
By Jenny Kitzinger, 29th March 2021
Editorial Note: See also Celia Kitzinger’s blog post about the role of Dr Patrick Pullicino, the expert witness in this case.
Family videos of severely brain injured patients play a crucial role in the public domain. They feature in court proceedings, fund-raising drives, social media and the national and international press. They are used to contest patient diagnoses and to fuel disputes about life-sustaining treatment.
During the pandemic, videos have been hugely important for families. Many have been unable to see patients face-to-face. Families have often had little or no opportunity to be at the bedside. This means they have limited experience of what relative is like given their clinical condition and are unable to sit with clinical teams in person to reflect on and come to terms with their loved one’s diagnosis and prognosis.
In this blog I discuss how video featured in a recent Court of Protection hearing, and in the public controversy that followed. I place this in the context of previous controversies, and ask what the courts can do, in future, to respond to the deployment of video-recordings in cases of treatment dispute.
The case of RS
A middle-aged Polish man, known to the English-speaking world as “RS”, was the subject of several contested Court of Protection hearings during December 2020 and January 2021 before Mr Justice Cohen, and before judges in the Court of Appeal (although permission to appeal was refused)[1] . There were also at least two failed attempts to put the case before the European Court of Human Rights. The key issue was whether continuation of his life-sustaining treatments – specifically, clinically assisted nutrition and hydration – was in RS’s best interests.
The applicant Trust (University Hospitals Plymouth NHS Trust, represented by Vikram Sachveda QC) believed – in common with the treating team and RS’s wife (and children) – that continuing life-sustaining treatment was not in RS’s best interests. His niece, speaking also for his mother and sisters and other members of the ‘birth family’, believed that it was in his best interests to continue treatments, and that this is what he would have wanted. The ‘birth family’ was represented by a changing cast of lawyers including Bridget Dolan QC, David Lock QC, Charles Foster, James Bogle and Bruno Quintavalle. Lawyers acting for RS by his litigation friend the Official Solicitor included Andrew Hockton and Katie Gollop – and the Official Solicitor herself (Sarah Castle) was in court for one of the hearings. The Official Solicitor’s view – like that of the Trust and RS’s wife – was that continuing life-sustaining treatment was not in RS’s best interests.
RS eventually died on 26th January 2021 after his clinically assisted nutrition and hydration had been withdrawn and reinstated on several occasions while yet another court application concerning him was in preparation.
The dispute about RS’s treatment spread well beyond his treating team and his family. It spilled out from the bedside to the courts and into the public domain and then back again through the legal system (including the Court of Protection, the Court of Appeal, and the European Court of Human Rights). There were many powerful forces at play, and a huge clash of religious and cultural values. The persuasive power of video was a crucial lightning rod in how the story played out.
“Is this what a patient in a coma looks like?” The RS video
RS had been living in England, with his wife and children, since emigrating from Poland in 2006. On 6th November 2020, he had a cardiac arrest and was without oxygen to his brain for at least 45 minutes. Inevitably, he had significant brain damage as a result. The treating team, and an independent specialist appointed by the Official Solicitor (Dr Dominic Bell, Consultant in Intensive Care Medicine) diagnosed him as being first in a coma and then in a vegetative state and, in consultation with his wife, decided that continuing treatment was not in his best interests.
The patient’s birth family – his mother, sisters and niece – disagreed. They believed that (irrespective of his diagnosis) RS would never have wanted the feeding tube withdrawn due to his strong Catholic faith. (For discussion about the potential role of his religious faith see this report from the Anscombe Bioethics Centre.)
Although they initially accepted the diagnosis (at the first Court of Protection hearing), the birth family subsequently also claimed that he was not ‘vegetative’ but in a ‘minimally conscious’ state and that his prognosis was therefore much better than his doctors were predicting. Their changed position about RS’s diagnosis was – in their view – supported by video clips of RS.
During a brief visit to the bedside (ostensibly to ‘say goodbye’), RS’s niece made videos of RS in his hospital bed which purported to show him responding to her. Video clips were shown to other neurological experts and presented to the court. One also found its way onto social media and then into Polish mainstream media outlets, where it attracted a great deal of comment. The video was made and distributed without the consent of RS’s wife or the Official Solicitor representing him and is in breach of the Court of Protection’s reporting restrictions. For that reason I do not link to it here.
