
By Upeka De Silva, Rhiannon Snaith, Claire Martin and Jenny Kitzinger
Update, 14th December 2021: The judgment has now been published here: Cambridge University Hospitals NHS Foundation Trust v AH [2021] EWCOP 64 (13 December 2021) It includes information from court documents not read out during the course of the hearing and we have taken the opportunity to make some corrections to this blog post.
Introduction by Celia Kitzinger
A woman in her 50s, AH, has been an inpatient at Addenbrooke’s Hospital, Cambridge, since the end of December 2020, where she was admitted, on an emergency basis, suffering with severe symptoms of Covid-19. She no longer has Covid-19 but the virus has left her with extensive and serious brain damage. She’s in a minimally conscious state.
The question of whether it is in AH’s best interests to continue to receive mechanical ventilation was addressed back in August 2021 by Mr Justice Hayden (blogged here), who decided that it was not. He said: “I make it clear that ventilation should be discontinued by the end of October 2021”. The full judgment is here: Cambridge University Hospitals NHS Foundation Trust v AH & Ors (Serious Medical Treatment) [2021] EWCOP 51).
Her family appealed and the Court of Appeal found in their favour.
However, the appeal was not granted on the basis of any of the four substantive grounds of appeal: (1) that Hayden J had given insufficient weight to AH’s wishes as recorded on the ReSPECT form; (2) that he’d failed to appreciate the importance of her religious and cultural values; (3) that he’d not adequately considered her past and present wishes and feelings; and (4) that he’d failed to give sufficient weight to her Article 2 right to life. All those grounds of appeal were dismissed.
The appeal was allowed on the basis of procedural unfairness, relating to a visit from Mr Justice Hayden to AH, after the hearing had concluded. (For an account of the Court of Appeal hearing see this blog post, and you can read the full judgment from the Court of Appeal here: Re AH (Serious Medical Treatment) [2021] EWCA Civ 1768).
This meant that a re-hearing was necessary.
Following a relatively short ‘directions’ hearing on 29th November 2021 (blogged here), there was a hearing before Mrs Justice Theis on 7th and 8th December 2021. This blog post offers some reflections on that hearing from four observers and is written in advance of the judgment.
Counsel were Simon Miller of Harcourt Chambers for the family, acting pro bono through the Bar Pro Bono Unit, Nageena Khalique QC for AH via the Official Solicitor, and Katie Gollop QC for Cambridge University Hospitals NHS Foundation Trust.
An updated expert medical report on AH (by Dr Chris Danbury) was now before the court. His findings were clear. After almost a year in intensive care, there was no prospect that she would improve further. She would never be able to live without mechanical ventilation. She would never emerge from the minimally conscious state. There was, in his view, evidence of deterioration since he had last assessed her in August 2021 and AH is now in a terminal decline of consciousness. She is dying.
This was also the view of those treating her. Evidence was given in court by two treating consultants, Dr A (Consultant Intensivist) and Dr B (Consultant Neurologist), and by Ms C (Matron of Adult Critical Care).
The family view was radically different. Three of AH’s children and her sister gave evidence of having seen slow improvement in AH’s condition in the four months since August 2021. They see AH as more alert and aware, and as more able to communicate with them. They provided videos of their interactions with AH which they considered illustrate that improvement. Dr Danbury had reviewed this videos but does not see them as providing evidence of improvement in either her physical or cognitive function. (We’ve blogged before about the use of videos as court evidence, and the differences between families, experts and others in what is “seen” in them.)
There is, then, a very stark difference between clinicians and family in how they see AH.
The Trust position (now supported by the Official Solicitor) is that withdrawing ventilation under controlled conditions with AH’s family around her in a peaceful and prayerful atmosphere is in her best interests. The alternative may well be, in their view, a sudden death unattended by family. In Dr Danbury’s view, a catastrophe will occur at some point “and is likely to be sudden, unexpected and most likely without any opportunity for her family to get to the ICU in order to be with her while she dies“.
The family position is that it is in AH’s best interests to continue to receive mechanical ventilation. They believe she is showing signs of improvement and that she wants them to “fight for her“.
Four observers reflect on the hearing, bringing a range of different perspectives and experiences to their descriptions of what they witnessed in court.
1. Family testimony: Relieving the burden, by Upeka De Silva
I observed incredibly brave family members giving powerful testimony in support of what they believe their mum (or sister) would want.
In doing so, they did not hold back or censor what they had experienced in hospital. Although they accepted that she had generally had excellent care, they also voiced their frustrations about what they’d experienced as poor practice. It must have been cathartic to be able to speak out about it in this public and respectful setting.
[Amended text from here to end of this section, 14th December 2021] Before reading the judgment, my primary concern was that their feedback should be heard and valued not just by the Trust in this case but by others too, so that their experiences could be fed back with a view to improving practice.
Reading the judgment (especially paras 26, 33, 39, 89) really brought home to me – more than in the court hearing itself – that specific and detailed evidence was provided about the excellent care that AH had received while being ventilated for over 300 days.
Providing this level of care during a pandemic is particularly noteworthy and it is useful that this has been made public.
It is deeply unfortunate that the family still experienced distress about AH’s care. I appreciate it is not easy, but I am always hopeful that families and clinical teams can find ways to work together in the best interest of the patient.
Taking the burden from families
The barrister for the Trust (Katie Gollop) rightly reassured the family member who struggled to answer a question about what his mum would want, that one of the benefits of having the case heard in the Court of Protection is that it passes the responsibility of making the difficult decisions to the judge.
This is not to minimize the immense burden of duty that families must feel when giving evidence and advocating for a loved one, but it must provide some relief.
With this in mind, I would like more to be done to alert families to this valuable avenue of support when faced with disagreements about life-sustaining treatment decisions and end-of-life care.
Research shows that families often consider court hearings to be a deterrent to pursuing what they believe is right for their loved one. But here, as in other reported cases, it’s clear that for this family the court hearing gave them the reassurance that they had done everything they could possibly have done to fight for their mum.
The importance of advance statements
My take home message from this hearing, as in so many others in the Court of Protection, is that we should all prepare for possible future lack of capacity.
