withdrawn as long as it is effective in sustaining their existence. But that, of course, was not an argument that would have traction in court.
Why did Christian Concern proceed to court with such clearly inadequate evidence: did they believe they could help a desperate (birth) family and save RS’s life? Possibly. But it may also be that legal cases like this are pursued less with the expectation that the individual patient can be saved, and rather, as Jenny Kitzinger has said, “with the view that these cases (whether or not they are won or even ‘winnable’) are a valuable strategic way of carrying on and promoting a broader agenda.” The case achieved publicity for Christian Concern and the Christian Legal Centre and it adds to the overarching narrative they promote of a court system that is anti-Christian and an establishment that is against them. They have also used the RS case to advance pro-life claims and linked it with another of the cases they were involved in, the Alfie Evans case. The Christian Legal Centre’s Roger Kiska writes (here) with reference to both cases that “semantics aside, this is euthanasia” and (later) “state ordered killing”.
Why was Dr Pullicino’s evidence admitted to court when the paucity of this evidence must have been apparent to the court from an early stage? Counsel for the Trust (Vikram Sachdeva) submitted that Pullicino’s evidence was inadmissible and that there was no need for oral evidence from him. The judge, however, believed that the birth family was entitled to hear from the treating clinician and independent expert why Dr Pullicino was wrong (if he was). I could see his point, but would have wished that this had been possible outside of court in a round table meeting.
My over-riding sense having observed these hearings was that the Court of Protection had been hijacked and subverted in pursuit of an adversarial campaigning agenda that is alien to its usual practices and procedures. It was disappointing and somewhat demoralising to see this obviously doomed attempt to ‘rescue’ RS take up so much time and energy in the courtroom, when there is such a backlog of other important work for the court to do.
I hope those with oversight of the Court of Protection might consider how this sort of situation could be avoided in future. Perhaps there might be a more robust approach to eliciting, acknowledging, and respecting statements of conscientious objection among some doctors to particular (lawful) courses of action and an open consideration of the implications of this for their role as expert witnesses. In my experience, it is quite common for clinicians to have ethical qualms about removing nutrition and hydration from people who are not otherwise within hours or days of death, but this is something they may not feel comfortable expressing without support.
Perhaps, also, it might be possible to insist on the proper application of existing COP rules concerning expert witnesses: COP Rule 15.2 (Restriction on filing an expert report) and COP Rule 15.5 (which lists the actions to be done when a party applies for a direction to file expert evidence). With reference to Rule 15.2, I have observed several hearings at which parties have asked for permission to instruct an expert witness and the judge has refused (it was not considered “necessary”). Clearly no such permission was requested in this case, but I imagine that, if it had been, permission might well have been refused. Alternatively, if permission had been granted then, in accordance with Rule 15.5 it would at least have been clear to the birth family’s legal team that a proper letter of instruction should have been prepared detailing (for example) the questions the expert was expected to answer – and Dr Pullicino would also have been given access to all the relevant information on which to base his assessment of RS, which might have resulted in better quality of evidence from him.
Ultimately, however, if organisations like Christian Concern are willing to spend time and money on conducting their ‘pro-life’ campaigns via courtroom litigation, and can find experts willing to act for them, there may be very little the Court of Protection can do to prevent them.
Celia Kitzinger is co-director (with Gill Loomes Quinn) of the Open Justice Court of Protection Project. She tweets @KitzingerCelia
[1] I think this is a typo for either GCS (which stands for Glasgow Coma Scale) or for CRS (which stands for Coma Recovery Scale). I don’t know whether this error appeared in the original email from Patrick Pullicino, or whether it was introduced by the judge.
[2] In an earlier blog post, Jenny Kitzinger, co-director of the Coma and Disorders of Consciousness Research Centre, analysed a video clip of RS that was circulated on social media, explaining how it is that non-experts might read it as evidence of consciousness, but why – in fact – it does not demonstrate any behaviours inconsistent with a diagnosis of the vegetative state.
[3] Pavel Stroilov, who was also in court, has published a piece which includes a list of the questions he noted down as having been directed to Dr Pullicino (but not Pullicino’s answers to them). I recognise all of the questions he cites, but Stroilov’s wording and my own are quite different in ways that may be significant. For example, where I have “You’re an ordained priest – does that have any bearing on the objectivity of your views?”, Stroilov renders this same question as: “Are you an ordained priest? Would that affect your objectivity?”. Where I have “You’ve acknowledged that you haven’t seen the clinical records, the MRI, the EEG, or other tests”, Stroilov has: “You have not seen the clinical records, have you? You have not seen the results of the MRI, EEG, or any other tests, have you?”. In both cases, he has two questions where I have only one, and the use of tag questions – in his version, but not in mine – also adds to the sense of ‘barrage’ of interrogation. Without the recording, there is no way of knowing whether my version or Stroilov’s is more accurate, but I note that his rendition (which also omits Pullicino’s responses) certainly fits better with his claim that Pullicino was “machine-gunned with tough questions from two barristers and a judge, rarely given a split-second to answer” – which was certainly not my impression.
[4] This is factually incorrect in relation to English law. People in coma, vegetative states and minimally conscious states are ‘persons’ in English law.

Really interesting and important piece.
As a tangent, as a practicing Consultant Intensivist, I do not like using the word ‘coma’.
A coma is a deep state of prolonged unconsciousness in which a person cannot be awakened, fails to respond normally to painful stimuli, light, or sound, lacks a normal wake-sleep cycle and does not initiate voluntary actions.
A person can’t be in a coma unless they are not receiving any drugs that might impair their consciousness. This is not a common state for the average patient on ICU.
The normal state on ICU is that a patient is sedated
Sedation is NOT an ‘induced coma’ as I’ve heard some people say.
Generally patients should be interacting with ICU staff, with their sedation being the minimum required for their safety. Some conditions effectively require an anaesthetic, which is still not a coma.
The Richmond Agitation and Sedation Score is a good starting point of how to assess degree of sedation in ICU.
https://www.icudelirium.org/ is a good place to go for more resources
LikeLike
Is there some law or code about being an expert witness in court? Surely there must be? I have no problem at all with people holding all sorts of strong views, for religious or other reasons. But if I’ve read this one correctly what seems to have happened is that the doctor has tried to convince the court that his views are based on science, without disclosing his strongly held moral/religious beliefs. I don’t see any evidence that he disclosed these beliefs in court – have I missed that?
LikeLike
It’s hard to comprehend any professional being prepared to go into court so ill-prepared, knowing they would need to explain their findings in detail.
If his involvement was to present an ethical argument then that should surely have been made clear before getting into court.
LikeLike
Patrick PULLICINO je podľa mňa obetavý a láskavý človek, ktorý sám vychoval tak nádherne úspešne deti, nesťažujte mu život,nezasluzi si to.
****
Editorial note:
For non-Polish speakers, Google Translate renders this as follows:
In my opinion, Patrick PULLICINO is a selfless and loving man who himself has raised children so beautifully successfully, don’t make life difficult for him, he doesn’t deserve it.
LikeLike