Figure 1: Transcript of the dialogue recorded on the video of RS
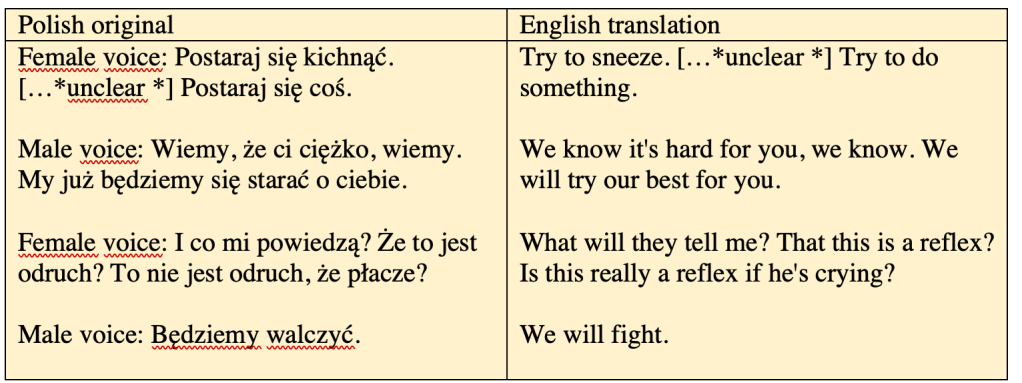
In the video clip circulating on social media, the patient’s eyes are open, they move and blink. The handheld camera (presumably on a phone) is slightly adjusted to look directly into the patient’s face. He sniffs, blows out through his mouth and makes facial expressions. One interpretation is that he is about to cry: that is certainly how it looks to me, and his eyes seem to be watering. A colleague, however, who saw the video without being able to understand the Polish says this is not what she saw (and it may not be the self-evident ‘reading’ to all viewers).
For anyone with experience of working with patients in ‘disorders of consciousness’ (the generic term covering coma, the vegetative state, and the minimally conscious state), this is very clearly not a patient in a ‘coma’ – because his eyes are open.
However, there is no evidence at all to suggest that he is in a minimally conscious state as opposed to vegetative. Everything about his behaviour in that 18 second clip is compatible with a vegetative diagnosis – including, in particular, his eyes being open, breathing on his own without artificial ventilation, watering eyes, eye movement, and facial grimacing.
By contrast, for the majority of members of the public who commented on the video, the clip provided evidence that RS was not vegetative (though this was often equated with not being in a coma or, indeed not being brain dead). They drew on the very behaviours characteristic of the vegetative state as evidence that he was not vegetative (e.g. breathing on his own) – and they read into the video behaviours that (for professionals with experience in this area) absolutely cannot be evidenced by it (e.g. claiming that it showed RS reacting to relatives).
The text beneath the video when it was posted on YouTube asserted that UK doctors had misdiagnosed RS and it called on viewers to campaign for Polish government intervention and the return of the patient for ongoing treatment in Poland.
“Doctors, after three days, wanted to kill him while he was still in a coma. They said he would never wake up. However, he woke up, breathes on his own, reacts to his relatives. The hospital plans to kill him by starvation and dehydration, and the family fights desperately to save him.”
The YouTube video had over 100,000 views within 48 hours before being taken down after the Official Solicitor contacted the legal office of YouTube, provided them with a copy of the transparency order and requested removal of the video. Even after that, however, the video continued to circulate widely in a tweet on Twitter where it garnered another 160,000+ active views (people clicking on it) and was seen by many more as it was embedded to be played on a loop without any need to click on it[2]. The video was picked up by several Polish press reports and played on Polish television. Tweets about the video tagged high profile political, media and religious figures, including the Polish Embassy, the British Embassy in Warsaw, the British Prime Minister, the Queen of England, and the British Foreign Secretary, Dominic Raab. Other tweets targeted the NHS and the hospital in which RS was being treated.
What is clear from the comments is that viewers were horrified at the threat of ‘starvation’ and the majority saw the video as compelling evidence of RS’s consciousness and as proof that his doctors had misdiagnosed him (see Figure 2).