We can write down what makes our life worth living – and describe the circumstances under which life would not be worth living for us – so that if we become incapable of making and communicating decisions for ourselves, our family and all those caring for us, can hear our voice.
Documenting our preferences in this way, using an Advance Statement, in a calm and thoughtful manner, rather than having our wishes interpreted by clinicians, gives us the opportunity to comprehensively convey what it is that matters to us and what it is that we are willing to endure.
It was argued at the Court of Appeal (but not during the re-hearing) that AH’s preferences were in fact documented in a ReSPECT form. However, in para 46 of the Court of Appeal judgement it was held that the ReSPECT form:
“is directed, as is clear from the title, to emergency care and treatment. It is not directed to long-term treatment and so provides very little assistance to whether AH would want treatment to continue in her current condition which is very far from an emergency.”
Both a ReSPECT form (for emergencies) and an Advance Statement (for a much wider range of possible situations) are invaluable tools which enable individuals to get the treatment and care that is right for them while also supporting clinicians to make genuinely person-centered best interest decisions.
If AH had completed an Advance Statement explaining her religious, cultural and family values, her family may not have had to endure as many grueling questions about she would have wanted.
Even though they cannot demand a clinically inappropriate treatment, having written evidence of AH’s wishes, would have made the family’s powerful evidence even stronger.
Free Advance Statements and Advance Decision forms can be found at: www.mydecisions.org.uk
Upeka de Silva is Policy Officer for the charity, Compassion in Dying. She tweets @de_upeka
2. “What would I want for myself?” Facing up to burdens of treatment, by Rhiannon Snaith
This was the first time I’ve observed a Court of Protection hearing. It’s very different from what I’d seen in criminal courts (when completing work experience with a local newspaper). It was very intense, and you can’t help but get emotional and think “what would I want for myself?” or “what would I do if this were my loved one?” and go back and forth in your mind.
What really struck me about the case was that it gave me information about the potential burdens of treatment, giving me tools for thinking about the question “what would I want?” It made me confront some issues which I hadn’t really faced before, and maybe that few of us consider in depth.
Usually, you just think of being in Intensive Care as being ‘out of it’, but the doctors in this court hearing really described how being mechanically ventilated might feel for this patient who is in a minimally conscious state and has many other complications (e.g., paralysed, muscle wastage and severe neurological deficits).
Sometimes, it felt as though the doctors could be emphasising the burdens of ICU treatment to persuade the family to agree to letting the patient die – but that doesn’t stop their accounts of the potential burdens from being true.
The intensivists who gave evidence explained that Intensive Care was accepted and justified as a temporary measure if it helps stabilise a patient and give time for assessment and/or recovery – but they clearly did not see it as a humane long-term solution. Nor is it a practical one because, as the independent expert commented, “in intensive care, generally if you are not getting better then you are getting worse”.
The concern in this case was that the patient had been mechanically ventilated for almost a year and given her severe brain injuries and dependence on long term ventilatory support, combined with her specific and complex care needs, there was no prospect of her ever leaving ICU.
The treating team felt she was deteriorating and was very likely to die soon (potentially in a sudden and uncontrolled manner). All three clinicians involved in her care gave evidence that emphasised the burden of the treatment when there was no balancing benefit of recovery. It was also clear that all three were personally distressed by witnessing, or being involved in, what was done to this particular patient.
One of the treating doctors talked about ICU being a “dehumanising” environment for patients and referred to research showing that people who recover sufficiently to report on their experiences can be left with Post Traumatic Stress Disorder.[i]
Another doctor involved in treating this patient became quite emotional describing what was done to AH, outlining the distress of desaturation, having to be turned every few hours, and the intrusion of personal care associated with double incontinence. He said that, when there was no hope of recovery, “we know that many people in this situation do elect not to continue with the treatment that continues their life.” In this case, the situation was made worse because she might not understand what was being done to her, and damage to her memory meant she could not even recognise her caregivers.
The ICU matron (who gave evidence as well as the doctors) explained that, because of her brain injuries “despite being with us for almost a year, none of the team are familiar to her. She is meeting strangers every day”. They now try to avoid hoisting her into a chair (to help with skin integrity) because “the whole process of hoisting, even when someone understands, is frightening and AH was looking very frightened when we did that”.
This comment hit home as I’ve worked in care homes and was hoisted as part of my training. Even for me it was not a nice experience. It made me think that it must be so much worse if you don’t understand what is going on and don’t have any control over your own body. I‘ve certainly seen how hoisting can be a really upsetting and scary process for some residents, even in a routine care setting.
On top of this, AH is subjected to physically intrusive medical treatment such as the mechanical ventilation itself and associated interventions. This was highlighted by evidence from the independent expert, Dr Danbury (the 4th clinician to give evidence in the court, but one who was not part of the care team). He said that deep suctioning, which this patient requires regularly, could be particularly painful. It has been described by some survivors as “akin to having a red-hot poker pushed down your throat”. This witness also described how patients who have been severely ill and in ICU for a long time report terrible disorientation and “psychological scarring”.
Summing up in her closing statement, Katie Gollop QC (representing the Trust) highlighted the relentless and repeated interventions carried out on AH. She referred to witness evidence to highlight that the treatments necessary to sustain this patient’s life were ‘tortuous’ and a ‘torment’ for AH.
The family do not necessarily accept the clinicians’ descriptions of the ‘fear’ ‘pain’ & ‘psychic anguish’ this woman might be suffering. In any case, the decision must be a balanced one that also draws on what she would have chosen based on her own beliefs and values, and the acknowledgment of the comfort and pleasure she appears to derive from family visits.
For me, however, this case left me with a clearer sense of just how excruciating some treatments might be and that time in ICU is not a neutral ‘suspension’. It highlighted the importance of grappling with this information and thinking for oneself what one might want and trying to inform the right decision for others.
Rhiannon Snaith is currently studying for her MSc in Research Methods at Cardiff University, in preparation for starting her ESRC PhD scholarship on “The Role of Journalists in Reporting End-of-Life Decisions”, supervised by Professor Jenny Kitzinger. She’s just started tweeting @Rhiannon_Snaith and is looking forward to joining in online discussion of law, ethics, and end-of-life.
