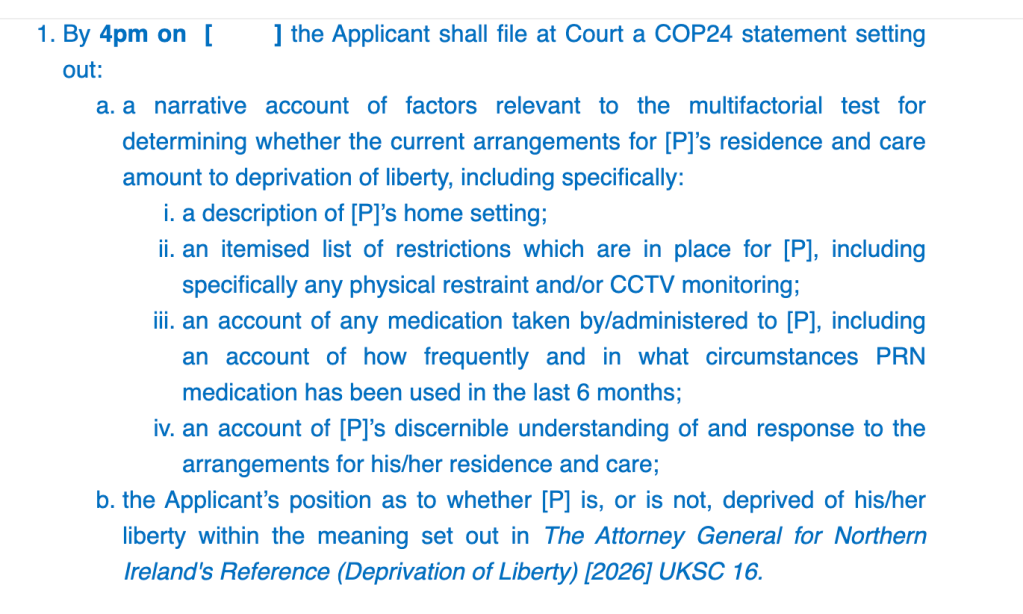
District Judge Glassbrook is a very engaging judge to watch because of the extent to which he “shows his working” as he listens to competing submissions, tests arguments against the law, and makes his reasoning transparent.
I don’t know what the judge will eventually decide in this s.21A case – it will be back in court later this year – but in terms of everyone’s concerns about how AGNI will be interpreted in the Court of Protection, it’s an interesting case. Although P’s ‘deprivation of liberty’ is currently covered by a Standard Authorisation, the local authority has suggested that P may no longer (under the AGNI criteria) be deprived of his liberty. The judge disagreed, saying: “The Supreme Court said that if there are objections then, on the face of it, we’ve got deprivation of liberty”.
Despite the obvious importance of establishing the legal basis of P’s confinement (is it or isn’t it a ‘deprivation of liberty’?), this judge – like others I’ve watched since AGNI – gave priority to considering whether P’s residence and care arrangements were in his best interests and the least restrictive necessary. That was the only reason it was in court today – called in by the judge after the parties had made an application to vacate it.
Background
Proceedings in this case (COP 2002681) began about six months ago, in January 2026. The protected party is a man in his seventies with dementia and several other medical problems, including insulin-dependent Type 2 diabetes. Until a few years ago, he was living alone at home. He was admitted to hospital twice, first due to being “disoriented” and wandering the streets, and then because he was found collapsed on the stairs outside his neighbours’ flat. After the second admission it was decided that a return to his own flat was “not viable”.
He’s been in the current placement for almost exactly two years – following a move from a different care home, where he lived for nine months after hospital discharge. His current care home is closer to his son, and I think that was the reason for the move.
It’s clear that P is objecting to the current arrangements. He’s said that he feels restricted in his movements, would like to go out more often, and that not being able to go out “wears me down”. He’s not allowed to leave the placement without support and the placement has said that staff shortages prevent them from being able to take him out. He’s also been verbally and physically aggressive towards staff and other residents and has been prescribed Risperidone which has “helped to reduce challenging behaviours”.
The current care home served notice on him almost a year ago – apparently, he is “intimidating” other residents. At the moment there’s no alternative accommodation available. Several care homes have been approached without success; and “further assessment is required to determine whether community living would be appropriate”. His flat – the place he called “home” – is no longer available to him.
There’s been some uncertainty about his capacity to make decisions regarding residence and care. It’s reported that when he was visited in February by his Accredited Legal Representative (ALR), he “presented very well and answered questions realistically” and “did not evidence confusion or disorientation during the meeting”. In May, a social worker reported that there has been “an improvement in [P’s] presentation, insight into his condition and need for support”. It had seemed possible – and his legal representatives had argued – that P might be found to have capacity to make his own decisions about residence and care.
But the situation changed a few days before the hearing I watched on 1st July 2026, when the parties received an expert capacity report finding that P lacks capacity to make decisions about his residence and care.
The parties had made an (agreed) application to vacate this hearing because they wanted time to consider the report before deciding on their positions. The judge refused the application to vacate because he was concerned about the restrictions P was facing, and about the non-compliance with the ‘condition’ he’d imposed on the Standard Authorisation.
The hearing
The judge focussed on what is going on for P right now and wanted to address it immediately, rather than wait for another couple of months. In particular, he was concerned that, irrespective of P’s ‘capacity’ to decide for himself on residence and care, P should not be subject to restrictions on his access to the community that are not in his best interests.
The ‘condition’ imposed on the Standard Authorisation
A couple of months earlier (on 2nd April 2026), pending final determination as to whether or not the “capacity” condition of the Standard Authorisation is met, the judge imposed a “condition” on the authorisation currently in place – a condition designed to address P’s objections to where he currently lives. At the beginning of the July hearing, DJ Glassbrook drew attention to the fact that this condition has not been complied with.
The condition required the nursing home to take P out “at suitableintervals and to maintain a log of each excursion and activity offered, and P’s response to it”. But “the log of community access is not being provided”, says the ALR – and that’s what caused the judge concern.
The judge turned to the bundle: “On page 84, paragraph 2, it says that when asked about support to access the community, P advised that he’s not currently receiving any assistance with community access – and he expressed a desire to engage in the community and make new connections. The notes also say that the nursing home has offeredP community access “two or three times a week” and that he declines the offer.So, I’m left with a question: does he actually go out? (It later becomes apparent he doesn’t, and hasn’t been out of the placement “since Christmas”.) Is there actually a separate log of each offer and response as the ‘condition’ requires? And on a broader front, just what is it that he’s offered? If the offer is always to go to a particular café that he doesn’t like, there no surprise that he doesn’t go. In April, I was told that he hasn’t been out since December. Let’s turn to the psychiatric report. There’s a recommendation: ‘non-pharmacological support for well-being, including safe access to the community, the absence of which seems to be adversely affecting his mood’. That’s dated 12th June, so three weeks ago or thereabouts. Has he been out? The assertion, ‘he’s offered activities two or three times a week’ doesn’t really do it for me. It says here: ‘he voices a clear wish to relocate, saying he currently spends much of his time inactive and feels restricted’“.
Here’s some of the courtroom interaction (as best I could capture it).
Judge and ALR
Judge: You’ve very helpfully raised the point that there’s no log being kept of offers of activities in the community – contrary to the condition of the Standard Authorisation. Let me ask you a legal question. If there’s a condition on a deprivation of liberty and that condition is not satisfied, what’s the legal effect of that?
ALR: The Court would have to consider the position of the Standard Authorisation.
Judge: There could be an argument that if the condition is not met, then the deprivation of liberty becomes unlawful.
ALR: Yes, I agree.
Judge: And that means the local authority is at risk here.
ALR: I couldn’t disagree with that.
Judge: The point of that condition wasn’t to find out if the local authority and the managing authority fancied going along with it. There was no dissent at the time from the local authority. There was no appeal against it being imposed. It seems to me that it’s absolutely essential that it’s complied with, and if not the ALR must consider her position of what is she going to do about it.
ALR: Yes.
Judge: And if the ALR thinks the deprivation of liberty is potentially unlawful, it begs the question in my mind as to why the dickens did the two parties agree to vacate the application.
ALR: We are facing more of a pragmatic problem. The placement has given notice. There are no other placements available to him. While the situation is as you’ve described it, there is a risk of further disrupting the security of the placement. There is nowhere else for P to go.
Judge: Just because the placement itself might be at risk, bearing in mind the notice to quit is 11 months old now, is not a good reason to think “oh well, never mind, let’s keep the bloke locked up”. No. I’m not happy with that.
ALR: I’ve heard what’s been said and will be sure it’s passed back.
Judge and the LA
Judge: This is your particular responsibility. In the case of AJ v A Local Authority[2015] EWCOP5, Baker J found that the ultimate responsibility for protecting the Article 5 rights of those subject to deprivation of liberty lies with the local authority. I’m not convinced at the moment that this local authority has met its obligations.
LA: Sorry, Judge. I can’t argue with that at the moment. The fact that the condition attached to the authorisation hasn’t been met – that’s something I’ll have to go back to the allocated social worker to discuss. It was agreed in April and the Nursing Home was instructed, I believe.
Judge: Do you agree that if the condition isn’t met, then the deprivation of liberty becomes unlawful?
LA: It’s not something I’ve faced before. I don’t know.
Judge: What I’m after mainly is what the dickens are we going to do about it? My wish is for it to be put right without me having to make more of a nuisance of myself, but if it’s necessary to have the Director of Adult Social Services and the Director of the Nursing Home to come to court and explain it, we can do that. It may be that if you mention it, that might drive the message home.
Counsel for the LA reported it is willing to fund additional community access “where appropriate” – but no details or time scale were forthcoming.
The hearing continued with expressions of concern (from the judge) about the non-availability of an alternative placement (from the local authority) and expressions of concern about P not leaving the care home, problems with his hearing aids, and a lack of credit on his phone.
AGNI
On the matter of ‘deprivation of liberty’, the judge remarked that “subject to evidence, subject to submissions, I certainly get the impression this chap wants to leave where he is. The Supreme Court said that if there are objections then, on the face of it, we’ve got deprivation of liberty. So, my provisional view, subject to arguments, is that we still have a deprivation of liberty. [Counsel for the ALR], you’re nodding. [ALR: Yes. LA: (pause) Provisionally, yes.]
But in their Position Statement, the local authority addresses AGNI head on and (provisionally) seems to suggest that P may no longer be deprived of his liberty.
“The Supreme Court has confirmed that there is no single universal acid test for deprivation of liberty. The Court must examine the practical reality of the arrangements rather than theoretical possibilities. Accordingly, the Court should consider what actually occurs on a day-to-day basis including whether [P] seeks to leave, how staff respond in practice, whether restraint is routinely exercised and whether the arrangements reflect ordinary care for a person with his needs. The Local Authority submits that the evidence now justifies careful reconsideration of whether [P] remains deprived of his liberty. Whilst staff would intervene if immediate safety concerns arose, the current evidence indicates a settled resident, reduced restrictions, increased opportunities for community access and an absence of routine coercive measures. Whether those arrangements amount to a deprivation of liberty requires fresh analysis applying AGNI rather than historic assumptions. Regardless of the legal characterisation of the arrangements, the Local Authority continues actively to seek a suitable long-term placement.”
It seems from this, and other hearings I’ve observed since AGNI, that P’s ‘objections’ may play a key role in determining whether or not the arrangements for P’s care constitute ‘deprivation of liberty’. Of the three post-AGNI hearings I’ve blogged about, the first reports on a case where the judge determined that there is a ‘deprivation of liberty’ for a person undergoing serious medical treatment under general anaesthetic in hospital, in large part because he objected – to the extent that treatment was possible only with restraint (‘Judge authorises medical treatment and DOLS in hospital”); and the second found no deprivation of liberty for a young woman living under constant supervision and control (including CCTV cameras) in an annex to the family home, and it was significant to his decision that she did not object – and the nature of her disabilities may mean that she has no liberty to lose anyway (Considering ‘deprivation of liberty’ in a family home setting after AGNI). It will be interesting to see how the apparent reliance on ‘objections’ as a key determinant of ‘deprivation of liberty’ continues to develop in this and other cases.
I’ll look out for the next hearing and hope to observe it.
Celia Kitzinger is co-director of the Open Justice Court of Protection Project. She is on LinkedIn (here), and also on X (@KitzingerCelia) and Bluesky (@kitzingercelia.bsky.social)
In April 2025, a woman with diagnoses of mild learning disability, emotionally unstable personality disorder, functional neurological disorder, dissociative disorder and elective mutism, was admitted to hospital. In September 2025, she had surgery and was soon afterwards declared medically fit to leave. But the discharge did not happen. Instead, the case became mired in the unresolved practicalities of getting her home resulting in a series of increasingly urgent Court of Protection hearings.
Her siblings had been trying throughout to make the people around her understand who she is and what she needs. During a hearing on the 5th June 2026, her sister told the court that their lives had been “completely changed” by what had happened (see the previous blog post “Fit for Discharge for the last 8 months”).
By the time I observed the next hearing about three weeks later, on Monday 29th June 2026, everyone appeared to agree on the path needed to get her home. But after months of delay, another risk, this time detention under the Mental Health Act 1983, was in danger of overtaking the plan entirely.
This hearing, like the one before it, was before Mrs Justice Lieven. It had been due to start at 2pm, but an administrative error meant it had appeared in the public listing as starting at 10.30am. In the event, it began at 2.30pm, with Lieven J commenting that she had received the draft order “literally as [the case] was called on”.