Figure 2 Tweets about RS
Note: Some details in the following tweets are blanked out, such as where a patient’s name is given and I have excluded the image of the video that was often attached.
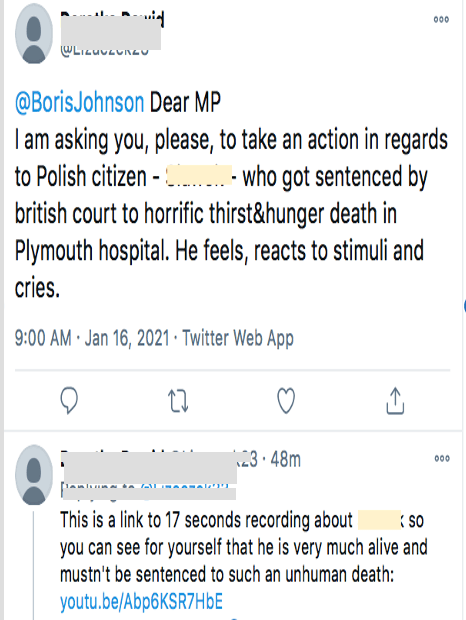


To many viewers, it seemed self-evident that RS was not unconscious – as claimed by the doctors who had diagnosed him. If a person is correctly diagnosed as vegetative, they are – by definition – unconscious and have no awareness of themselves or their environment: they do not respond to stimuli.
But those circulating the video declared that a viewer can ‘see for yourself’ that the patient is aware and responding, pointing out how his eyes blinked or moved. An email appeal reached me asking that I help save RS’s life: “As you can see from the dramatic video [he] is responsive! Here is the dramatic video”.
Claims were made that this man could clearly experience emotions and even understand his situation. Assertions included that he was crying because of the pain (or anticipated pain) of having food and water withdrawn. It was all obvious to the naked eye. “He is not unconscious, he pleads and pleads with his face” wrote one; “His face of pain and tears is clearly visible” wrote another. (These last two tweets were written in Polish – the main language used in this online debate. I relied on Google Translate and the help of a Polish colleague to translate them.)
Patient Videos in the Public Domain
The use of patient videos, initially circulated on social media and then becoming news events and fuelling coverage in their own right, has become a familiar weapon in the public battle for hearts and minds in treatment dispute cases.
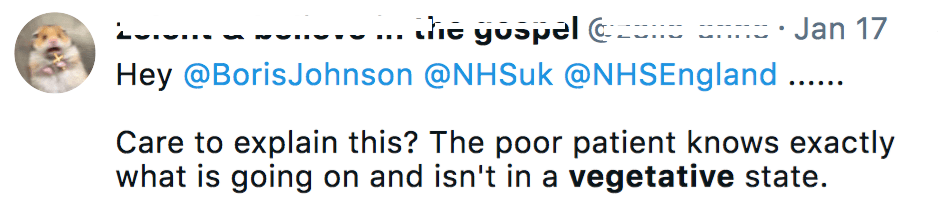
Videos were used in the battle over the diagnosis and treatment of vegetative patients such as Terri Schiavo (in the USA in 2005) and Vincent Lambert (in France in 2015) – where family members were at loggerheads about the right way forward. They have also featured in a series of cases in which there have been disputes between clinicians and parents around the treatment of children such as Alfie Evans (in England in 2018) (see Fig 3). It is becoming increasingly important to understand how and why such videos circulate and how they might be deployed in the course of end-of-life decision-making.
Figure 3 – Media coverage showing the power of the videos
So how do such videos come to be made, why are they so powerful? And what was the context in this case?
The creation and use of videos of RS in court
At a Court of Protection hearing on 15th December 2020, Mr Justice Cohen granted a declaration that it was not in RS’s best interests to continue to be given life-sustaining treatments, including clinically assisted nutrition and hydration (CANH) and that such treatment could be lawfully discontinued (a position supported by RS’s wife and pre-adult children). Treatment was withdrawn on 16th December 2020, but reinstated on 18th December when RS’s birth family filed an application for permission to appeal that decision. Permission to appeal was refused on 24th December 2020 and treatment was again withdrawn. The following day, members of RS’s birth family visited him in hospital and made the videos – which in turn prompted another court hearing on 31st December 2020.