[i] I was only able to attend the second day of the hearing so did not hear this witness myself, but benefited from access to Jenny Kitzinger’s (anonymised) notes from her observations of the first day. As recording is not allowed in court, these quotes are as close to what was actually said as possible, but are unlikely to be verbatim
3. The problem with ‘splitting’, by Claire Martin
“Splitting is a very common ego defense mechanism. It can be defined as the division or polarization of beliefs, actions, objects, or persons into good and bad by focusing selectively on their positive or negative attributes.”
Psychology Today May 2020
I am a clinical psychologist, working in the NHS. I get on with some patients better than others. Sometimes there seems to be a better ‘match’ or what I offer or the way I relate seems to suit some people better than others. There can be a tendency, for us all in the caring professions, to feel that the people we get on with less well are ‘hard to engage’ (instead of ‘I find it hard to work with this person’), or ‘difficult’ (instead of ‘they are asking questions I find it difficult to respond to’) or who exhibit ‘challenging behaviour’ (instead of ‘their behaviour challenges my skills’). We can put the blame for people not liking what we do on them, instead of looking to see how we could do things differently or handing over to someone else. Psychological processes and patterns of relating are happening all of the time, between us all, and do not reside only in our patients and clients. We all bring our own experiences and ways of being to our professional lives. Difficulties can arise around communication and how we relate, rather than ‘mistakes’ as such. Problems with communication are the most frequent formal complaint to NHS Trusts.
AH’s family spoke from their experience and their hearts when describing her. They all clearly love AH dearly, desperately want her condition to improve and for the court to rule that she should continue to be ventilated and allowed to survive for as long as possible. They think AH also wants this.
Their evidence that they witness purposeful communication that demonstrates an understanding of her situation (that she requires ventilation to survive) is at odds with the evidence from AH’s treating clinicians and the expert witnesses who have assisted the court.
Balancing all of the evidence and deciding whether it is in AH’s best interests to continue with life-sustaining treatment must be a hugely challenging decision for the judge to make.
At the end of the hearing, I was left with a feeling of unease about the way in which the family was psychologised when they spoke of differences in the quality of care they experienced from different members of the treating team.
Part of the family’s evidence had been about their experiences of different doctors and nurses involved in AH’s care. Their evidence was mixed – one doctor in particular was described as ‘caring’ and ‘patient’ with AH. Another doctor was experienced as ‘just wanting to pop the tube out’ and ‘not patient’ with AH when assessing her.
The eldest son said: “Dr A’s judgment cannot be trusted” – contrasting him with Dr B who “makes a lot more conscious effort to engage with mum and to listen to us”. Looking across the courtroom at Dr B he said, “I know you care about my mum, Dr B, I know you do.”
They also said of some nurses: ‘they’re busy, they talk at [AH], others talk to her. There’s a difference. Sometimes, I have seen, some nurses ask her a question and before she’s had time to answer – I can see she’s going to answer – they’re gone’ (AH’s sister).
Whether the professionals involved think that they do or don’t fit this characterisation is not the point. This is how the family experiences their interactions with them and observes their interactions with AH. They did not characterise all professionals in the same way, and were keen to point out excellent care and some staff who have a ‘gentle manner’.
In closing submission, Katie Gollop QC said[i]:
“The COVID pandemic has been brutal and caused situations of emotional brutality up and down the country. At a different time, there would have been scope for more family visiting, perhaps scope for more fruitful discussions and the ability to come to terms with the nature of the illness. All of those things have been denied to this family. It had seemed in August that some family members had come to terms with the reality of the situation. Since then, psychologically, in terms of absorption of that information, that capacity has been lost. How can somebody so full of life, such a powerful person, right at the heart of this family, suddenly be taken away from them and reduced to someone totally dependent on others when before she had others dependent on her? This is unbearable and unacceptable to them. Family members have developed coping strategies to enable them to bear the unbearable. They think she’s getting better, when all the evidence is that she is not. They believe she’s accepted her situation, when the evidence is that she doesn’t have the mental capacity to understand her situation. They say she tells them what she wants, when all of the evidence is that she does not know what she wants because she does not have the capacity. They say she’s a fighter and wants to fight on, when the reality is that air is painfully pumped down into her lungs through a tube down her windpipe. They say she can improve, when there’s been no improvement. They say she needs more time, when there has already been four months more time and Dr Danbury was very clear about her condition and prognosis. Sadly, very sadly, [one of AH’s daughters] who was very capable of understanding the situation in August makes some of the most unpleasant accusations against the hospital – as unpleasant as they are baseless. There is the splitting mechanism in action: Dr B the good doctor, Dr A the bad doctor. All this is understandable, but Your Ladyship is concerned with AH and not with the family.”
I don’t know if the family is mistaken about seeing improvement and an ability to understand and communicate in AH. That picture is certainly at odds with the clinical assessments presented by the team caring for AH and by the expert witnesses.
But even if we assume that the family is desperate to see what they want to see in terms of progress for AH, and has misinterpreted ‘signs’ from AH and over-valued change as recovery, it does not logically follow that experiencing Dr B as caring and Dr A as uncaring is unfounded – or indeed ‘splitting’.
That would be to assert that, because the family is wrong (according to the NHS Trust) in their assessment of AH’s condition, progress and prognosis, they cannot are trusted to report accurately their experience of how people relate to them and to AH. And, moreover, that the reason they report different experiences with different clinicians is due to psychological difficulties that reside in them.
The term ‘splitting’, in particular, can be used pejoratively as a defense within systems of care and applied to people given a label of ‘personality disorder’. It is not a term to be used lightly, or by those untrained to apply it.
If the court relies on expert medical evidence to make submissions and declarations about physical health conditions, it is not appropriate to bandy about psychological terms and attach them to parties without expert psychologist/psychiatrist evidence – which is then open to testing in court.
Good reflective practice – and the NHS Constitution – require that we all, in the NHS, respond to concerns, feedback and patient experiences with humility and a willingness to learn about our ways of working and relating.