There were 27 people on the link, including observers and representatives for the parties: Aswini Weereatne KC for Suffolk County Council; Anna Bicarregui for P’s siblings; Tor Butler-Cole KC for the protected party, via her litigation friend the Official Solicitor; Rhys Hadden for the ICB and Essex Partnership; Steph Collier for the Hertfordshire Partnership NHS Foundation Trust; and a representative for the hospital where P is currently an inpatient.
Proceedings began with something approaching good news. Mr Hadden, summarising where things currently stood, identified the headline points. A new care provider had been identified and would begin shadowing P in preparation for discharge. Progress had been made towards agreement on CCTV and body-worn cameras and, most significantly, there was now a proposed discharge date during the week commencing 27th July.
It became apparent at this early stage of the hearing that Lieven J had no intention of allowing valuable court time to disappear into lengthy explanations. When Mr Hadden began to explain the background to the proposed CCTV arrangements, she stopped him. “You don’t need to give me any of the reasons…I’ve read the papers.”
Mr Hadden then introduced a new complication. Since the last hearing, a Mental Health Act assessment had been requested by the hospital, creating a very real risk that P could face further prolonged detention in hospital. The parties, he said, wanted the court to authorise, on an interim basis, P’s deprivation of liberty in hospital in the hope that if present restrictions were approved the Mental Health Act assessment would become “redundant”.
Lieven J fixed immediately on the proposed discharge week. She would “very, very much prefer” P to leave hospital in the week commencing 27th July, as she would still be available to hold a short hearing afterwards “just to see how things are going” as she had “a distinct feeling that the moment I’m off the job things might not happen”. Next, she moved into the “granular detail”, to check that the parties were not merely saying they agreed “for the sake of the hearing” before “reneging later”.
The first question was whether there was a clear plan leading up to the week of 27th July. Mr Hadden said the new care provider would need a nurse to begin observations and that P would need a social story to help her become accustomed to the idea of a new care agency. Lieven J asked if thought had been put into how P would be informed, and apologised for “micromanagement” but said it felt necessary.
She noted that P wanted to leave hospital but was scared of change and could become dysregulated very easily. The proposed solution was a meeting with P’s siblings and those representing her, to work out how she should be told. The new care provider would need to begin observations, train staff in Makaton and prepare psychological strategies to support P through the move. Anna Bicarregui, for P’s siblings, said they were keen for Makaton training to take place and did not understand why it hadn’t yet started. Lieven J requested “less chat and more action” and instructed the parties to draw up a dated plan that afternoon.
This was my first time observing Lieven J, and if it’s permissible for observers to pick a favourite judge she might just be mine. Direct, practical and plainly impatient with delay, she consistently kept proceedings focused on P. This instinct was evident a few minutes later, during what might otherwise have become a drawn-out discussion about the logistics of installing CCTV in P’s hospital room. Mr Hadden began to explain that the timing depended on the hospital estate team being able to install the equipment. “Well, it will happen this week,” Lieven J replied. “To be frank with you, I could do it on Amazon this week. It’s not rocket science.”
Mr Hadden then briefly attempted to explain that fixed CCTV in a hospital room was not quite the same as buying domestic equipment online. “No, no,” Lieven J interrupted. “I understand…they could do it in two days.”
Lieven J then turned to the safeguards that would have to sit around CCTV. She felt it had advantages over body-worn cameras as it was less easy to delete footage, could not be switched on and off at will, and would record the wider context of what happened in P’s room. But those advantages depended on the footage actually being preserved.
Mr Hadden suggested adapting the existing body-worn camera care plan, but Lieven J was clear that this would not do. CCTV needed its own protocol, particularly because P might become dysregulated when she learned about the camera. Tor Butler-Cole KC for P via the Official Solicitor, added that there should be provision for footage to be kept for longer if there was an incident or injury. Lieven J wanted to avoid “critical incidents” being “randomly deleted” and agreedthat there should be an automatic storage period and a process for preserving footage beyond that if anyone said something had happened.
On the deprivation of liberty, Lieven J made it clear that she was “not going to make a ruling on the applicability or otherwise of the Supreme Court judgment to the facts of this case”. On the facts before her, she considered it “necessary and proportionate” for P to be deprived of her liberty in hospital on an interim basis: “I’m not going any further than that.”
Mr Hadden then returned to the Mental Health Act assessment, explaining that it had been triggered following increasingly serious incidents, particularly one on 22nd June which had led to an emergency protocol meeting.[1] The hope, he said, was that if the court authorised the current restrictions and with a clear discharge plan, the public bodies party to the case might agree that the assessment was no longer necessary. Lieven J responded sharply to this, telling the parties that if they proceeded with a Mental Health Act assessment and sought to make an application, she would expect the Official Solicitor to consider judicial review. She told Ms Butler-Cole KC that she was sitting in the Administrative Court that week, and any such application could be directed back to her.
Mr Hadden then moved to “restrictive practices”, a phrase that was quickly picked up by Lieven J, “restrictive practices, do you mean restraint?”. He did, but he was also referring to PRN medication, including lorazepam, which had been given to P on a regular basis and which, he said, had caused anxiety among professionals because of the prolonged use of restrictions without lawful authority. Lieven J was visibly unimpressed. There was no medical report before the court, no explanation of contraindications and she was firm that she would not authorise medication under Article 5 as this “was a matter for clinicians”. When Mr Hadden tried to explain that the medication had already been prescribed, Lieven J stopped him again. “I don’t care, Mr Hadden…it’s not a matter for me. Do not use the High Court as a veil of respectability for clinical judgements.”
Lieven J then returned to the draft order, which she had only received as the hearing was called on. She felt the provision was too general. If the court was going to authorise restrictions on P’s liberty, the order needed to be clear about what those restrictions actually were, and in particular to make clear that any physical restraint must be the minimum necessary. Mr Hadden suggested an appendix setting out the proposed restrictions, drawn from the local authority’s evidence. That was agreed, until he added that it included PRN medication. “Well take that out,” Lieven J said. She was content for the order to record, by way of recital, that P had been receiving medication because clinicians considered it clinically indicated, but she repeated that she was not authorising it and emphasised that it was not appropriate for the High Court to authorise medication without a full medical report and explanation.
It was agreed that the order would authorise deprivation of liberty in hospital only on a carefully limited basis, with the detail needing to be properly set out in a further hearing before discharge. Mr Hadden said the court would need to return to the issue of P’s deprivation of liberty in the community prior to her discharge from hospital; specifically, whether CCTV should be used in her home.
The new care providers had indicated that body-worn cameras would be needed, but had not yet reached a view on CCTV in the community. Mr Hadden also raised that P had asked to meet the judge. Lieven J said she had considered suggesting it herself at the last hearing, but she could not use Makaton and was concerned that this might dysregulate P. There was also the practical problem of arranging a visit before the proposed discharge week and it was later agreed that a remote meeting between Lieven J and P and her siblings would be arranged.
A timetable was then agreed: care planning documents by 20th July, a professionals’ meeting that same week, and a further remote hearing on 28th July at 9.30am, with the expectation that P might then be discharged on 30th or 31st July. Before moving on, Lieven J returned briefly to CCTV, making clear that her opinion was that fixed CCTV was preferable to body-worn cameras. She felt that people could forget about CCTV, allowing ordinary relationships whilst body-worn footage, was “very intrusive” and would almost physically stand in the way of a normal relationship.
Aswini Weereatne KC for Suffolk County Council, then raised the question of physical restraint, inviting the court to authorise the current care provider’s intervention plan. Lieven J said that would be “wholly inappropriate” as she had not gone through it line by line, and was not in a position to decide whether it fell within Article 5 or was “sensible or flawed”. The plan itself could be referred to in a recital, but the order itself would need to contain “standard wording” that physical restraint could be used only as a last resort and only where absolutely necessary and proportionate.
Anna Bicarregui, for P’s siblings, said there had been real progress in discussions before the hearing and they were grateful for her indication that CCTV was preferable to body-worn cameras. If filming was to happen at all, CCTV had been P’s siblings’ choice as it was “infinitely preferable” to P being confronted by carers wearing cameras.
Lieven J pressed the importance of P’s siblings being fully involved in how the move was communicated to her. Lieven J said that though she had never met P and only had “the most superficial” knowledge of her, from the papers she suspected that P became dysregulated when she was frightened or felt out of control. Her siblings knew her best and were “much more likely to understand her triggers than any of the professionals”. Ms Bicarregui agreed, referring to an occasion when one of P’s siblings had calmed her by tracing figures of eight on her hand. Lieven J then addressed everyone on the call saying that the next few weeks would be difficult for P, and therefore difficult for the professionals too, but there was “no point blaming people” and that for the next four weeks, everyone’s focus should be on getting P out of hospital.
Ms Butler-Cole KC, asked for the statutory bodies to confirm by the following day whether they still wanted it to go ahead with the Mental Health Act Assessment. If they did, yet more work would be needed to prepare P, including another social story explaining the assessment itself. Lieven J queried whether the hospital intended to “shift her to another hospital and psychiatric unit”. Ms Butler-Cole said that would be the outcome if an application succeeded, and that P would not do any better in a psychiatric hospital saying that if things unfolded this way she “may never leave”.
When the Trust representative addressed the court on behalf of the hospital, she explained that the request for a Mental Health Act Assessment had followed a meeting of the public bodies involved in P’s care after increasing incidents, described as “violence and aggression”. The hospital had made the request because it was the body holding P, although she understood it to have been a joint clinical decision.
Lieven J was careful not to dismiss the hospital’s concerns. She understood that there had been a very difficult incident and that the hospital had a duty to protect its staff. But said she felt strongly that a psychiatric admission at this stage would be “very counter therapeutic” for P, and feared that if P ended up in a psychiatric hospital now, “it may be a very long time till we can get her out again”. The possibility remained that the request could be withdrawn, or that the AMHP might decide not to take it forward after seeing the court’s order.
The final substantive issue was the eating and drinking plan, and questions around a professional report which proposed P be discharged with an NG tube in place. Lieven J warned the parties “don’t let the best be the enemy of the good”, saying that some of the things the report sought might be achievable, some might not, but none of that should be allowed to block “the big picture”, which was getting P home. She said there were risks with discharge but also in P staying in hospital, where there was a real possibility that she would end up detained under the Mental Health Act. She understood that public bodies were nervous about carrying risk, and that there was an understandable desire to place it “firmly in the lap of the High Court”, but everyone appeared to agree that it was in P’s best interests to go home and she did not want was a return to “a superficial risk averse approach” in the final weeks.
Mr Hadden then updated the court on efforts to identify an individual therapist to work one-to-one with P. The difficulty, he said, was that the person would need to be Makaton-trained, and such support did not currently exist within the service. It was unlikely to be in place before discharge, but the hope was that it could begin once P was home. In the meantime, P’s siblings would be involved, and the new care provider would be given psychological strategies they could use at carer level.
The next hearing was then fixed for 28 July at 9.30am. After thanking everyone for the work done to reach such a high level of agreement, Lieven J closed the hearing.
Reflections
Observing this case, I was very aware of the larger picture that P’s case sits within. The policy ambition, for more than a decade, has been to improve community support and reduce reliance on mental health inpatient care for people with a learning disability and autistic people. NHS England’s figures for May 2026 show how far that ambition remains from being realised. The latest data recorded 2,130 people with a learning disability and autistic people in inpatient services. Of these, 1,030 had been there for more than two years, and 320 for more than ten. At least 1,920 were detained under the Mental Health Act 1983.
P’s case shows how easily a person with learning disabilities can be pulled towards Mental Health Act detention. All parties seemed to accept that community care would be best for P, and that the longer she remained in hospital, the more distressed she was likely to become. That is now what appears to have happened. Her distress has increased, the restrictions around her have increased with it, and the fact of that distress has helped trigger a process that could lead to long-term inpatient detention under the Mental Health Act.
This is why I admired Lieven J’s handling of the hearing. She did not minimise the risks of P going home, the pressure on the professionals caring for her or the hospital’s duty to protect its staff. But she also recognised that delay and escalating restrictions carried their own risks, and might in the end be far more damaging to P than the risks everyone was trying to avoid. By the end of the hearing, it felt as though there was still a great deal to do, but also some momentum towards getting P home. I hope she will be able to do so.
Elissa Novak is an unpaid carer to her son and studies Law part-time with the Open University through its Carers’ Scholarship Programme.
[1]I was not clear where the request for an assessment had come from. I did request the case summary, chronology of relevant events and issues for determination prior to the hearing, in accordance with the Court of Appeal’s guidance in Gardner (Re Gardner (Deceased) [2026] EWCA Civ 640, but these documents were not been provided.
Editorial Note: This is the fifth ‘commentary’ blog post we have published in the wake of the Supreme Court decision, handed down in June 2026, changing more than a decade of law and practice on ‘deprivation of liberty’ (see Endnote for more information).
Since 2014, with the Supreme Court decision in CheshireWest, my profoundly brain-injured sister, Polly Kitzinger, has been “deprived of her liberty” in a series of neuro-rehabilitation centres and care homes.
Since 2nd June 2026, when the AGNI judgment[1] was handed down by the Supreme Court, effectively reversing Cheshire West, she is probably no longer deprived of her liberty, as a matter of law (though this hasn’t yet been confirmed), and it’s likely that she will soon cease to have access to the associated Deprivation of Liberty Safeguards [DoLS].
Nothing actually changed in the nature of Polly’s care or confinement on 2nd June 2026, except for the way the law now defines it.
The AGNI judgment says that a person is not deprived of her liberty if she is confined “because her condition was such as to require this by way of care” or the person is “wholly incapable of leavingboth because of physical inability and because she was unable to form any desire or intention to leave” (§196 AGNI, approving an earlier judgment, SM before Lieven J). I think this is probably how Polly’s current care provision and condition will be interpreted.