The videos were created after the birth family asked an experienced neurologist, Professor Pullicino, apparently located via Christian Concern, to give his opinion about RS. They did so without seeking permission from RS’s wife, from the hospital, or from the court. Professor Pullicino instructed RS’s niece, during a FaceTime consultation as to what to do in order to try to elicit a response from him and how to make the video clips. It is unclear how long the niece’s visit to RS lasted or the duration of the video recording that was made, but the clips submitted to court in a hearing before Mr Justice Cohen on 31st December 2020 totalled about 3 minutes. The longest is 41 seconds.
During the hearing, Professor Pullicino testified that the clips provided evidence that RS either was or might be (his evidence was confused) in a minimally conscious state, and that, either way, this meant a much better prospect for his recovery than had been suggested by the treating clinicians or independent expert. He claimed that the video clips suggested an emotional response from RS to the presence of family members, and that he moved his eyes in their direction when they called his name.
The significance of the diagnosis – as either vegetative or minimally conscious – is that an MCS diagnosis would have changed RS’s prognosis to include the possibility of recovery to a level he might have wanted (according to evidence of his wishes provided by his wife). His birth family were keen for him to be moved to Poland and treated there, and the Polish Ministry of Foreign Affairs and the Polish Ministry of Justice offered to provide transport and treatment to enable this.
The video clips were not shown in court at any of the hearings, but by the time of the 31st December hearing they had been examined by the treating clinician and the independent expert neurologist, appointed by the Official Solicitor. These doctors, in contrast to Professor Pullicino, had previously reported that RS was in a coma and showing signs of becoming vegetative (at the time of the first hearing) and then that he had moved in to a vegetative state (by the time of the second hearing). They had never seen any evidence that RS was in a minimally conscious state. Nothing in the video clips changed the views of the treating clinicians or the independent expert that RS had been in a coma and was now in a vegetative state. Subsequent re-examination of the patient by the expert neurologist appointed by the Official Solicitor again found him to be in a vegetative state.
The judge at the 31st December 2020 hearing (revisiting questions raised from the 15th December 2020 hearing) concluded that “there has been no improvement in RS and no basis at all to change my decision that it is not in his best interests for life-sustaining treatment to be given“. He went on to reject the request for RS to be moved to Poland because, among other things, “there is no suggestion that any treatment or care can be provided overseas that could or would not be provided in UK if it were in his best interests“. Moreover, “it is unthinkable that he should be moved against the wishes of his wife and children“.
Diagnosis at the margins of conscious and unconscious states
To understand the problem with Professor Pullicino’s interpretation of the videos (and with public interpretation of the video circulating on social media), it’s necessary to understand how diagnosis is established according to best practice and clinical guidelines. The key guidelines for patients with disorder of consciousness in England and Wales have been drawn up by the Royal College of Physicians [RCP] and it is here one can find definitions of, and clarifications of the distinctions between, coma, vegetative and minimally conscious states.
The word ‘coma’ is often used in a very loose way in everyday discussions and sometimes interchangeably with ‘vegetative’ but it has its own distinctive clinical definition. The RCP guidelines state that a coma is: “A state of unrousable unresponsiveness, lasting more than 6 hours in which a person: is unconscious and cannot be awakened, fails to respond normally to pointful stimuli, light or sound, lacks a normal sleep–wake cycle and does not initiate voluntary actions” (RCP, 2020, p25). Comas rarely last more than a few days or weeks after which a severely brain injured patient who does not die will often move into a vegetative or minimally conscious state. Distinguishing between these two latter states requires expert diagnostic skills.
A defining feature distinguishing the vegetative state [VS] from the initial coma is that patients move into having sleep-wake cycles. They not only open their eyes when ‘awake’, but their eyes roam about, and they may turn their heads, make facial expressions, and even cry or laugh. Vegetative patients can also have a grasp reflex (they will squeeze a hand holding theirs), a startle reflex to noise, and they can turn away from painful stimuli. All these features are compatible with the clinical diagnosis of the vegetative state (RCP, 2020)
The minimally conscious state [MCS] can, at first glance, look rather like the vegetative state but the patient with some minimal consciousness may persistently focus on and follow a family member with their eyes, may cry or laugh appropriately (rather than at random) or ‘localise’ and do “purposive motor behaviour” (e.g. rather than reflex retraction from pain, the patient may act to push away the source of pain) (RCP, 2020).