Commitment to quality of care
We earn the trust placed in us by insisting on quality and striving to get the basics of quality of care – safety, effectiveness and patient experience – right every time. We encourage and welcome feedback from patients, families, carers, staff and the public. We use this to improve the care we provide and build on our successes. ( NHS Constitution)
Suggesting that the family is lacking in objectivity because they are in some way psychologically compromised serves the purpose of undermining and discrediting their evidence. This was not necessary to powerfully argue the Trust’s case that ongoing life-sustaining treatment is not in AH’s best interests. The medical evidence stood alone.
This could be described as a ‘power-over’ position – appropriating powerful psychological terms (not likely to be familiar to the family in their actual meaning, and without any expert evidence to support the claim) in a submission that cannot be challenged.
When can we, as a patient or relative, say that care is not good-enough without that concern being psychologised away?
Or raise that the way this person speaks to me/my family member is not experienced by me as caring/compassionate/helpful without that being recast as a problem within me?
A tweet from Kathryn Mannix, author of With the End in Mind and Listen: how to find the words for tender conversations addresses this point and her analysis should be read by everyone in the caring professions. She says she has been the doctor whose words were not understood as she intended them to be by patient and family, and she takes responsibility for that miscommunication. She posted photos of this text (from her book, With the End in Mind (pp. 114-115) )attached to a tweet. The text describes an interaction between herself and Maggie, the partner of Fergus who has just died under her care.
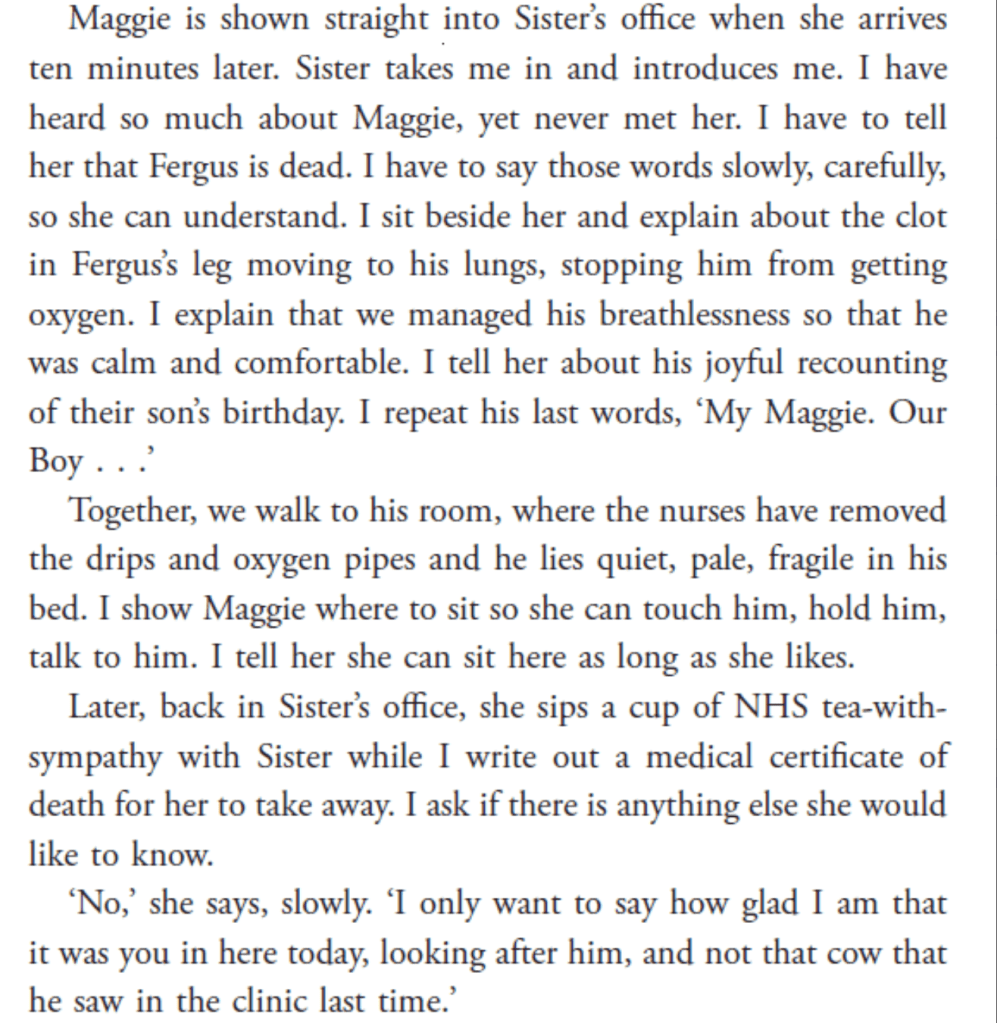
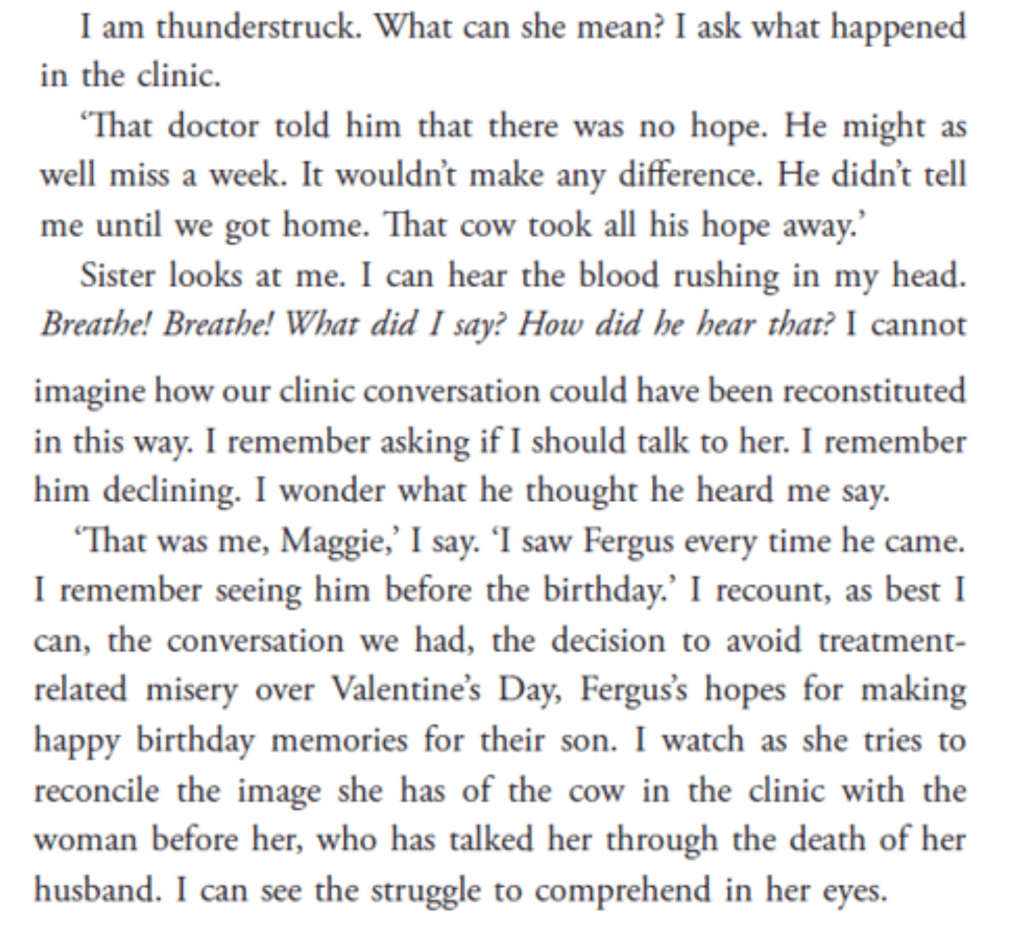
So, “I have been the doctor“, says Kathryn Mannix, “whose words were relayed by a v sick patient to a relative, & what the relative heard was not what I said. But it WAS what the patient/family understood from what I said, so I was responsible for that miscommunication. Communication matters.“
I was pleased that counsel for AH via the Official Solicitor said both that she believed Dr A to be a “compassionate clinician”, and also that she “does not accept the Trust submission that there’s been an attempt at splitting”.
Counsel for AH asked whether – without any aspersions being cast against the two clinicians the family say they have difficulty with – some adjustments could be made:
“Placing AH’s wishes and feelings at the forefront, how difficult would it be to ensure those two clinicians are not involved in her care? It is best to ensure no friction at this time. I wonder if that is beyond the resources of the Trust in the circumstances of this case.”
Sometimes it may be necessary to accept that we are not the person a family needs at a particular time. And we can do that without pathologizing the family in a situation like this.
Claire Martin is a Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a member of the core group of the Open Justice Court of Protection Project and has published many blog posts for the Project about hearings she’s observed (e.g. here and here). She tweets @DocCMartin