The AGNI judgment has polarised opinion. On one hand, former Court of Protection judge Anselm Eldergill sees it as an “excellent decision” restoring liberty to disabled fellow citizens.[2] On the other hand, some charities say that it strips people of “fundamental human rights protections” in “the biggest rollback of disability rights in a generation“.[3]
This blog contributes a concrete and specific illustration of how the legal concept of ‘deprivation of liberty’ has been applied to one individual person, my sister Polly; and it explores the implications of the AGNI judgment for Polly and her family.
Part 1 introduces Polly as a unique individual with her own particular set of values, beliefs, wishes and feelings about liberty.
Part 2 outlines Polly’s deprivation of liberty following her brain injury and examines how, in practice, DoLS operated for her under Cheshire West. First, I highlight how DoLS was simply not relevant for her in ways it’s obviously relevant for some other people deprived of their liberty (Section 2.1). Second I focus on how DoLS delivered some crucial benefits (2.2). Third I show that DoLS sometimes simply failed to deliver on its potential (2.3). Finally I consider how DoLS might have actually caused her harm (2.4).
Part 3 explores what Polly’s future might hold following the AGNI judgment. I reflect, in particular, on the role of objection and ‘valid consent’.
Part 1: Introducing Polly
Polly was in a road traffic accident in 2009 which left her with multiple physical injuries along with intra-cerebral and subarachnoid haemorrhage and severe Diffuse Axonal Injury, a particularly devastating form of global brain damage involving stretching and shearing of nerve fibres in the brain.
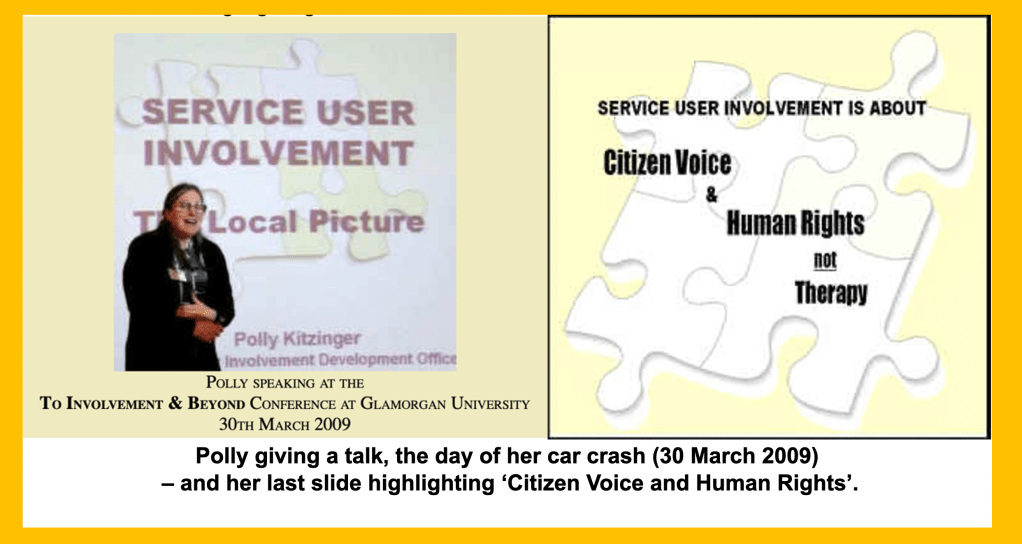
Unlike some people subject to DoLS (e.g., those with learning disabilities, whose impairments have been present since birth), people with acquired brain injuries have usually already lived part of their lives able to make what domestic law deems “capacitous” decisions. In Polly’s case, her capacitous decisions and choices were very distinctive. She prioritised freedom and adventure. Her values and beliefs were also well known by friends and family, partly because she had strong feelings about her own autonomy and also because she worked as an advocate and then a ‘service user involvement officer’ in health care settings. (For more about Polly’s work and politics, see material we’ve posted on that section of the “We Love Polly” website).
In her final job, Polly produced a leaflet about how personal stories can be used to create changes in policy and practice. It is her commitment to that, and the conversations we had as sisters about issues such as ‘privacy’ and ‘the personal is political’, which helps guide my use of her personal story now that she’s unable to author this herself, or give permission for its use.[4]
From the moment of the car crash, Polly lost the ability to make any decisions about her own medical treatment. After two years in a Prolonged Disorder of Consciousness, she eventually emerged into full consciousness with profound physical and cognitive impairments. Her presentation has fluctuated and shifted over the last seventeen years – but she’s been consistently subject to ‘best interests’ decision-making about almost every aspect of her life. For most of that time, Polly has also met the legal criteria for being ‘deprived of liberty’.
Polly was in a general hospital and then a specialist neuro-rehabilitation hospital for about a year and a half following her accident, and then moved on to a series of five different neurological rehab centres and care homes. Her care was clearly “imputable to the State” and she was “under continuous supervision and control” and “not free to leave” (the ‘acid test’ from Cheshire West in 2014).[5]
Every DoLS assessment carried out so far (these started in 2014) has found that she’s deprived of her liberty and also that she lacks capacity to consent to her residence and care arrangements because, for example, “Miss Kitzinger…presents with global cognitive impairment…disorientation to time, place and person, and lack of insight into her care needs” (DoLS form 3a, 2023). None of the extensive efforts at treatment or rehabilitation, fine-tuning pain medications, and exploration of technological aids or alternative care packages has altered this.
Polly’s physical and mental impairments severely restrict what she can do, her awareness of herself, and how she understands the world around her. She demonstrates some memory of her early life and can show flashes of compassion, intelligence and humour, but does not know that she lives in a care home (except, for brief moments, when someone informs her of this fact), and can’t remember what has happened even ten minutes ago.
She also seems to lack a sense of cause and effect: she cannot identify a source of pain or realise she needs help and then press a call bell. She is hemiplegic because her brain does not ‘recognise’ one side of her body and she’s dependent on others to hoist her out of bed, change incontinence pads, wash and dress her, spoon feed her food of the appropriate texture for her dysphagia, give medications, and transport her within, and outside of, the place where she resides.
The concept of liberty was very important to Polly, as it is to many people. It is a hugely evocative concept in politics, public discourse and in personal and family life. It’s represented by the Statue of Liberty overlooking New York harbour and personified in Delacroix’s famous painting as the bare-breasted woman leading the crowd over the barricades during the French Revolution. Liberty is symbolised by the broken chains in iconography associated with class struggle and the civil rights movement and it’s a core concept for the disability rights movement. However, as Alex Ruck Keene points out, in the law terms such as ‘deprivation of liberty’ have“autonomous meanings that do not correlate exactly with their ordinary usage”.
Polly has lived her life in the context of both the ‘ordinary usage’ of ‘liberty’ with its powerful social and political symbolism, and also the more peculiar legal definitions created by judicial interpretation of mental capacity legislation.
1953 (about eight years before Polly was born) Article 5 of the European Convention on Human Rights (ECHR), which guarantees the right to liberty and security, came into force.
1998 (Polly was in her 30s) the ECHR was incorporated into UK domestic law through the Human Rights Act 1998.
2005 (7th April) The Mental Capacity Act received Royal Assent.
2007 (1st October) The core provisions of the Mental Capacity Act [MCA] 2005 came into full force and Polly discussed this legislation with her family and prompted our mother to draft an Advance Decision to Refuse Treatment. Polly’s car crash was 18 months later (30th March 2009) when she was 48.
2009 (1st April)The Deprivation of Liberty Safeguards [DoLS] (an amendment to the MCA 2005) came into force. This was just two days after Polly’s accident, while she was still in intensive care.
2014 (March)Cheshire West– following legal proceedings based on an initial interpretation of the statutory meaning of ‘deprivation of liberty’ that played out during Polly’s early post-injury years, the definition was refined and expanded in the Supreme Court “Cheshire West” judgment in March 2014.
Polly was actively engaged with questions about ‘liberty’ (in the broadest lay sense of the term) long before she herself became subject to ‘Deprivation of Liberty’. Her views – vocally articulated before her car crash – were informed by evolving legal and political debates about liberty at the time and by our own family history and context. From childhood onwards, family conversations included: our father’s experiences in Nazi Germany and his child refugee journey to the UK; our mother’s campaigning for women’s rights in childbirth (including women in prison); and other family members’ experience of psychiatric hospitalisation and sectioning under the Mental Health Act 1983.
In adulthood, Polly’s opinions developed through her ongoing personal experiences, political activism and her professional work in diverse roles supporting people who wanted their voices to be heard, especially around health choices. This included, at one point, working for MIND as an independent advocate in a secure psychiatric unit – until she was banned from entering the premises because, in her account of this, she’d been ‘too challenging’ to the staff.
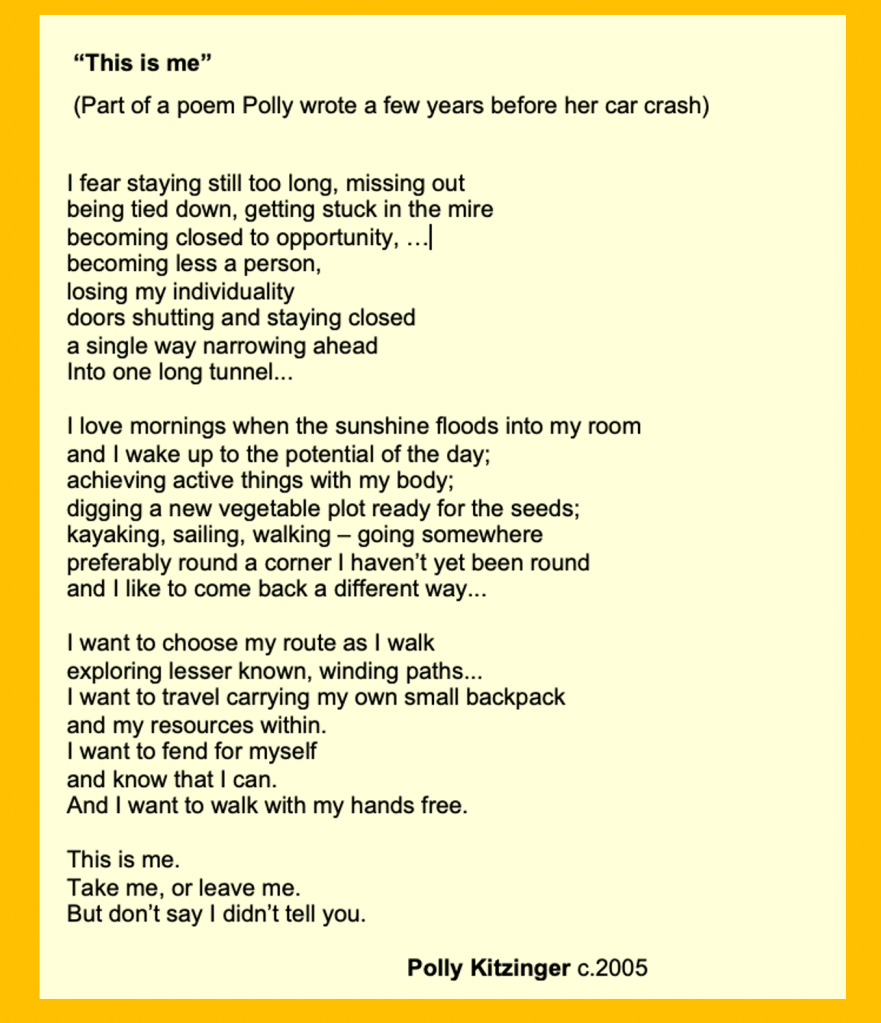
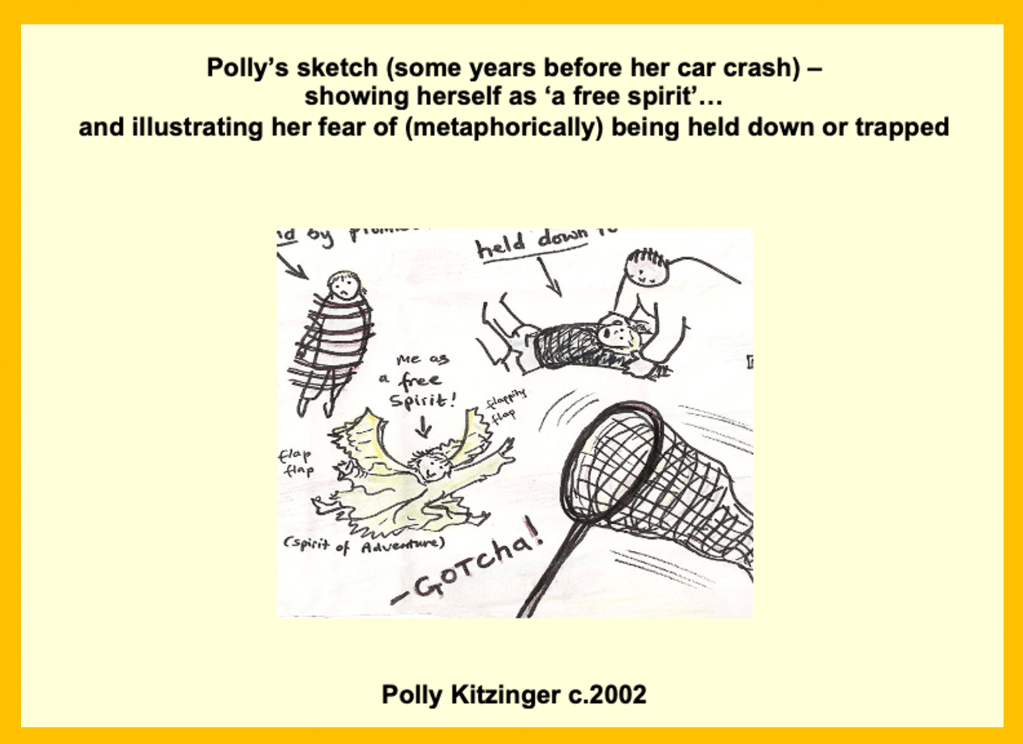
Polly was also strongly committed to her own personal autonomy. She’d refer to the fact that she’d been ‘born free’ – at home (not in hospital) in a village called ‘Freeland’; joking that this set the scene for her approach to life. She was adamant that she’d never want to live under state control, in an institution or a care home; for most her life she didn’t even want the compromises involved in sharing a home with a partner. Independence was core to her sense of self. She expressed this in the way she chose to live her life and in letters she sent us, as well as in poems and pictures.