Given how the difference between VS and MCS is defined it is obvious that one-off observations of something as subtle as eye movement or facial expression without capturing the context or engaging in rigorous repeat testing could result in a confusion of the two states (with error in either direction, i.e. VS patients might be taken to be MCS or vice versa).
That is why clinical guidance from the Royal College of Physicians makes clear that interpretation of apparent ‘responses’ (or the lack of such responses) must be approached with great care. Patients’ behaviours need to be understood in the context of other clinical knowledge of that individual and “When assessing responsiveness several complementary sources of behavioural observations should be used”, including, for example, routine observations recorded within notes, made by staff (RCP guidelines, 2020, Annex 2). At the same time, it is vital that efforts at refining diagnosis should incorporate observations (and recordings) by family and close friends, because they “are often present over prolonged periods and because many patients respond at an earlier stage with familiar people.” [my emphasis] (Annex 2). The interpretations of family and friends should not, however, be necessarily taken at face value, but explored in dialogue with the clinical experts’ interpretations and structured testing processes.
The weaknesses of Professor Pullicino’s interpretation of the videos include his reliance upon what the patient’s niece conveyed about her interpretation, such as how she felt that RS’s behaviour ‘changed’ when she entered the room (a slightly odd statement given it is unclear how she could assess what his behaviour had been before she entered). In addition, Pullicino offered a (re)diagnosis without having read any medical reports about RS, without having spoken to any member of the treating team, and without having seen the MRI or EEG scans. He was not privy to information about whether RS’s eyes had a tendency to roam to the right or the left, and had insufficient evidence or time to make a meaningful assessment of whether or not his eye movements in relation to his niece might be significant. He had not reviewed the patient’s notes or engaged with the observations of staff involved in examining or caring for him.
He also did not have the benefit of engaging with RS’s wife and her experience at the bedside, despite her being the person most familiar to RS before injury. She had been his “constant companion” at the hospital and provided the value of having been “present over prolonged periods” (as per the RCP guidelines). It was unclear whether Professor Pullicino was even aware of the estranged nature of the relationship between the niece and RS. He even incorrectly referred to the niece as RS’s daughter at one point and had to be corrected in court. As the judge recorded in the judgment:
“I remind myself that RS had not seen his niece or her family for nearly a decade. I am not sure whether Dr Pullicino was aware of that fact. To found his opinion as he did on the basis of what he believes to be an emotional response to someone who may have been almost a stranger seems a huge leap of faith.” (para. 29)
This is the context within which the video released to the public needs to be understood. I cannot be sure whether or not the 18-second video was one of the ten short clips that constituted key evidence discussed in court on 31st December 2020. However, this video is completely unconvincing from a clinical perspective – there is nothing in it to suggest the patient has any consciousness and, if it were part of the evidence presented, it would not have had any purchase for all the reasons discussed above. However, the very weakest of evidence in court can be the most compelling in the public domain.
Undermining trust in diagnosis
The fact that the video of RS released via social media gained such attention – and seemed so shocking to viewers – is in part because people think they know what a coma or vegetative state looks like. After all, we have all seen the static body in the bed, immobile face and closed eyes which circulate widely on TV and in film (Wijdicks and Wijdick, 2006; Kitzinger 2014). On the rare occasion that eyes are shown open, they are fixed and unmoving. Indeed, in one otherwise well-researched portrayal in the TV series “Casualty” (see Fig 4), the unblinking and unmoving response to having a hand waved in front of her was a way in which we were introduced to a vegetative patient and the scene was set for understanding that she was entirely unconscious.
Figure 4 – A still from the TV series “Casualty”
It is not surprising that anyone viewing the video clip of RS, or indeed actually visiting a vegetative patient in person, may feel that the patient fails to conform to expectations and therefore must have some level of consciousness. There is a vast gulf between typical cultural representations of the vegetative state, and its clinical definition.