[i] We are not allowed to audio-record hearings in court. This quotation is an amalgam of the three versions of what Katie Gollop said that were written down/typed by Claire Martin, Jenny Kitzinger, and Celia Kitzinger. We recognise we each had slightly different versions, but the differences were small and do not seem to us to be significant for the purposes of the argument here (e.g. the difference between “come to terms with the reality of the situation” vs. “understood the reality of the situation”). This is true of all the other quotations in this piece. They are unlikely to be verbatim, but they are as accurate as we can manage under the circumstances.
4. Human connection, communication and capacity: Family experience of trying to determine AH’s wishes, by Jenny Kitzinger
For me, the most moving, and complex, part of this hearing was the family accounts of visiting AH – and how this informed what they thought should now happen.
In the witness box at the Court of Protection at this re-hearing on 7th and 8th December 2021, AH’s adult children and her sister vividly described their experiences at the bedside, explaining how they felt AH had become more alert and engaged since the hearing before Hayden, J back in July 2021.
Their accounts illustrated powerful human connection. The family were also adamant that they’d established meaningful communication with their mother/sister, and that AH conveyed a consistent wish that they should keep fighting for her; she does not want to die.
In this blog I record what the family reported and ask: How can this help with ensuring that AH’s feelings are factored into the best interests decision? And what is the relationship between human connection, communication and capacity?
I focus on this partly out of my academic interests in best interests decision-making and the resonance this family’s experience has with the stories of relatives of other severely brain injured patients interviewed for our research at the Coma and Disorders of Consciousness Research Centre.
But the reason I found myself so intensely engaged with this family’s account was because parts of what they said reminded me of (and sometimes contrasted with) my own experience of being at the bedside of my sister, Polly Kitzinger, while she was in a Minimally Conscious State for two years after a road traffic accident in 2009. It also connects to my ongoing experience of making best interest decisions for her as her court-appointed deputy for Health & Welfare.[1]
The clinicians’ perspective – emphasising the burdens of treatment and lack of capacity
Clinicians giving evidence in court (and the reports read out from other members of the multi-disciplinary team) describe AH as predominantly either sleeping, or neutral (‘just lying there’), or when she is alert, often appearing tearful, fearful, anxious or in (psychic or physical) pain. Such distress was sometimes, but not always, linked to the necessary interventions she undergoes to be sustained alive in intensive care (as also highlighted by Rhiannon Snaith (above)). They emphasised that this independent, family-centred, very private woman would have to remain on a mechanical ventilator in intensive care for the rest of her life. She was likely to die soon, one way or another: the issue was not whether she would die, but how and when.
In so far as AH can communicate or understand anything at all, the clinical assessments suggest this is very minimal. A recent report from the specialist Speech and Language Therapist concluded that: “meaningful and purposeful communication remains extremely limited. If anything over last two months communication has deteriorated with increased signs of what appears to be distress”. She was never able to initiate communication or spontaneously express her needs. There was some simple command-following and someYes/No responses, but these were not completely reliable or consistent, and were not adequate to support functional communication or inform a significant decision.