Polly’s freedom to live her life in accordance with her own choices, value and beliefs was taken from her after her car crash. Polly’s sisters, parents and others close to her testified that Polly would not want to risk surviving with catastrophic brain injuries but doctors decided to continue to impose life-sustaining interventions upon her. Their position was supported by the ways in which the socio-medical system operated at that time. (We’ve written about this elsewhere see: “M,” Polly, and the Right to Die” and “Doctors wouldn’t let my sister die”.)
Seventeen years on, three of her sisters (Celia, Tess, and I) continue to try to fight for Polly (our parents have now both died and others close to Polly have drifted away). We keep on trying our best to mitigate the ongoing harm to her and make her life the best it can be. We take different roles.
Celia focuses on legal developments, researches key areas about Polly’s care and liaises with lawyers. She was instrumental in lobbying for Polly’s first DoLS in 2014 after Cheshire West.
Tess focuses on day-to-day support for Polly. She is most adept at understanding Polly now and helping her to communicate as much as possible. She became Polly’s Relevant Person’s Representative (RPR) once a DoLS was in place.
I am Polly’s Welfare Deputy and have responsibility for the best interests decisions authorised by my court order. I make those decisions after consulting with those involved in Polly’s care or “interested in her welfare”, and taking into account Polly’s “past and present wishes and feelings” etc. as specified by s.4 MCA 2005). A Welfare Deputy must be consulted about deprivation of liberty and can veto an authorisation but cannot give valid consent to the person’s confinement. (The same applies to anyone the person had appointed in advance as their Attorney for Health and Welfare).
Part 2:What Cheshire West and DoLS meant for Polly and her family
When the Cheshire West judgment was published in 2014 it resonated powerfully with us as Polly’s family. Its principles and its symbolism seemed hugely important. It recognised the necessity of safeguards and the responsibilities of confinement “imputable to the State”. We certainly endorsed (and still do) Lady Hale’s oft-quoted statements that “A gilded cage is still a cage”. Our mother, Sheila Kitzinger, particularly liked that statement as it connected to some of her work on power dynamics in hospital maternity services (which she originally highlighted in the 1960s in her first book ‘The Experience of Childbirth’).
The ‘gilded cage’ has continued to be a powerful metaphor for us as Polly’s sisters, in ways perhaps not intended. So far, between two and three million pounds has been spent on Polly’s care by the State (i.e. taxpayers). This is, literally, around twice her weight in solid gold (at the market price at the time of writing). Even her ongoing (now reduced) core care package is £1950 per week, ie over £100,000 a year; so this figure could increase to four million pounds given estimates of her current life expectancy. This figure would have horrified Polly who had strong views on patient-centred and just distribution of health care resources.
Expenditure does not, of course, guarantee the quality of provision, but among all the dilapidated buildings, stressed staff, under-resourced and at times chaotic health and social care system it’s also clear that Polly has sometimes had access to state-of-the art medical equipment, excellent rehabilitation facilities and some superb specialist support and day-to-day care from dedicated professionals.
The places in which she is confined have also (usually) been made to look as pleasant as possible and staff often work extremely hard to create a positive ambiance. Her first placement after leaving the general hospital was on the ward of a slightly decaying Victorian country house, adapted by the Red Cross for World War 1 ex-service men. It remained in use as a rehabilitation centre until 2020 and had a hydro-therapy pool for patients, colourful pictures on the walls, and a fish tank in the reception area.
Later she moved into modern units – designed to maximise light, air and accessibility. She currently lives in a purpose-built care home in the grounds of a former stately home. Her room has a little veranda with potted plants and the unit is as ‘normal’ and ‘home-like’ as possible. We’re pleased that Polly has a view of mature trees from her window. It’s a placement we resisted because it’s a dementia centre into which she was essentially forced when a placement needed to be found urgently, and the Health Board responsible for her NHS Continuing Healthcare package declined to fund the specialist neuro-care centre we’d have preferred – but she seems quite ‘settled’ there now. There is a simulated bar in the residents’ lounge, folded napkins on the dinner table, and regular activities such as in-house films, quizzes and live group sing-alongs.
None of this alters the fact that Polly is trapped in a life she would have refused if she’d been at liberty to do so – no amount of money can change or disguise that. ‘A gilded cage is still a cage’.
But what can (and can’t) DoLS do to help make her placements as least restrictive as possible?
The AGNI judgment prompted me to systematically review what DoLS has done for Polly in the twelve years between spring 2014 and summer 2026. I’ve organised my thoughts into four categories relating to times when DoLS has been (1) irrelevant (2) beneficial, (3) unrealised and (4) harmful.
2.1 When DoLS is irrelevant
The Deprivation of Liberty Safeguards framework is designed for a very specific purpose in relation to ‘physical liberty’ – and this is narrowly defined. The safeguards are not designed to address medical treatment as such, so trying to get a DoLS was of no use in stopping doctors from providing life-sustaining treatments contrary to what we knew would be Polly’s wishes (between 2009 and 2011). Nor did it help in challenging the associated restrictions that giving those treatments sometimes required.
By the time she did get her first DoLS (in 2014, around 5 and a half years after the car crash), Polly was no longer dependent on life-sustaining treatments such as clinically assisted nutrition and hydration so there was no obvious medical treatment we could ask doctors to withdraw. And by that time (belatedly), health care professionals concurred with family about what ceilings of treatment were in her best interests.[6]
The major residence issues that have been problematic for Polly have also often not seemed to be something DoLS can assist with. Arguments about deprivation of liberty were powerless in the context of key determinants of her placements and care such as what placements were available, what the CHC would pay for, and problems with the business models or stability of the care sector.[7]
Other situations in which DoLS is designed to help have simply not been relevant to Polly’s particular situation. There is no argument, for example, that she might have capacity to make her own decisions about residence. There’s no option to return to her own home. There are no complex discussions to be had about issues such as using the internet or going out unaccompanied (she simply can’t).
We’ve not needed scrutiny of ‘extreme’ restrictions – partly because the severity of Polly’s physical impairments means that staff can simply usually walk away from ‘challenging behaviour’ without the need for restraint. Her ability to physically self-harm is minimal and episodes of refusing food and fluid have tended to cease within 72 hours. Although we know these sorts of issues come up repeatedly in DoLS cases (especially s.21A cases) in the Court of Protection, they simply aren’t relevant for Polly. Very few cases (an estimated 1% of people with DoLS)[8] result in proceedings in the Court of Protection (some of which can bring about such vital changes for the protected party). Some lawyers are simply not very familiar with the other 99%!
2.2 When DoLS has benefits
Where DoLS has been useful is in relation to day-to-day care management issues. Ironically, this was never intended to be the purpose of DoLS (which is about the proper implementation of Article 5). However, Best Interest Assessors (BIAs) are very adept at spotting ways of improving care planning. and this has been, in practice, an important benefit to the thousands of people who have DoLS reviews, but who never make a Section 21a challenge or other court application.
The BIA is independent from both the family and the managing authority. They can bring a different focus and fresh eyes compared to those of us entangled in the morass of challenges involved in supporting a profoundly disabled person – either as a relative or as a healthcare professional. The BIA also has the authority to see all relevant documents and is recognised as an expert whose recommendations should be taken seriously – and might even recommend ‘conditions’ to the Supervisory Body which, if imposed, must be followed for the DoL to be lawful.
We’ve welcomed the fact that Polly’s BIAs can review all the documents, give close attention to Polly and her situation, and ask questions that we may not have considered. They’ve also been able to reassure staff about the use of devices such as a lap belt – underlining, for example, that staff should follow the guidance from the neuro-physio and specialist wheelchair assessor about doing up Polly’s lap belt and that this has been assessed as necessary, proportionate, and in Polly’s best interests. (The lap belt merely stops Polly sliding onto the floor; it does not prevent her moving in other ways, because she can’t.)
This never should have been an issue that DoLS needed to address of course. It should have been resolved by proper engagement with best interests, but in a unit unused to people with Polly’s type of impairment and lack of body tone, staff frequently forgot to do up the belt, and two even declined to do so when asked by me or Tess, citing ‘deprivation of liberty’ as a reason.
BIAs have also often managed to engage with Polly sensitively, listen to family concerns, and tried to maximise the ‘normality’ of Polly’s placement situation or promote her ‘access to the community’. For example, several BIA reports have stated that Polly should be included in more activities or taken out more often – and these have sometimes been set as ‘conditions’ of the Standard Authorisation.
It should not be this way of course; but our experience as family members (even when one of us is Welfare Deputy and another is RPR) is that we are often not listened to in the same way as a BIA. We can be dismissed as ‘hyper-vigilant’ or ‘serial complainers’ and we also face the complex task of trying to navigate on-going relations with care staff and organisations.
Navigating relations with staff/organisations is a particularly pertinent issue for us as we live under the shadow of Polly having been evicted from one placement after we made a series of complaints (including one about an incident of disproportionate and unnecessary use of restraint).[9] The relationships with staff became very fraught. Tess’s freedom to enter the care home was restricted – an echo of Polly’s own experience when she was banned from the premises of a psychiatric unit where she worked. Polly herself was then evicted.
Tess feels very strongly about the values of DoLS and its ability to help Polly. When I asked her about her views for this blog, she highlighted the value of being Polly’s RPR (not ‘just a sister’): “It feels like a protection for me. – that I have some validity as a visitor and someone with opinions about how my sister should be cared for. Whether that can be leveraged a tiny, tiny bit. It’s not just about whether she’s behind a locked door. It should allow me to enable her to have choices, even behind that locked door…I think DoLS is really important, it’s just another tiny corner of hope families have for making some changes.” (A longer part of this filmed interview is available at:https://www.youtube.com/watch?v=AgmtMvo2Myo).
2.3 When the potential benefits of DoLS are unrealised: A system under stress
I am less positive about DoLS than Tess. Maybe that’s because I don’t have the threat of losing the status of RPR, or maybe I have less tenacity in holding on to hope. Most of all, though, it’s because the DoLS system has often not worked as it was supposed to. The gap between the principles underpinning DoLS and the practice on the ground – and the huge unrealised potential that reflects – is crucial to considering the future of DoLS.
Our experience during the last 12 years is that DoLS has often been missing (2.3.1), ineffective (2.3.2) and/or has led to perpetuation of misleading and inaccurate information about Polly (2.3.3).
2.3.1 Missing DoLS years – unlawful deprivation of liberty
During the twelve years between 1st April 2014 (after Cheshire West) and 31st March 2026, there were, in total, almost seven years when (everyone accepted at the time) Polly should have had DoLS in place, and did not.
This surprises nobody. It’s accepted that there were simply too many cases to process after Cheshire West and that the system wasn’t equipped to deal with that volume. The result was that a large proportion of people deprived of their liberty by law, were also deprived of the safeguards that the law, in the shape of the Cheshire West judgment, had ruled should be in place to protect them. This was, as Alex Ruck Keene highlights, morale-sapping for professionals forced to prioritise who got DoLS and who didn’t; they were left effectively “having to identify how best to break the law”.
For us, as family, the message was that depriving Polly of her liberty unlawfully was not taken very seriously. It made a mockery of what had been determined by law to be Polly’s ‘rights’, reflected a gulf between law and practice, and created another fruitless task for me trying to chase up missing DoLS. The very mechanism that was supposed to “protect” her became yet another example of the broken system that now controls Polly’s life.
2.3.2 Ineffective DoLS
It’s our recurrent experience that DoLS simply doesn’t deliver on-the-ground change. For the five years when DoLS was actually in place, we were disappointed to realise that BIA recommendations and conditions often promised more than they delivered – as illustrated by the examples below
Example 1: In 2020 (maybe partly due to the start of the Covid crisis) nobody, not even the care home manager, received the relevant DoLS paperwork that should have been sent out and this was despite repeat chasing. A year later, when I was lobbying for the next DoLS, the care home manager wrote: “We never received the paperwork from the one submitted last year and we requested it several times, even during the review that was done over the phone, this was stressed out to the review officer….I will contact them immediately to submit the new application and explain that if there was any recommendations, we couldn’t have complied with them.” When I finally did receive the paperwork I found, in fact, that it had included not just recommendations, but actual conditions (for more activities and outings). These conditions had never been communicated or monitored. Ironically, and despite the failure of the DoLS, I think in practice progress had been made on these ‘conditions’, as there was good communication and collaboration with this manager and Polly’s key worker at that point. But in terms of effective operation of DoLS, it’s obvious, at the most basic level, that the value of setting “conditions” depends on communicating with the managing authority about what those “conditions” actually are.