Over and above the issue of media/cultural stereotypes is the question of visceral human experience. Emotional investment and common-sense everyday experience prime us to interpret facial expressions, eye gaze and physical movement as meaningful. The declaration of the woman speaking in the RS video suggests she is absolutely genuine in her feeling that the patient is experiencing emotions despite clearly having been offered alternative clinical explanations: “What will they tell me? That this is a reflex? Is this really a reflex if he’s crying?”
The question she asks is raised by many of the families my colleagues and I have interviewed as part of our work at the Coma and Disorders of Consciousness Research Centre.
One man, for example, commented that even after several years he is not sure whether his brother is vegetative or minimally conscious. He says: “when you’re looking at somebody and they’re looking straight at you, in your eyes, and they start crying you don’t not take any notice of this. I don’t care what anybody says really” (see Figure 5).
You can see many other examples of how families of severely brain injured patients may struggle to make sense of what they see here in a healthtalk.org resource we developed to support families.
Video as a tool to give ‘a face’ to the patient and assert humanity
The power of such videos goes well beyond challenges to diagnosis. Videos of patients can also be mobilised as part of a broader challenge to the way in which patient care is approached (e.g. in a particular healthcare or legal system). It is not surprising to find that some of the same organisations and individuals (especially from Catholic organisations) have been involved in many of these cases – this is certainly true in the Schiavo case in the USA, the Vincent Lambert case in France, and in both the Alfie Evans and RS case in the UK. This is an international issue.
In an interview on “Pro-Life” weekly about the Vincent Lambert case, both Bobby Schindler (Terri Schiavo’s brother) and Tom Shakely from the Terri Schiavo Life & Hope Network (based in the US), highlight the importance of videos. They assert their view that clinically assisted nutrition and hydration is not ‘life-support’ but rather is basic care, and that these patients are not ‘end-of-life’. Video images, they point out, are powerful because they put a human face to the patient, and disrupt the idea that he or she is dying, or should have ‘care’ withdrawn.
“The phrase ‘sunlight is the best disinfectant’ is common in law…when you see the humanity of someone like Alfie Evans or Vincent Lambert …it’s incredibly difficult to look him in the eye and to say this is a man who is dying or this is a man who doesn’t deserve basic care”.
Bringing these images ‘into the light’ challenges the false media imaginings of the patients at the centre of these disputes as frail husks hooked up to multiple machines. It challenges fallacious fantasies of simply ‘pulling the plug’.
From the point of view of those promoting life-sustaining interventions, videos of the patient in their brain-injured state re-centre the individual’s humanity.[3] In many ways, the explicit claims associated with patient videos (that the clips provide evidence that the patients are at least partially conscious) is irrelevant from this perspective. The claim is that all life matters and that no patient should have CANH withdrawn as long as it is effective in sustaining their existence.
The videos in this sense have significance far beyond the individual case and their use allows these patients to become icons, personifications of struggle beyond any one individual; the faces of Terri Schiavo and Vincent Lambert for example, and now of RS, are used to illustrate (among other things) the dangers of ‘state-controlled medicine’, the failings of a ‘barbaric state’, and the unethical nature of medio-legal frameworks developed outside the tenets of specific religious faiths. It may even be that involvement with such cases is pursued (by organisations such as Christian Concern) less with the expectation that the individual patient can be saved, but rather with the view that these cases (whether or not they are won or even ‘winnable’) are a valuable strategic way of carrying on and promoting a broader agenda.
Reflections
As far as videoing patients is concerned, the genie is definitely out of the bottle. Families will continue to video patients and circulate clips on social media, whatever doctors and courts tell them and such videos will continue to engender controversy. This is made possible by the ubiquity of the phone-camera, the proliferation of social media, and promoted by the rising distrust of expertise and access to international lobby networks.
Family members take videos of patients for a wide variety of reasons with or without the knowledge of the patient’s clinical team (or even other relatives). They may film the patient to assist with, or to challenge, clinical diagnosis; to share what they witness with distant family; or in order to provide ‘evidence’ to another clinician from whom they seek advice. Those not able to attend in person can simply record calls with the patient on video-platforms. Such recordings may be entirely an individual initiative or they may be encouraged to make clips by organisations keen to help them to access alternative clinical expertise or to draw public attention to what they see as a violation of patient’s rights – with the deliberate endgame of using it for campaigning purposes.