The family perspective – emphasising human connection and communication
The contrast between the clinical accounts of AH and those offered by her family perspective was profound. Family members did not focus on deficits in understanding or communication: instead they focused on their mother’s fight to live, family love, mutual recognition, comfort, concern and human connection. They also talked about their mother making choices and communicating her wishes, including in response to family efforts to ask her about what she wanted in her current situation.
One son, ‘K’, described how when he went in to see his mother she “lit up” and was “transfixed on me”. His reports that his aunty said “she’s looking at you, she recognises you…she’s really happy to see you”. He placed his head against her and “she was pushing her head against me. I had a comforting feeling…. She was giggling and smiling at me.”
A daughter, ‘S’, described how, after coming back to the UK to see her mother after some time away: “You could see her emotion in her eyes… She cried when she first saw me, obviously, and she got to see her grandson. Her eyes fixed on him, she knew who he was”. During this visit she “felt like I was having meaningful discussion with her”. Later, when visiting her mother along with her sister, she told her mother about a deeply personal and sad recent experience in her own life: the three cried together, with her sister lifting her mother’s arm to place it around her.
It wasn’t all intensely serious: there was humour too. The oldest son, ‘A’, described a family visit involving “a cousin who was supposed to marry her when she was young”, who was joking by saying “come on, let’s go get married now you’re single”. “Oh my god, the smile on my mum’s face”, he said. “I was cracking up, I was laughing, she was laughing – you just know she’s dying of laughter inside”. Another time, “one of the patients farted really loudly: it was gassy, it was really loud, it was BAD. And I said, ‘that wasn’t you, was it Mum?” and she was smiling”.
The family seem to be able to help AH feel relaxed and safe too. Family members described how they could soothe her to help her accept interventions. One particularly distressing scene was described in which AH’s youngest daughter, Daughter A, arrived while nurses were attempting to place a tube into her mother’s rectum. After gently talking to her mother to explain why it was necessary, her mother appeared willing to comply and “there were no more tears’.
The family were clearly skilled in trying to maximise AH’s opportunities to communicate by ensuring she was clean and comfortable, and was given enough time to respond (all elements recommended in professional guidelines).
They are, of course, not coming in with painful instrumental goals (suctioning, hoisting, turning) – which might make her tense and overwhelmed. They were clearly engaging with her in empathetic, meaningful, sociable and familiar ways (including familiar religious or cultural rituals). They might also bend the rules: one son said he sometimes lowers his mask as “she communicates better if she can see my face”.
They had refined practices to try to ensure answers to questions were accurate (e.g. asking the same question in different ways) and they had developed routines to check for sources of discomfort, e.g. reporting occasions when asking about different parts of her body in turn had allowed them to detect, for example a hand twisted under the blankets, or the fact that she had soreness behind her ears.
They also tried to ensure her choices to allow for pleasant experiences: anticipating what she might like based on their long familiarity and love for her, inviting her to nod or shake her head or to use tongue movements as they offered her choices about having her nails done, her hair dyed, or deciding, for example, what television programme to watch.
AH is clearly at the beating heart of this loving and devoted family and family time was created around her too (within some constraints due to Covid). Family members usually visit in pairs and there is an emphasis on including AH in conversations. AH’s sister described an interaction between herself, her niece and a nurse and how AH was part of that, commenting: ‘She actually belonged, and was not forgotten about’. The clinician’s view of AH made no sense to her: “I feel she’s communicating back to us. I find it really difficult to say she’s deteriorating. She’s just there. She’s there. I do feel that she’s there.”
This contrast between family experience and clinical accounts is even more vividly described by the son who declared that in reading about his mum in the notes and public reports, “it’s like she’s just a corpse with a damaged brain and a machine attached to her – but this woman watches TV!”
I recognise much of what this family describe from my own experience of being at the bedside of my minimally conscious sister – and it is familiar from interviews with other families in this situation too (see examples on the healthtalk resource).
As family members, many of us will recognise how someone with profound brain injuries may nevertheless sometimes ‘light up’ when we enter the room and gaze unwaveringly at us, as if with great love or as if trying to communicate by telepathy.
We also know how our sister, partner, child or parent can seem to absolutely trust us, and we can (sometimes) soothe them or help them stop struggling against a care intervention that we feel it would be best they receive.
They may also appear to focus all their energies in an effort to communicate with us (or even to engage wih a phone call from another relative) and may share (or mirror) our own emotional responses, or burst into laughter as we joke around trying to lighten the mood.
Minimally conscious patients can, at times, give meaningful responses to careful questioning, even if we can sometimes be unsure about accuracy, or responses are inconsistent (or very consistent with some questions but not others, perhaps)[2]. We have probably also all witnessed some staff who are patient and skilled in maximising all possible communication (and helped to add to family knowledge about good approaches), and others who seem impatient or disrespectful (talking over, not to, their patient).
The clinicians too accepted (in part) many aspects of what the family reported. Having seen videos of AH with her family or observed such interactions themselves, clinicians mostly accepted that the family were getting some connection with AH that was different from staff engagement with her.
Dr A said: “I accept the richness of their relationship and communication with her is different from that of all the treating team …I fully agree that the family have a richer substrate of communication with her…There is a shadow of AH left and it is focused on the people that she knew…Her family are ingrained on her”.
Ms C, the matron, said “The videos echo what I’ve seen at the bedspace when family visit. I’ve seen those interactions face to face as well”…
Dr B, the consultant neurologist said “there is no question, when the family arrive the level of distress goes down. ”
The independent expert, Dr Danbury commented that it is common that people with severe brain injuries are more likely to respond to familiar faces and that “long term memory is generally preserved at the expense of short term memory [.. ] so it doesn’t surprise me family get the best out of her”.
The fact that family often “get the best” from a patient is well established in the clinical literature. That is why family are encouraged to be part of assessment processes and to report, or indeed video, their interactions. (See the RCP Guidelines.) The closing statement from counsel for AH via the Official Solicitor underlined the “clear and cogent evidence from the family, who know their mother very well”, emphasising the the fact that family may pick up on signs missed by professionals and that the family are attentive and observant. Family evidence must be factored into decision-making.