Example 2: A couple of years later there’d been a long gap without a DoLS. The care home manager who’d sent me the email I’ve quoted above had left (as had Polly’s key worker) and there’d been a rapid turn-over of staff accompanied by an equally rapid deterioration in Polly’s care. We’d lobbied for DoLS for a long time, and kept being fobbed off with promises that it was in the system, or that an assessor had been assigned and that it would be done soon. A BIA was finally sent in – and she carried out a thorough consultation and review resulting in a detailed and extensive set of conditions. Those might have been helpful had they been imposed earlier – but, in fact, the care home closed down a few weeks later after severe staffing problems and being rated Inadequate by the CQC.
Example 3: Even when DoLS recommendations or conditions are in place and known about in a timely manner, it has taken huge efforts to deploy them in the service of even a tiny improvement in Polly’s life. It needs concerted efforts, week after week, to make progress that is often only temporary. For example, a “condition” stating that Polly should have the opportunity to be taken out of the care home at least once a week may be thwarted by, for example: first finding that her large wheelchair can’t be safely accommodated in the care home van along with other residents that are to be taken out that day; next, when they finally get her into the van, finding the necessary securing tension strap is broken; the third week there is no outing at all because the driver is off sick, and there is no cover. Other reasons outings didn’t happen have been that the van is needed for another resident’s hospital appointment, Polly herself has an unannounced visit from the dentist and we decide that should take priority, or Polly is too exhausted or agitated at the scheduled day and time. When it finally does happen, the “outing” may constitute nothing more than being put in a van and driven around a lake without even being taken out of the vehicle. But Polly has “had an outing” and the box for that week is ticked, on paper at least.[10]
Example 4: There is considerable variability in the skills and practice of BIAs (or perhaps challenges they face with conditions of employment and pay). This can mean the whole DoLS process is at best a lost opportunity. The BIA who assessed Polly in 2025 did not contact us in advance of going to see her. This meant that neither Polly, nor he, could benefit from what we might have told him in advance, nor could we offer to provide Polly with communication support. He only rang Tess (Polly’s RPR) and me (Polly’s Welfare Deputy) the week after seeing her – and then informed us he urgently needed to submit the report by the end of that day. My initial conversation with felt too brief (I was travelling at the time): he did not get back in touch when I asked him to, nor did he discuss his report with us in advance of submitting it, as some BIAs have done in the past. His report included significant errors of fact.
2.3.3 DoLS paperwork can perpetuate misleading information and errors of fact
I have become accustomed to sometimes ignoring and sometimes playing ‘whac-a-mole’ with the misinformation that frequently results from the copy-and-paste process of paperwork about Polly. Inevitably, BIAs are having to edit and process unfamiliar information at speed and the relevant forms often seem to involve the need for multiple repetition of similar information in different ways, without those completing the forms always having access to the relevant authoritative source. This means out-of-date information lingers and other information morphs and changes to the extent that it sometimes ceases to bear much relation to reality. The format of the forms themselves seem to breed data degeneration.
Even when reviewing the DoLS documents produced by the professionals I think were good there are errors. For example: one report says that the BIA consulted Polly’s sisters and her children (she doesn’t have any children). Another DoLS document says that Polly kicks out at staff with both legs (she can’t – she’s paralysed down one side). A third states that Polly is being taken on visits to her family home – but this was claimed long after our father had died and the family home had been sold
Some of the reports include what might pass as detailed legal analysis if we didn’t suspect it was simply cut and pasted from another source. In assessing Polly’s understanding of the salient points about her care and the impact of her brain injury on her decision-making, one assessor cites Derbyshire CC v AC, EC & LC [2014] EWCOP 38 and PC and NC v City of York 2013 and refers to the “Causative Nexus” (Form 3a, 2023a). Another assessor claims to use ‘the Guzzardi framework’ to analyse the restriction on Polly (Form 3a, 2025). It’s superficially impressive – but it feels as if Polly herself has become lost in the process. In some reports the tell-tale signs of copy and paste are sometimes betrayed by pronoun changes (e.g. Polly is referred to as ‘he’ and ‘him’ mid-sentence) or odd shifts from “Miss” or ‘Ms’ to ‘Mrs’ (she was never married and would have vehemently objected on feminist grounds to both “Miss” and “Mrs”).
Forms also include slightly bizarre statements such as “Miss Kitzinger has no awareness of what is a healthy balanced diet” or “If she left by herself she would become lost” (Form 3, 2017). These are bizarre (to us) because planning a balanced diet or finding her way around are so remote from Polly’s actual capacities as to sound fanciful. Apart from propelling herself from bed to crash mat when thrashing during periods of agitation, Polly can’t independently mobilise at all.
Errors and irrelevances sometimes result from what we have come to think of as ‘performative personalisation’. By this we mean that professionals attempt to display familiarity with the individual, and to demonstrate that they’re considering Polly’s best interests ‘as a person’. Of course, acknowledging who the person is/was can be done skilfully and well – and we appreciated the BIAs who took the time to listen and acknowledge something meaningful about Polly. But some assessors’ representations of who Polly is/was can be very shallow and unconvincing.
The 2025 DoLS paperwork is a prime example. The BIA reproduces incorrect information from earlier forms and adds some additional factoids of his own.
Form 3 asserts that Polly was born in Oxford: she was not – and the fact that she was born in Freeland was, as I’ve highlighted earlier, very important to her. It says that she also went to school in Oxford. She did not. It reports that: “At school, she enjoyed drawing and writing poems. She did not like Maths” (Form 3, 2025). Unlike the first two ‘pseudo-facts”, this last point is true, but seems a strange thing to highlight. We haven’t been able to trace where the BIA obtained the ‘dislike of Maths’ factoid: it’s certainly not information we would ever have raised as relevant to DoLS, but was perhaps something one of us mentioned in passing to a carer or activity co-ordinator. It seems very odd to put this on a DoLS form, over 40 years after she left school.
More seriously, under the heading ‘Past View” the BIA went on to state (manifestly falsely) that: “There is no information on record of an advance decision or past views/wishes expressed by Ms Kitzinger in relation to care/accommodation”. I don’t suppose anyone reading this blog post will be surprised to learn that I’ve placed a one-page summary about Polly’s “past views/wishes” with her hospital admission pack, alongside my detailed and evidenced Welfare Deputy report. There are also, of course, the public statements we’ve made about Polly’s past values, feelings, wishes and beliefs, including an interview with BBC news.
The final paperwork from the Supervisory Body states categorically: “The Supervisory is satisfied that the Best Interests Assessor is assured that there is…no Deputy for Health and Welfare”. Who can have “assured” this BIA that there is no Deputy for Health and Welfare? Certainly not me, her Deputy for Health and Welfare. How can the Supervisory Body be “satisfied” that the BIA is so “assured”? The fact that this form was signed off and filed to “protect” Polly and “safeguard” her is ironic. It was probably “just” cut and paste – but it’s an egregious error.
In the 2025 DoLS documentation, Polly’s identity as an adult and the extensive evidence of her strong values and beliefs (her sisters’ ability to represent these and my particular role in promoting her best interests) is simply erased. The documentation leaves a gap between Polly as a schoolgirl who didn’t like Maths and Polly as the care home resident she is today – the Polly we knew for her entire capacitous adult life is rendered invisible.
2.4 DoLS Harms
All interventions (whether administrative or medical) can carry both benefits and harms – the point is to be aware of the potential for both, and to maximise the benefits and minimise the harms.
Mostly I’ve felt that DoLS has not harmed Polly directly, but reviewing relevant documentation for this blog has led me to revise this opinion a little.
The spectre of DoLS, and (erroneous) views about it by front line health care staff, may sometimes have interfered with thoughtful best interests decisions and care for Polly. For example, in October 2014 (just after we’d successfully initiated the first DoLS process) we discovered that Polly had been left in bed for over a week. This was contrary to her care plan and therapists’ advice, especially in relation to managing her chronic pain at that point. There was no evidence that any significant time had been spent reassuring Polly ahead of the necessary hoisting or even giving her a reason for getting out of bed (such as an opportunity to be taken out of the care home). The manager’s response to our complaint was that this decision accorded with Polly’s own wishes not to transfer to her wheelchair. She wrote: “There is no Deprivation of Liberty safeguard in place for Polly and as such we need to remain responsive to her wishes as she indicates them“. The letter concluded with the result of the investigation of our complaint: “Outcome – Unsubstantiated” (Letter from manager, 22nd October 2014). This illustrates the anxiety staff may have about attempting to persist with some interventions when a person says no. It also reveals a confusion between DoLS and Best interests.[11]
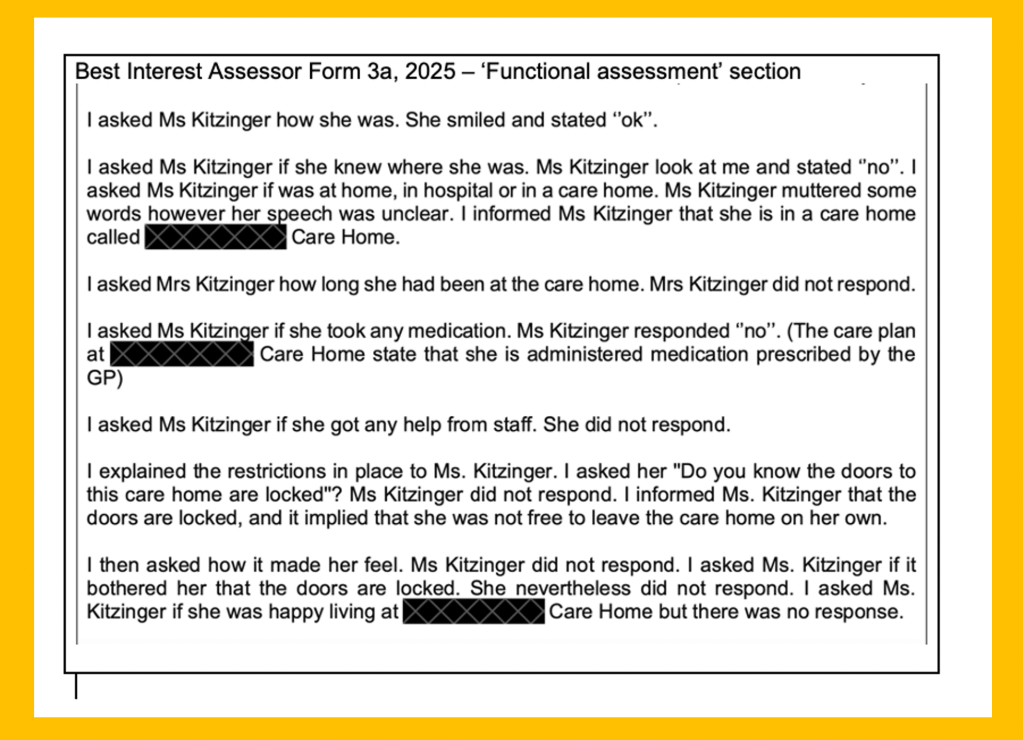
The second potential harm to Polly relates to the assessments themselves. It’s well-documented that some care home residents experience the BIA process as intrusive or distressing (see, for example, “A court hearing and 23 visits from 16 officials”). I do not think Polly has usually experienced them this way – not least because Tess has usually been there to mitigate any distress that might result from the questioning and to ensure that Polly is understood as much as possible (Polly’s speech is very limited and difficult to understand). However, looking closely at the report from the BIA assessor in 2025, I think this assessment may have caused distress. This was the year we received no prior notice of the assessor’s visit to Polly: he met her with a ‘senior carer’ but no family member. He describes arriving to find Polly relaxed, calm, and alert, but his account suggests to me that she quickly became disengaged. Here’s his record of the interaction:
Best Interest Assessor Form 3a, 2025 – ‘Functional assessment’ section
I do not think this was handled well. We know from our own interactions with Polly that when told she’s in a care home, she can respond with shock and repeatedly ask ‘Why? Why? Why?”. She can also become distressed when quizzed about a reality she does not recognise (e.g. that she needs support and is living in a locked environment). I suspect Polly forgot this encounter within minutes – and I hope any distress it caused faded quickly too. But I’m going to request that in future no formal assessment on Polly is done without informing me or her RPR in advance and ensuring that Polly has the option of having one of us present for the assessment.
3. Looking to the future: objection and consent
I assume there will be at least one last DoLS assessment of Polly to check whether or not she remains eligible for DoLS. The multi-factorial approach will necessitate some consideration of objection, and I suppose it’s possible it might also (depending on the flow chart followed) consider the concept of ‘valid consent’. In this last section, then, I want to reflect on how Polly’s behaviours and views in these domains were interpreted prior to the AGNI judgment, and how this might be different post-AGNI.
On objection: For almost ten years after Polly regained consciousness she could display very “challenging behaviour” and what the nursing assessments record as “violence against herself and others”. This necessitated funding for one-to-one support at times and specific management strategies. Sometimes the ‘triggers’ could be clearly linked to specific actions (such as giving personal care), her chronic pain, or sources of obvious frustration (such as no one being able to understand what she was trying to say).
But sometimes no specific ‘trigger’ could be identified (in spite of all the ABC charts and monitoring) and at times there were intense periods of shouting and kicking and refusing care and treatment, as well as food and water. The most intense episodes could be accompanied by increased lucidity and ability to communicate. They seemed linked to internal distress; she could occasionally shout or write legible words during these episodes – sometimes recording emotions and desires including, on one occasion, quite remarkably, writing: ‘I‘m thinking how to die’, ‘kill me’, “I need to kill myself”. A psychiatric assessment was carried out in 2012 using an ‘Ill-being’ scale’: it gave Polly the highest possible ratings on all dimensions including: “shows signs of feeling depressed or despairing”, “shows intensely angry or aggressive behaviour”, and “shows signs of grieving over losses”.