In general, it is neither feasible nor advisable to attempt to stop families taking videos of patients. There may be occasions when chaperoning a one-off visit from a particular relative might be possible where other close family believe this might be necessary to avoid inappropriate filming (i.e. not in the best interests of the patient). An alternative approach is to proactively work with family members to film the patient and discuss videos with them (as is often done in neuro-rehabilitation settings) and to ensure that, during any zoom calls, an experienced staff member is there to help family interpret what they see.
It is extremely hard to police what is done with such film once it has been made and is stored on a relative’s mobile phone. It can be easily and anonymously uploaded to social media and the fact that the general public may find such videos shocking and compelling ‘evidence’ can ensure rapid and extensive circulation. When a case is of interest in a different jurisdiction, the threat of contempt of court may also have little impact on mass media circulation (unless the media outlet has UK outlets/staff). It might be possible, however, for judges – alert in advance to the possibility of the public release of videos – to address this issue during a hearing. They might, for example, ask family members in court whether they have shared such clips, and remind them of (or negotiate with them) the terms of the transparency order. It is also important that legal teams act swiftly to have videos taken down where they breach the transparency order: it may be useful for lawyers working on such cases to develop an information resource that can be quickly accessed by lawyers acting to protect the privacy of their clients, which will provide a guide to contacting the relevant offices of the main social media platforms such as YouTube, Twitter and Facebook and their policies on the removal of items which breach their privacy and any existing court orders.
More fundamentally, of course, nothing will change without a broader public understanding of disorders of consciousness, better media representation of these conditions and a wider engagement with the clinical, ethical and social challenges. Even then, fundamental clashes in underlying values and beliefs will continue to ensure that some disputes will always become major public battles, whatever effort clinicians, families and courts make to try to come to collaborative best interests decisions.
Jenny Kitzinger is Professor of Communications Research at Cardiff School of Journalism, Media and Culture. She also co-directs (with Celia Kitzinger) the Coma and Disorders of Consciousness Research Centre and runs a regular short online course on “Media, Culture and Coma”. She tweets @JennyKitzinger
Illustrations by Tim Sanders
[1] The published judgments are:
- University Hospitals Plymouth NHS Trust v RS & Anor [2020] EWCOP 70 (15 December 2020)
- Z v University Hospitals Plymouth NHS Trust & Anor (Rev 3) [2020] EWCA Civ 1772 (23 December 2020)
- Z v University Hospitals Plymouth NHS Trust & Ors (Rev 1) [2020] EWCOP 69 (31 December 2020)
- Z v University Hospitals Plymouth NHS Trust (NO 2) [2021] EWCA Civ 22 (13 January 2021)
- RS, Re [2021] EWCOP 6 (18 January 2021)
[2] When the video of RS was released on YouTube it quickly ‘went viral’ – even though both the YouTube channel on which it was located, and the Twitter-embedded format were started on the very day of release with no established channels or followers (presumably a device to avoid identification given the dubious provenance and unlawful use of the material). However, there were well-established social media networks from particular value bases, such as Catholic networks, who picked up on the video. (One re-tweeter has twitter handles such as #BabiesLivesMatters and images of the Virgin Mary and other tweets on their timeline suggest strong traditional Catholic values). The video also generated interest from a wider constituency due to the ‘shocking’ nature of the moving images and the story behind it.
[3] Of course, those who believe life-sustaining interventions should stop may take a very different view about what it means to ‘see the humanity’ of an individual. Vincent Lambert’s sister, for example, has spoken out about the dehumanising appropriation of images of him after his injury, circulated without his consent; and she has spoken about how much he would have hated this and wanted to be remembered and connected to his ‘humanity’ via his own beliefs and autonomy. ‘La soeur de Vincent Lambert reagit au novel arret des soin”, L’union’. L’union, 3/7/2019) Interestingly also while RS’s birth family evidently saw the videos as a powerful endorsement of their view treatment should continue this was not the only reaction from people who encountered the images on twitter. One person, for example, commented how distressing it was to repeatedly encounter the video of RS looping on her timeline, and commented that, to her, it showed a man who was suffering pain and indignity, and should be allowed to slip away and be at peace.

10 thoughts on “Seeing is Believing? Patient Videos in Life-Sustaining Treatment Disputes”