However, quite how family members interpret what they experience, and exactly what weight should be placed on what they learn from their mother, creates more conundrums.
Questioning the implication of ‘responses’ – the communication conundrum
Where clinicians differed from the family was in their views about the accuracy and consistency of AH’s “communication” i.e. whether expressions or gestures which appeared to indicate ‘yes’ or ‘no’ were always intentional, and, if they were, whether they really always reflect an understanding of the questions or issues being discussed.
Dr B explained how in seeking to ‘test’ a patient’s understanding it was, without the right training, very easy to inadvertently cue something (e.g. in the way one read out the optional answers, placing emphasis on the correct answer). He also pointed out that “with a yes/no response you are already at 50% just by chance”.
Although seeming more ambivalent about how to interpret AH’s emotional responses, members of AH’s care team also cautioned against always interpreting something as a ‘response’ when it could sometimes be observed happening ‘randomly’ when family were absent and no one was interacting with AH at all (e.g. ‘random tearfulness’). It was understandable that family members would read everything as ‘meaningful’ and construct a narrative around it, but this was not necessarily always the correct interpretation.
Some apparent responses to conversations were also explained away by the clinicians as potentially being ‘emotional’ mirroring rather than cognitive processing. A particularly excruciating discussion revolved about scrutinising one daughter’s report of explaining to her mother how she’d recently suffered a painful personal loss, and how her mother and she (and her other sister too) wept together, with her mother’s arm around her for comfort. Dr Danbury was asked to comment on AH’s tears in this situation. It was, he said, a “tricky” experience to interpret:
“But you could say – [Daughter S] and her sister were upset – the body language was one of sorrow and upset. It may have been that her mother was responding to the body language of her daughters rather than a true understanding of the words themselves. That is an alternative explanation. It is difficult to say that she [AH] understood [what was being said to her] as a multi-level statement.”
For the clinicians, there was nothing in the family’s experiences that undermined their view that AH could not understand her current situation, and also that she certainly did not have capacity to make a decision about it (including the sort of ‘supported decision-making’ that might work for some people).
They made clear that an ability to respond emotionally should not be conflated with a cognitive capacity to understand, retain and weigh up information about a medical decision.
On the face of it family members were not arguing that AH had the capacity to make the decision about continuing mechanical ventilation. They were simply informing the court of her current wishes and feelings as they understood them on the basis of their prior and current knowledge of her.
Counsel for the family was clear in his opening position statement that they were not disputing the clinical view that she “lacks capacity” in relation to the decision to be made by the court. However, at times this seemed quite ambiguous in individual family members’ testimonies or in their response to questioning.
In part this was implied in the way family members challenged the formal clinical assessment of what AH could or could not understand and communicate, and when they made clear statements about what AH now thought and had somehow been able to make understood by her family e.g. “She’s grasped what’s happened to her: she’s accepted it” (Daughter S).
Most importantly family members repeatedly informed the court that they had asked their mother what she wanted in her situation and she had indicated that she did not want to die.
Clinicians stated that they did not feel it was appropriate for them to seek AH’s views on treatment decisions, as she lacked the cognitive capacity to respond in a way that could usefully inform (let alone determine) the decision.
The family took a different view and had frequently asked their mother what she wanted to happen next, and were frustrated and upset by the apparent lack of respect for what they consistently heard from their mother. The way in which her children presented the question and understood the answer from their mother was unpacked in questioning,
AH’s oldest son “A”, for example, commented as follows:
Son A: My only interest is to give my mum what she wants. So I thought I would crack the question – “Do you want to be put at end of life, palliative care?” [ …] “Mum, doctors and nurses want to put you at end-of-life care, is this what you want?” – and you can see her [shakes head]. Every time we ask her the same questions: “Do you want to return to Allah? Do you want to continue?” Every time without fail [shakes head]…[They say] “sorry but your mum doesn’t understand the question”. What do we do? It’s like banging your head against a brick wall” .
Gollop: Do you consider that your mother has the capacity to make a decision about whether ventilation should continue?
A: I personally believe that if you ask her that question, she’ll give you the answer.
This was echoed in the response of other family members, all of whom felt that AH had indicated a clear desire to live and had ‘capacity’ to answer the question about ventilation (although it was unclear whether they felt she had ‘capacity’ in the sense of understanding her true clinical situation).
Gollop: Does your mother have capacity to make decision about whether or not her ventilation should continue?
Daughter S: Yes, if you ask my mum she will give you her answer.
Gollop: Do you think she has capacity?
S: Yes I do, I do think she has the capacity […]
Gollop: You think she understands what is going on around her and she understands what her condition is like, and what it will mean to be ventilated for the rest of her life?
S: Yes, I know my mum’s aware.
G: Your belief is that she chooses to continue to be ventilated?
S: I don’t think anyone chooses to be ventilated, I think my mum wants a chance to get better.
G: Every single doctor says there is no chance of improvement – do you reject that evidence.
S: No, but I know my mum doesn’t want to go onto palliative care.
Questioning in court tried to tease out whether the children themselves were able to address the risks that the experts believed faced their mother – not a choice between dying and living, but a choice about how she would die. Her children were very honest in their responses: this was not a question they felt they could answer. In questioning “S’ for example, the following exchange occurred:
Judge: The medical evidence is that your mother is not going to be able to come off the ventilator. What do you think her views would be if that were the position?
Daughter S: That is a hard question, because our mum has told us to not give up on her, and she’s told us to keep going, so I can’t answer that question for us. All I know is our mum…everything is about doing what our mum would want. Saying “yeah, she would want you to switch off the machine” – that’s not us fighting for her.
Similar issues were explored with AH’s son, “A’:
Gollop: Have you read Dr Danbury’s report? There is a high risk of sudden unexpected death without her family there. A very high risk of dying alone. Passing away alone without people around her praying for her…
Son A: you can’t guarantee that…you just don’t know
Gollop: …The choices are continuation or withdrawal of mechanical intervention (in the hospital). One allows her to die with the people she loves around her, praying for her and the other puts her at a very high risk of dying alone.
After A indicated that he couldn’t really engage with that question, the judge intervened.