Polly’s “challenging behaviour” or expressions of distress have never been interpreted as Polly objecting to her placement. Nor has documentation of her prior wishes (never wanting to live in an institution or care home) ever been used to inform such a conclusion. She no longer displays such behaviour – but were these episodes to recur, I think it looks like ‘objection’ might get more attention in the post-AGNI legal, policy and practice landscape (e.g., see AGNI para 145).
On ‘consent’: Ironically it is ‘valid consent’ which now, at least in theory, might be more relevant to Polly (if the objective measure for ‘deprivation of liberty’ were to be met, which I don’t think it will be). Polly’s behaviour has changed dramatically in recent years. She is now super-compliant and seems eager to please. She may still briefly become agitated by things such as if another resident who is mobile walks into her room and touches her – but otherwise Polly seems not to complain about anything; in fact she seems no longer to attempt to communicate her experience at all. Her care notes record her as “settled” and “cheerful”.
A recent psychiatrist’s report prepared for the last DoLS writes that Polly is “very compliant” and is “happy with her care” (Form 4, 2025). She often smiles a welcome to people who come into her room and starts shouting “I love you” repeatedly over and over again (to care staff, GP, dentist, and to the best interests and mental capacity assessors). When, a few weeks ago, Tess tried to explain to Polly that she was living in a care home and ask her about her experience of it Polly replied “I love you”, then “you’re lovely’. When Tess again prompted Polly to talk about the care home she responded “it’s lovely”.
I would like to think some of the changes in Polly’s presentation might be linked to changes in her actual experience. I don’t think she’s got the memory or processing power to ‘adjust’, ‘come to terms’ or discover new meaning in a radically changed life (a common journey eloquently reported by people facing sudden-onset physical disabilities such as spinal cord injury). But perhaps her brain has changed in ways that mean she’s less tormented by flashes of memory or insight that seemed to me to be associated with the earlier most intense and sustained outbursts of rage and distress. I wonder if she’s now developing post-brain-injury dementia and losing a deeper layer of memory in some way. Or perhaps her care and the nature of her placement has changed in ways which keep her calmer?
But I also see the force of the explanation advanced by my sister Tess, who is closest to Polly – and her perspective is much more disturbing. She believes the changes in Polly’s behaviour were, in part, linked to the Covid restrictions, when we were often unable to visit her. The effects of the pandemic lockdowns were exacerbated for Polly as staffing and management of her care home deteriorated. Its CQC rating dropped from “Outstanding” to “Inadequate” – with failures in safety, caring, effectiveness, responsiveness and leadership. The CQC report records that “Staff members did not always treat people with warmth, dignity and respect” and “People were not always supported to have maximum choice and control of their lives and staff did not always support them in the least restrictive way possible”. Tess says that Polly simply “gave up on fighting her corner”. She has been finally “broken-in”, her emotions “flattened”, she no longer expresses some of her needs: “It’s almost like there was no other way for her to exist but to become compliant and lock the frustration away and hide the key”.
This remains true even in the new placement she moved to – with kind staff, who are clearly fond of her, and committed to respecting her choices where ever possible and supporting her the best they can. This ‘new Polly’ will now assent to almost anything. After noticing her front teeth looked loose and askew, for example, I discovered that carers had taken a dental bridge that had broken off – and been repeatedly reinserting it into her mouth (apparently under the mistaken belief it was a form of denture). She’d passively accepted, without protest, the reinsertion of the metal spike into her jaw, and the consequent lopsided bulge in her mouth as it worked loose again. On another occasion Tess tasted a spoonful of the food she’d been given to feed Polly with, only to find it had a yoghurt topping containing bitter medications – which should have been given separately and overtly by a nurse. Polly had been accepting the food and indicating that it tasted good – though it can’t possibly have done! Tess says: “She is very vulnerable in every way. She’s vulnerable to people deceiving themselves into thinking everything’s okay when it’s not. I wish she could protest more… This is a big problem because she doesn’t complain. They think they’re doing really well and they don’t understand why I have issues with some of the care“.
Although I have been somewhat reassured by the sophisticated understanding shown by BIAs when discussing how people might present, and a clear reluctance to take ‘consent’ at face value, I do share the widely expressed concerns that ‘valid consent’ is open to misinterpretation and may result in making vulnerable people more vulnerable.
4. Conclusion
Polly’s life for the last 17 years has been radically different from how she lived her life when she was free to make her own choices. She has irrevocably lost her ‘liberty’ – in the sense in which she interpreted and valued it. She would have defined herself in this situation as someone with ‘no liberty left to lose’ as she understood the concept.
We are left trying to ensure ‘person-centered’ care for her in the situation she is now in, navigating ‘best interests’ decision-making and attempting to minimise restrictions, maximise opportunities, and support what few choices she can still make.
The framework put in place by the Deprivation of Liberty Safeguards has enormous symbolic (and some real) power – and that framework has been one of the few mechanisms for regular independent review, on which we have rested our hope for improvements in her care. We have valued the intervention of skilled and knowledgeable Best Interests Assessors. But the system has also been frustrating, not always fit for purpose, and can cause harm.
Despite all this, we are deeply worried by the likely removal of safeguards from Polly. We can only hope that whatever other supports and safeguards are introduced to replace or supplement DoLS will offer something better for Polly and others like her – especially in relation to her Article 8 rights. Perhaps our family experience, as described here, can contribute in some small way to those future developments.
[1]“A Reference by the Attorney General for Northern Ireland of a devolution issue under paragraph 34 of Schedule 10 to the Northern Ireland Act 1998” [The AGNI judgment] https://www.supremecourt.uk/cases/uksc-2025-0042
[5] P v Cheshire West & Chester Council & another; (2) P & Q v Surrey County Council
[6]Lindsey Briggs brought an application under s.21A MCA 2005 challenging the DoLS authorisation in place at the hospital where her husband was being treated (and being given life-sustaining treatment in a minimally conscious state). She did so on the express basis that a s.21A application would allow her to claim legal aid on a non-means-tested basis – thus supporting legal representation to be able to argue her case that continuation of CANH was not in her husband’s best interests. The Court of Appeal in Director of Legal Aid Casework and others v Briggs [2017] EWCA Civ 1169 found that the Mr Justice Charles (in the original COP judgment on this point) had been in error in finding Mrs Briggs’ application under MCA 2005, s.21A, appropriate in these circumstances. Lady Justice King commented that: ‘section 21A goes to a consideration of whether the detention or deprivation of liberty is itself in P’s best interests and, while the surrounding circumstances are part of the picture, the question is not whether the circumstances, including the medical treatment P requires, (which amount to a deprivation of liberty), are in the best interests of P, but whether it is in the best interests of P to be a detained person.’ https://www.anthonycollins.com/insights/ebriefings/withdrawal-of-life-sustaining-treatment-and-mental-capacity-director-of-legal-aid-casework-and-others-v-briggs/
[7]I’m grateful to Lucy Series for drawing my attention to proposals by the Law Commission 2017 (paragraphs 9.27 – 9.28) to remove the ‘best interests’ criteria for authorising a deprivation of liberty. This was on the grounds that, in practice, authorisations often have to be made that are not in the person’s best interests but are the only available option. The notion of “best interests” adds nothing to the requirement that the DoL should be “necessary” and “proportionate”. (See also the judgment by Cobb J in North Yorkshire CC v MAG).
[8]Lucy Series writes: “There are no statistics on rates of appeals under the DoLS, but a best estimate puts the rate of appeal at fewer than 1% of people subject to a DoLS authorisation during 2017, and under 0.5% of DoLS applications overall” (Dr Lucy Series, Cardiff University, Evidence to JCHR on MCA DoLS, March 2018 (https://committees.parliament.uk/writtenevidence/87756/html/#_ftnref6.)
[9]Tess’s written complaint to the home manager recorded that she’d entered Polly’s room to see a carer holding down Polly’s right hand (the only one she can use) and the nurse spooning liquid medications into Polly’s mouth: “Polly was fighting it. When Polly began to choke, [the named nurse] said: ‘you see what happens when you make a fuss’ and spooned more medicine into Polly“. Tess’s formal complaint highlighted that Polly’s Speech and Language Therapist had advised that “Polly is not supposed to be given any liquid before it is thickened to a ‘whipped cream’ consistency” and “If a patient begins to choke I understand that a carer is supposed to wait at least 5 minutes or until their voice sounds clear and non watery before putting more in their mouth. [named nurse] failed to do this“. Tess also pointed out that the nurse’s comment to Polly (“see what happens when you make a fuss“) was “inappropriate especially given Polly’s level of distress and her communication and cognitive impairments“. We never witnessed such behaviour again but the fact the nurse (supported by the carer) did this as Tess entered the room, left us concerned about what might have happened leading up to this incident, and what staff might do and say to Polly when family were not present. On another occasion when I witnessed restraint that might have been disproportionate (involving staff in a different placement), I took out my phone and asked Polly if she’d like me to film what was happening – Polly nodded. As I started filming the two staff members immediately let go of Polly and stepped away, one saying in alarm, “It will look like restraint” – a comment that I thought was revealing in itself. It underlines the importance of outside scrutiny and ‘bearing witness’.
[10]There’s a huge gulf between the expectations Polly’s care homes set for outings and our own aspirations – some of which we’ve managed to achieve as a family, albeit with a great deal of time, repeated effort and flexibility. In Autumn 2010, before I understood how narrowly ‘outings’ and ‘access to the community’ are often interpreted, I produced a list of suggested trips out for Polly’s new placement based on things we’d already tried. This list now seems rather laughable. It included: “Craft fairs (especially if Polly is able to handle the objects)”; “Music events (she has tolerated short sessions …although be aware she may interrupt with sudden shouting)”; “Art Galleries (Polly was a keen artist – and one trip to an art gallery seemed particularly to engross Polly, although subsequent such visits have generated less interest)” and “Festivals (her sisters took Polly to the gay and lesbian Mardi Gras – and Polly was fascinated by the drag queens)“. (‘Service User’s Perspective: transfer summary for Polly Kitzinger’, Jenny Kitzinger, Welfare Deputy Report No 3. October 12th, 2010).
[11]I wonder if staffing shortages may also have come into play as 3 staff members were required to hoist Polly safely at this point and it took a long time to do it gently and appropriately. Working with family to support the transfer or having us there to suggest an outing with her sisters might also have been helpful, but there was little collaboration with us at this point. A formal eviction letter arrived for Polly the following month.
Endnote by Daniel Clark
Back in 2014, In Cheshire West, the Supreme Court considered the meaning of a deprivation of liberty (DoL) through reference to Article 5 of the European Convention on Human Rights. Lady Hale, giving the majority but not unanimous judgment of the Court, presented an ‘acid test’ for deprivation of liberty: is a person under continuous supervision and control, and not free to leave?
On Tuesday 2 June 2026, the Supreme Court handed down judgment in what is increasingly being referred to as “AGNI’ (the case was brought by the Attorney General of Northern Ireland). The Supreme Court overturned Cheshire West, finding the acid test to be wrong in law, and directed a different approach.
First, the identification of the objective element of a deprivation of liberty must entail a multifactorial analysis, which includes consideration of the intensity and purpose of confinement. If these conditions are not satisfied, there is no deprivation of liberty.
Second, a person may lack capacity to make decisions about their care and residence but can nevertheless give valid consent through an expression of their (positive) wishes and feelings. If a person is giving such consent, they are not deprived of their liberty.
To access the judgment, see: Judgment (PDF) (hyperlinked)
To access the court’s approved press summary, see: Press Summary (PDF) (hyperlinked)
If you would like to contribute a commentary about this judgment, please contact openjustice@yahoo.com, and mark your email for the attention of Daniel Clark.
Editorial Note: This is the fourth ‘commentary’ blog post we have published in the wake of the Supreme Court decision, handed down in June 2026, changing more than a decade of law and practice on ‘deprivation of liberty’ (see Endnote for more information).
Prior to the Supreme Court’s judgment, I wrote about the enduring tensions arising from Cheshire West. My central argument was that, although Cheshire West was grounded in the important objective of protecting vulnerable individuals through Article 5 of the European Convention on Human Rights, it expanded the concept of deprivation of liberty to such an extent that it blurred the distinction between necessary care arrangements and state-imposed restrictions. In practice, this created significant challenges for families, practitioners and public bodies seeking to balance autonomy, protection and proportionality.
The approach of the majority in Cheshire West reflected a deliberate policy choice. Recognising the particular vulnerability of people who lack capacity, the court favoured a broad interpretation of Article 5, arguing that where there was doubt, the law should “err on the side of caution” so that individuals benefited from independent scrutiny of whether their care arrangements remained in their best interests.
Over time, however, this approach arguably created an expectation that Deprivation of Liberty Safeguards could address wider safeguarding and social care concerns that were never intended to be resolved through the DoLS framework alone.
The Supreme Court in AGNI has now endorsed a different approach, concluding that these wider safeguarding objectives should primarily be achieved through existing statutory frameworks rather than by extending the scope of Article 5.
The concerns expressed by some charities following the judgment illustrate how strongly Article 5 safeguards have come to be viewed as the principal mechanism for protecting vulnerable people. While those concerns are understandable, AGNI challenges practitioners to adopt a more holistic approach to safeguarding: one that relies on effective implementation of the Human Rights Act, Mental Capacity Act, the Care Act and wider safeguarding duties, rather than expecting deprivation of liberty safeguards alone to fulfil that role.
However, the judgment also raises important questions. While the Court criticised Cheshire West for allowing DoLS to compensate for wider policy shortcomings in safeguarding systems, I believe it could be argued that AGNI was also partially influenced by policy considerations, particularly the unsustainable volume of DoLS applications and the practical difficulties of administering the system. This impression is reinforced by the Court’s discussion of the consequences of Cheshire West, particularly in paragraphs 103–109 of the judgment.
In seeking to restore proportionality, there is a risk that the pendulum may have swung too far in the opposite direction. The judgment provides numerous examples of circumstances that will no longer amount to a deprivation of liberty, but comparatively few examples of the types of cases that are likely to satisfy the revised threshold.
This may leave practitioners questioning where the new boundaries now lie. Greater clarity will no doubt emerge through national guidance, case law and practical examples, enabling professionals to develop a more consistent understanding of what constitutes a deprivation of liberty under the new legal framework.
The task of balancing competing human rights will continue to present challenges. Practitioners will continue to grapple with the challenging task of doing their best to reconcile respect for personal autonomy and private life under Article 8 with the need to safeguard individuals and protect life and physical integrity under Articles 2 and 3.
One of the notable features of AGNI is its attempt to navigate this balance by giving due weight to a person’s wishes and feelings, thereby promoting respect for privacy, dignity and autonomy, while also recognising the need for protective intervention where individuals are subject to coercion, are objecting to arrangements, or otherwise meet the criteria requiring formal legal safeguards.
Implementation and Training
The key challenge now lies in implementation. The Mental Capacity Act continues to be applied inconsistently in practice, and practitioners will require ongoing training, guidance and support to ensure that it is used effectively to safeguard individuals while appropriately balancing competing human rights considerations.
In my role as an MCA Lead and Chair of the National Healthcare MCA Community of Practice, I have repeatedly seen and heard examples across both health and social care systems where practitioners mistakenly view Mental Capacity Act assessments and best interests decision-making as specialist functions that sit primarily with Best Interests Assessors. The CQC’s State of Care (2024/2025) report continues to highlight the poor application of the MCA in practice across both health and social care including poor understanding of Deprivations of Liberty processes.
Too often, relevant capacity assessments and best interests decisions are not undertaken by frontline practitioners because it is assumed that these matters will be addressed later by a BIA, only for practitioners to discover that this is not so when the BIA turns up to complete their assessments for DoLS.
One positive consequence of the AGNI judgment may be that it encourages professionals to refocus on their own responsibilities under the Mental Capacity Act. By reducing the number of cases that require formal deprivation of liberty authorisation, there is an opportunity for practitioners to develop greater confidence in undertaking capacity assessments, making best interests decisions and applying the Act in day-to-day practice.
However, this will only be realised if significant investment is made in training, supervision and legal literacy across the workforce. Successful implementation of AGNI will depend not simply on understanding the judgment, but on equipping practitioners with the knowledge and confidence to apply it in complex, real-life situations. Training should move beyond traditional classroom teaching and place greater emphasis on practical, case-based learning using realistic scenarios that reflect the complexity of day-to-day practice.
Practitioners will need support to understand new concepts such as “valid consent”, how to interpret a person’s wishes and feelings, and how to distinguish between expressions of contentment, acquiescence and genuine consent. Equally important will be developing confidence in recognising objection, understanding the significance of different forms of restraint, and balancing competing rights under the Human Rights Act within the framework of the Mental Capacity Act.
Training should also help practitioners develop the professional curiosity to look beyond a person’s outward presentation, recognising that compliance or apparent happiness does not necessarily equate to freely given consent. National guidance, practical case studies and opportunities for reflective learning will be essential to build legal literacy and promote consistent decision-making across health and social care.
Above all, successful implementation of AGNI requires practitioners to return to the fundamentals of the Mental Capacity Act. A sound understanding of its core principles, supported by practical application rather than theory alone, will be the foundation for ensuring that the judgment is implemented lawfully, confidently and in a way that genuinely safeguards the rights, wishes and wellbeing of those it is intended to protect.
The judgment also arrives at a time when many local authorities continue to face significant pressures, including large numbers of individuals awaiting allocation for Care Act assessments and support planning. Against this backdrop, it is essential that AGNI is not viewed as a solution to wider systemic challenges. Rather, it should be seen as one part of a broader safeguarding framework that relies upon effective implementation of the Mental Capacity Act, the Care Act, the Human Rights Act and, where relevant, Children’s Act 1989, particularly for 16- and 17-year-olds.
Alongside formal training, there should be a national commitment to strengthening Mental Capacity Act Communities of Practice and practitioner forums. These provide invaluable opportunities for professionals across health, social care and other sectors to share learning, useful tools/resources, discuss complex cases, identify emerging challenges and promote consistent application of the law.
They also offer an important mechanism for identifying recurring themes from frontline practice that can be escalated to policymakers and those developing national guidance, helping to ensure that future guidance is informed by the realities of practice and is meaningful not only for professionals but also for individuals, families and carers.
We now await further detailed national guidance and case law to provide greater clarity about the criteria of deprivation of liberty as defined in AGNI.
AGNI is here to stay, and we should embrace it pragmatically. Its emphasis on hearing and respecting wishes and feelings aligns closely with the principles of the MCA, the Care Act and children’s legislation.
Mary Kadzirange has a legal background and is a Registered Mental Health Nurse and a practising Best Interests Assessor. She is the Mental Capacity Act lead within West Yorkshire Integrated Care Board’s safeguarding team. She is Chair of the National Health MCA Community of Practice and of the West Yorkshire ICB Race Equality Network.
Endnote by Daniel Clark
Back in 2014, In Cheshire West, the Supreme Court considered the meaning of a deprivation of liberty (DoL) through reference to Article 5 of the European Convention on Human Rights. Lady Hale, giving the majority but not unanimous judgment of the Court, presented an ‘acid test’ for deprivation of liberty: is a person under continuous supervision and control, and not free to leave?
On Tuesday 2 June 2026, the Supreme Court handed down judgment in what is increasingly being referred to as “AGNI’ (the case was brought by the Attorney General of Northern Ireland). The Supreme Court overturned Cheshire West, finding the acid test to be wrong in law, and directed a different approach.
First, the identification of the objective element of a deprivation of liberty must entail a multifactorial analysis, which includes consideration of the intensity and purpose of confinement. If these conditions are not satisfied, there is no deprivation of liberty.
Second, a person may lack capacity to make decisions about their care and residence but can nevertheless give valid consent through an expression of their (positive) wishes and feelings. If a person is giving such consent, they are not deprived of their liberty.
To access the judgment, see: Judgment (PDF) (hyperlinked)
To access the court’s approved press summary, see: Press Summary (PDF) (hyperlinked)
If you would like to contribute a commentary about this judgment, please contact openjustice@yahoo.com, and mark your email for the attention of Daniel Clark.
In the aftermath of AGNI, I’ve watched many hearings where judicial determination as to whether or not P’s residence and care arrangements amount to a ‘deprivation of liberty’ has been deferred to a later hearing, apparently in the hope that there might be greater clarity by then as to how that determination should be made. But many of us are looking to judicial decision-making to understand how the AGNI judgment is implemented by the courts.
This is only the second case I’ve blogged about where a court has made a post-AGNI ‘deprivation of liberty’ determination (there are three more in the pipeline).
My first post-AGNI DOL blog reports on a case where the judge determined that there is a ‘deprivation of liberty’ for a person undergoing serious medical treatment under general anaesthetic in hospital (‘Judge authorises medical treatment and DOLS in hospital”).
In this, my second reported case, a judge determined that there is no deprivation of liberty for a young woman living under constant supervision and control in an annex to the family home. HHJ Burrows found, in accordance with the AGNI ‘clarification’ of an Article 5 compliant definition of ‘deprivation of liberty’, that she is not so deprived – and it was clear from his comments in court that he did so with considerable reluctance, referring to “deeply philosophically difficult” arguments.
The young woman at the centre of this case (COP 13189539) is in her 20s with complex needs and a severe learning disability. She has refractory epilepsy with multiple daily seizures and severe curvature of the spine that necessitates use of a wheelchair. She receives 24/7 care and is routinely monitored using CCTV cameras. Proceedings were initiated by the local authority in April 2024 (so more than two years ago) seeking (a) a declaration that P lacks capacity in relation to residence and care, (b) a determination as to whether the arrangements in place for her residence and care are in her best interests, and (c) authorisation of a community ‘deprivation of liberty’ order.
It’s taken a long time to reach a final hearing, in part because one of the previous judges allocated for the final hearing recused himself (DJ Manasse, in October 2025) and then his replacement (DJ Bland) sadly died before the hearing listed for March 2026. The case eventually came before HHJ Burrows on 30th June 2026 for final determination.
A complex case
The word “complexity” was used multiple times during the hearing. I think I heard the judge say that the bundle runs to 1036 pages. It was listed for a full-day hearing.
Unfortunately, given this ‘complexity’, the court did not respond to my request for disclosure of position statements or (failing that) for the three Gardner documents (i.e. those documents which “must” be – but probably were not – provided to the court according to PD4B para.4.2(a)-(c) COPR 2017, namely (a) the case summary, (b) a chronology of relevant events; and (c) the issues for determination at the hearing). It’s possible that my request never made its way to the judge – which is what I’ve been told in other hearings, there being no system in place for relaying observer requests to the court. So, this report is written simply on the basis of what I heard during the hearing and relies only on my contemporaneous touch-typed notes. I’m grateful to the judge for requesting, and to the applicant counsel for providing, an oral summary of the case – but it’s hard to capture the details at speaking speed: a document is far preferable for accuracy of reporting.[1] What follows is what I understood of the case, reported as accurately as I can under the circumstances.
Residence and care arrangements
First, P is in receipt of a personal injury settlement calculated on the basis of one-to-one support during the day and sleeping support at night, with a projected life expectancy of seventy-one. In fact, for the last five years her needs have increased and are greater than originally projected: she’s been receiving two-to-one daytime support and waking night care. The financial deputy appointed by the court is concerned that, with this model of care, her funds will be exhausted by the time she is in her early thirties. However, nobody actively disputes that the current level of support is in her best interests, despite its financial consequences.
Second, the family has installed CCTV cameras inside the annex in which P lives and there’s been ongoing dispute about the use of cameras and about the retention of data from them.
Neither the local authority nor the Official Solicitor (OS) considers that the camera in the bathroom is in P’s best interests. It’s apparently there “for P’s safety following incidents with staff” (the judge confirmed “she’s never alone in the bathroom?”/”No”). The parents reported in court that they have now disconnected it – so this is no longer a matter of dispute.
A camera above her bed is used to monitor her during the night – with the waking night carer in a separate room, observing P on an iPad. The judge asked, “Wouldn’t the alternative be that carers sit in the bedroom staring at her – so in terms of proportionality, this is less intrusive”, which was accepted by the OS – although there seemed to be some doubt that waking night care was actually necessary (I think only on the grounds that it had not originally been provided for in the personal injury settlement).
The camera in the lounge is also contentious. According to the OS, the family at one point said that it was for P’s safety and for safeguarding, to monitor incidents with staff, e.g. “bruising and the cause of that”. But “now they [the family] say it’s in relation to staff training and the sharing of videos with clinicians” (said the OS). In particular, the family claim there is a need to monitor seizures and determine what might be triggering them. The case manager now supports the use of all the (currently operative) cameras – having changed her mind from an initial reaction that they were not the least restrictive option, to a position (as she got to know P better) where she says that non-clinical staff are “struggling to recognise the seizures which are sometimes very difficult to spot”.
By the beginning of the afternoon, the judge said he “was of the view that all the cameras [currently in use] are reasonable and necessary within the terms of Article 8. It seems to me that [the camera in the lounge] provides a function that cannot be adopted by ordinary carers because they don’t know what they are looking for [in terms of seizures]”. He considered that they are “not an unjustifiable intrusion into her privacy” and also that the “retention of data is useful” – since clinicians can inspect the videos to better understand the signs of seizures and possibly diagnose what triggers them.
Third, there is no comprehensive overarching care plan. The night staff are managed by one company, daytime care by another, plus the parents provide about 85 hours a week between them (“a crippling level of care, more than a working week each”, said the judge) – and their care is provided without a care plan that exists in writing. It’s also not clear who is in charge of her medication. “That’s bad, isn’t it”, the judge remarked. Later he added “What concerns me is that we’re two years into this case and we’re still asking what the care plan is. That is remarkable. It’s my first hearing, but two judges before me were none the wiser”.
Fourth, the care hasn’t been working out well. There have been tensions that “came to a head after an incident when one of the night staff was videoed asleep”. Both of the night waking staff were (or are?) on final written warnings for sleeping when supporting P as waking night staff. The parents (who were legally represented in court) want to move to a new model of care with directly employed staff. This would have the benefit of better governance (with the case manager responsible for all the people providing care), would enable better contingency planning (e.g., for staff sickness), and would also be cheaper.
Do P’s residence and care arrangements amount to a deprivation of liberty post-AGNI?
It was the Official Solicitor who, relatively late in the morning, pursued the question of whether or not P is deprived of her liberty.
OS: What we’ve not addressed is AGNI. The Official Solicitor’s submission[2] is that P is not now deprived of her liberty.
Judge: Is that on the basis that she’s implicitly consenting, using this new definition of consent, or is it on the basis of the unattractive proposition that she doesn’t have any liberty to be deprived of?
OS: The latter.
Judge: So, it’s that she’s so disabled that she doesn’t have any liberty to be deprived of, despite 24-hour supervision and control, including cameras, and she’s not free to leave, because she can’t unless she’s helped. Can I just ask you this. In a case of this sort where we have a profoundly disabled young woman who has to have this intensity of restrictions for her care, and where there are uncertainties about her future care plan (including because of financial issues), is this not a case where, whether it’s Article 5 or Article 8, there needs to be at least one review.