Judge: I’m going to have to face the reality. On one view of the evidence there’s a strong likelihood that will happen, so I think what you have to think about – if you want to – is what Ms Gollop is saying: that part of the component decision is to think what is in your mother’s best interests.
Son A: I wish I asked her this.
And being gently pushed a little further by the judge to try to provide an answer himself, he added
“It’s like saying would you rather be hit by a bus or would you rather drown – you don’t want either of them”.
He subsequently became tearful saying:
“I would give up everything I have to look after my mum… What is the point in being a son if you’re not going to be one.” (Son A)
It was at this point that Katie Gollop QC underlined that the Court of Protection was there to ask and answer the question that the family were finding so difficult to address. The court, she said:
“..can take the burden of responsibility away from those who feel it so weightily and pass it to a judge. The hospital would never wish anybody who has the grace to participate in this process to feel that they are responsible in any way for the outcome.”
The judge underlined this point, the family love for AH was clear, she said, “that shines through”. There is no criticism of anything family has said or not said. The outcome is the responsibility of the court
Judge: “It’s entirely my decision”.
It was hoped that the decision would be ready to hand down on the afternoon of Monday 13th December 2021.
Jenny Kitzinger is Professor of Communications Research at Cardiff School of Journalism, Media and Culture. She also co-directs (with Professor Celia Kitzinger) the Coma and Disorders of Consciousness Research Centre and runs online training for healthcare professionals about law and ethics. She tweets @JennyKitzinger
[1] Polly had a ‘traumatic’ brain injury which has a different prognosis than AH’s type of injury. She was also much less physically compromised than AH and displayed (to me) a much higher level of distress than this family report. Polly left intensive care within weeks to move through high dependency, rehabilitation and into the long-term care system, emerging from MCS after two years. She has profound neurological deficits, still requires 24/7 care and lacks capacity to make decisions about any medical treatments.
[2] In my experience, it is easier to see the extent of a brain damaged individual’s lack of capacity to make particular decisions once they are more recovered and a relatively clear and consistent ‘yes’/’no’ communication is established. It is then that hope, deduction, facilitation or ventriloquism become less a part of the interaction process and gaps in understanding, processing, weighing or recall may become more starkly evident. It may also, however, at that point, seem to be possible to confirm earlier interpretations.

Excellent commentary on a nightmare of a case, particularly the analysis from Prof Jenny Kitzinger. One of the most challenging things about my job (speech therapist) is when there is a chasm between families and clinicians and their interpretation of ambiguous/non-purposeful responses. It is often very difficult to know how much to walk families along the path of realisation and the clinical context matters enormously.
As a rule, I have noticed that the families of people with degenerative disorders (rather than acquired brain injuries) tend to share the perspective of clinicians. They’ve had time to metabolise the shock, watch the change before their own eyes, watch their loved one struggle in many environments and the proof is abundant.
I think acquired brain injuries cause such shock, and distress, and anger that discussing the changes they have caused is a much more fraught conversation. Not least because it is much easier to explain away their inability when physical paralysis co-occurs and they are in hospital. (“They’ve never liked hospitals, they’re not listening to you, they can’t move”.)
I used to push and push (“you ask them to do it then, why wouldn’t they do it when you’re telling them it’s important, how can they understand if they don’t do x”) in the misguided belief that ‘therapy’ was impossible if we were not on the same page. I look back on those conversations with horror. Not least because it was rarely successful.
Sometimes, I’ve come to realise the conversation isn’t even necessary. Or not at that time anyway. However as this case illustrates, the majority of the time circumstance doesn’t allow the luxury of time for loved ones to come these conclusions on their own. Nor should they have to find out on their own lost in pain and fury. They should have a trusted shepherd to guide them. It is a conversation that is needed to avoid outcomes like this one, where clear harm occurs to the individual with the injury, and the grieving process is substituted for a self perpetuating loop of anger.
I felt particularly affected by the quoted. words of one of the patient’s sons: “It’s like saying would you rather be hit by a bus or would you rather drown – you don’t want either of them”.
Isn’t that exactly right? What is being said here is “emotionally, I find this situation intolerable.” No amount of rational explanation from wise clinicians will change that. My observation is that anger gives us fuel, and often begets more anger and traps people in it. Grief and acceptance is often punctate and devastating. Yet those that can access grief and feel it fully tend to be able to rebuild their life over time.
I’ve come to believe that, for a person whose job is all about speech and language, that actually the words we choose when having these conversations are the least important part of it. Not least because what families say is often not what they mean. “She’s not listening – she hates it here” can really mean “I cannot entertain the possibility that our relationship as it was, has changed forever”.
“You need to do everything to keep her alive: it’s what she wants” can sometimes mean “I feel so guilty for focusing on myself and my career/kids/moving away and the idea I haven’t got time to redeem myself is unbearable”.
“The nurses don’t know how to care for her” can mean “I wish I could be here all the time and I find it so hard to be away when she’s so sick”.
The timing and nature of these learning conversations with loved ones, particularly in the less-than-ideal hospital environment, is so essential to helping families walk the path of realisation. Trust in the clinician helping them uncover these painful and devastating truths is essential and no simple task. As mentioned in the blog post, Kathryn Mannix’s conversation frameworks have been a lifeline for me and have made it much easier, and greatly increased the chance of a better outcome.
The longer I’ve worked the more I find myself counselling the loved one, speaking to their emotions, and letting them know I see their pain. Only when I’m convinced they believe this do I gently start to explain what we typically see in this type of injury and if they’ve noticed any of those things. More often than not, inch by inch, day by day, they come to see things as they are. Occasionally, there is even time for a bit of speech therapy…
With the impossible time pressure on clinicians, this is sometimes just impossible. I’ll be the first to admit don’t always get it right. Nonetheless, I keep learning, always in the hope that fewer families suffer in the way this family has and that they are allowed to experience normal healthy grief and then re-learn to live.
Thank you so much for these reports from the Court of Protection. They are of enormous benefit to a wide range of readers. They certainly make me reflect on the privilege and pain of accompanying those who experience these heartbreaking traumas.
LikeLiked by 2 people