OS: That encapsulates our concerns. She would have had a Rule 1.2 representative. The issue the Official Solicitor is concerned about in this very particular situation is that P will not have any active involvement from the local authority, other than the Care Act review. Which is no criticism of them, but the local authority is very clear that their responsibilities are annual Care Act review and safeguarding issues.
After the lunch break, the court returned to the matter of deprivation of liberty. The judge referred to the “fact-sensitive multi-factorial test” that is now required and said he was “provisionally of the view that she does not consent – because she is incapable and cannot be said in any meaningful way to agree to her circumstances”. He continued: “The more difficult point is that she is in her home – a proper home, with her family. Now I must consider a comparator case, which Munby said was [‘obnoxious’/ ‘innocuous’][3] – but it can’t be [a deprivation of liberty?] because the Supreme Court [I take this to mean in AGNI] said that P must be compared to other people similar to her, and everyone with a similar level of disability to her will be cared for in a position like hers. And there’s an even worse argument – that because she’s incapable of liberty, she’s not deprived of it. I find that deeply philosophically difficult. It fails to look at liberty in its broadest sense. The State has obligations to ensure that people are enabled to have the best life they can”.
In the view of HHJ Burrows, the AGNI definition means that P in this case is NOT deprived of her liberty – a conclusion he didn’t seem happy to have arrived at. He quickly moved on to consider Article 8. “Privacy is hugely interfered with – it is necessary and proportionate, and nobody is suggesting there shouldn’t be 2:1 care or that cameras at night shouldn’t be used, but it does engage Article 8”. The judge referred to Baker J’s observations in Cheshire West at first instance – “even if it weren’t an Article 5 issue, he would be requiring review under Article 8 to ensure P’s best interests”.[4]
Counsel for P’s parents agreed that their daughter was not deprived of her liberty – but put the reasons differently. According to them, “P is cared for, not confined. Everything about her circumstances is tailored specifically to what she needs in that moment. And it’s not experienced as confinement”. They also believe that P “… is able to indicate happiness with her circumstances… she is able to vocalise happiness … she is happy in the situation that she’s cared in, albeit that the care is very intensive”. This sounds to me as though they were articulating, in effect, the AGNI notion of ‘valid consent’ (although the OS had previously indicated that the basis of the claim was not valid consent but lack of liberty to be deprived of – see the exchange between the judge and the OS above).
The hearing concluded with what I think was a expectation (I haven’t seen the order) that residence and care arrangements, which don’t amount to ‘deprivation of liberty’, would continue pretty much as they are for the time being, while the care manager draws up an overarching care plan which will (hopefully) be irrelevant in a couple of months or so once the company providing the day care is replaced with directly paid staff. If the parties can agree the care plan, no further hearing will be needed – at least not until the anticipated ‘review’ (which I think the judge will have ordered).
I have not yet received the approved order and will amend this post if it turns out there is more to report or if I have got something wrong – which is quite possible given the non-disclosure of documents relating to this case.
Reflections
It was apparent that HHJ Burrows is unhappy with the AGNI judgment – which seems to have divided the judiciary and the bar as much as it has divided opinion on the ground. Nonetheless, as judges must, he has applied it to this case and determined that P is not deprived of her liberty given the new criteria. I was disappointed that this hearing didn’t seem to involve a particularly rigorous application of the ‘multi-factorial’ analysis required by AGNI – which is of course what I hope to see in order to understand better how case law from the Supreme Court is applied in practice. For example, the judge didn’t engage with the parents’ argument that P was giving ‘valid consent’ by virtue of displaying ‘happiness’ with her arrangements. He didn’t return to and defend or revise his earlier ‘provisional’ view that “that she does not consent – because she is incapable and cannot be said in any meaningful way to agree to her circumstances”. There was clearly a difference of opinion on ‘valid consent’ here – but perhaps, being pragmatic, it didn’t matter, since the judge had already decided she was not deprived of her liberty on other grounds.
Finally, I see from the COP User Group minutes (1st July 2026) that HHJ Hilder has suggested the following ‘template’ (subject to amendment as considered appropriate for any individual case) in relation to AGNI directions. This goes to the heart of the issue that members of the public are legitimately concerned about in relation to how judges determine whether or not a person is deprived of their liberty – but as it’s reported via a witness statement, it won’t be at all straightforward for court observers to get disclosure.
I am left with the strong view that the legitimate public concern about how deprivation of liberty decisions are being made in the post-AGNI Court of Protection requires more transparency from the court.
Celia Kitzinger is co-director of the Open Justice Court of Protection Project. She is on LinkedIn (here), and also on X (@KitzingerCelia) and Bluesky (@kitzingercelia.bsky.social)
[1]For reasons I have yet to discover (but suspect was the result of administrative error), this case was never publicly listed on CourtServe (or anywhere else on line). The judge said at the beginning of the hearing that it had been publicised via a paper copy of the listing displayed on a board in the court building in Preston. Since I was not in Preston and the listing was not more widely publicised, I did not know that the hearing was in person and I’m grateful to the judge for admitting me via video-link under these circumstances.
[2]The Official Solicitor’s position will have been set out in full in her Position Statement, but this was not disclosed to me. Consequently, I do not know the legal arguments on the basis of which the OS advanced her position in the kind of detail and with the appropriate case law that would have been useful to me, and to readers, in understanding how the judge arrived at his decision. It’s unfortunate that the Court of Appeal decision in Gardner has impacted so negatively on understanding how judges make decisions in the Court of Protection about key matters of public concern.
[3]I initially heard (and wrote down) the word ‘obnoxious’ – it struck me quite forcibly at the time. But when I tried to track down Munby’s use of the word in connection with ‘deprivation of liberty’, I couldn’t find anything (although he did use the word ‘obnoxious’ in relation to the values of some religious groups, see his keynote address in 2013 on “Law, Morality and Religion in the Family Courts”). I resorted to Chat GPT which produced an extraordinary hallucinated account of what Munby could have said about obnoxious comparisons between people with disabilities – but there’s no evidence that in fact he said any of it! I think either the judge misspoke, or (quite likely) I misheard him (there was no camera on the judge so I was deprived of the resource of ‘hearing’ supplemented by lip-reading). I am almost certain that what the judge said (or meant to say) and what I should properly have heard was not ‘obnoxious’ but ‘innocuous’ – which is a word that Munby does use in the Court of Appeal judgment (Cheshire West & Cheshire Council v P[2011] EWCA Civ 1257) – no fewer than FIVE times. The judge in the case I’m blogging about here, Simon Burrows, acted as junior counsel for the respondent, the Official Solicitor, in that Court of Appeal case back in 2011, so it might well have stuck in his memory. However, Munby’s point in using the word ‘innocuous’ was nothing to do with comparators, but rather that “a good motive or intention cannot render innocuous what would otherwise be a deprivation of liberty” (§76) – which isn’t the point I understood HHJ Burrows to be making at this stage of the hearing. Munby did make observations about appropriate comparatorsbut without using either the word “innocuous” or the word “obnoxious”: he found that the protected party in the case under appeal was not deprived of his liberty, essentially because P was “living a life which is as normal as it can be for someone in his situation”. Given P’s disabilities, it wasn’t appropriate to compare him with a healthy non-disabled adult. The appropriate contrast to draw is with “the kind of lives that people like [P] would normally expect to lead” (§97). The restrictions and limits on his life were “the inevitable corollary of his various disabilities” (§110), and “there was nothing to show the life he is living at Z House is significantly different from the kind of life that anyone with his concatenation of difficulties could normally expect to lead….” (§110). So, something has got jumbled here. (I am open to correction!). Many thanks to everyone who responded to my social media and WhatsApp posts trying to figure out what was going on here.
[4] I have checked the judgment to which the judge seems to be referring here (Cheshire West & Cheshire Council v P& M [2011] EWHC 1330 (Fam)) and have not been able to locate this – but possibly it was said in course of the hearings (the judge in this present case, Simon Burrows, having acted back then as counsel instructed by the Official Solicitor). I am happy to be corrected if anyone can locate the source of this claim. This is the first instance Cheshire West case, before Baker J, finding that P was deprived of his liberty. It was subsequently appealed in the Court of Appeal (Cheshire West & Cheshire Council v P[2011] EWCA Civ 1257) where Lord Justice Munby finds that P was not deprived of his liberty, based on comparisons with other people with similar disabilities. Of course, this case then (joined with MIG and MEG) went to the Supreme Court which determined by a majority that all three protected parties were indeed deprived of their liberty – and it’s that Supreme Court decision in Cheshire West[2014] UKSC 19 that was overturned (albeit not definitively in the case of the particular individual P in Cheshire West) in the AGNI judgment.
This is the first time, post-AGNI, where I’ve seen new Deprivation of Liberty Safeguards authorised by the court[1] – and it surprised me, as P is a patient in hospital who needs urgent treatment for his brain injury.
The Trust made an application for a declaration that it would be lawful to administer the standard recommended clinical treatment for P’s condition: there was no dispute about either his diagnosis or the appropriate medical treatment – except from P himself.
He’s resisting treatment because his brain injury causes him to be unable to understand he needs treatment (he thinks there’s nothing wrong with him). He refuses permission to insert cannulas and removes them after insertion. To treat him successfully, doctors will need to sedate him. The Trust applied for court authorisation of general anaesthetic for five days (for treatment usually given on ward) and sedation as necessary subsequently, both effectively as restraint to enable treatment.
The Judge authorised treatment (unsurprisingly) – and also authorised DOLS.
The hearing
The case (COP 20035691) was heard by Ms Powell KC on 22nd June 2026.
It was the first hearing in a case concerning a man in his forties who’s been unwell for around 5 months with a deteriorating mental state and psychotic symptoms. He was originally detained for two months under the Mental Health Act 1983, but was subsequently discovered (following MRI brain imaging, lumbar puncture and EEG) not to have a primary psychiatric disorder but instead to be suffering from autoimmune encephalitis – a serious but often treatable condition in which the body’s immune system mistakenly attacks the brain, causing inflammation (“encephalitis”). By the end of April, his detention under the Mental Health Act 1983 was rescinded on the basis that his condition was organic rather than psychiatric.
There is evidence to override the presumption of capacity in relation to medical treatment, notably from a consultant psychiatrist, and from the neurology team. P “demonstrates severe cognitive impairment, requires one-to-one supervision, engages in occasional episodes of aggression, is tangential in his speech and is developing language dysfunction – he has a poor insight into his illness, insists he’s completely well, and is not aware he’s in hospital”. When the Official Solicitor’s agent visited him, his answers to questions about his medical condition and the proposed treatment were “confused” and “unintelligible”.
The Treatment Plan proposed as being in his best interests is pretty standard for autoimmune encephalitis: 5 sessions of therapeutic plasma exchange, testicular examination and imaging, and brainimaging; 5 days of Intravenous Immunoglobulin plus oral steroids if clinically appropriate; and peri- and post-operative care and treatment as necessary. The only unusual feature of the treatment is the need to deliver it with restraint and under general anaesthesia or sedation – the only way it can be delivered given that he’s resisting treatment. There is consensus that this is in his best interests – from the clinicians, the Official Solicitor and an Independent Mental Capacity Advocate (IMCA) who has visited him (no family members or friends have been involved and the judge said she knew very little about his pre-illness life). Even with treatment, “he is not going to go back to being cognitively unimpaired – but without the treatment the future is terrible, and avoidably terrible” (Counsel for the OS). As the judge put it, “it is likely, given the length of illness he has already suffered, that there is a degree of irreversible brain damage”.
The Trust (Barts Health NHS Trust, represented by Parishil Patel KC instructed by Hill Dickinson LLP) was seeking: (i) a declaration that P lacks capacity to conduct these proceedings and to consent to medical treatment; and (ii) an order that P should be treated in accordance with the Treatment Plan – to include restraint and/or sedation as required to deliver the Plan safely.
A draft order had been agreed between the Trust and the Official Solicitor (represented by Katie Gollop KC), effectively to make that declaration and order – and that’s the order the judge ended up making in the course of a short oral judgment at the end of the hearing.
The judge also authorised Deprivation of Liberty Safeguards. In light of the recent Supreme Court decision in AGNI, I hoped to understand the judge’s decision-making process in authorising a hospital DOLS – but it was over in a flash with no explication.
The judge reported the submissions made (in written form) by the applicant Trust: “In the Trust view, the circumstances under which he will be restrained and sedated amount to a deprivation of liberty under Art 5, using a multi-factorial approach. These methods are coercive as it is likely that he will not remain in hospital without them. His compliance will be secured through sedation.” She went on: “I agree with those submissions and authorise the DOLS as necessary and proportionate“.
On what legal basis did the judge decide to authorise DOLS?
Given the uncertainty and confusion that’s followed the AGNI judgment, many of us are looking to court judgments for careful articulation of the legal basis for deciding whether or not the living arrangements of particular Ps, considered in a multi-factorial way, meet the criteria for ‘deprivation of liberty’. There is, as Lucy Series has said, “widespread confusion and disagreement on the ground, already, about how to apply this test. There are so many potential elements that may or may not be relevant, and little clarity about how they work in combination with each other” (“Elephants, mosaics and hammers“).
In this case, the relevant elements of P’s situation that the judge said mean that P’s living arrangements meet the criteria for ‘deprivation of liberty are that he’s “restrained and sedated” (she could have added, if I heard right, that he’s also under one-to-one care) and he would “not remain in hospital” if he weren’t compelled to. But what that this tells me is that P meets the criteria for “deprivation of liberty” under the Cheshire West definition, because he is subject to ‘continuous supervision and control’ and ‘not free to leave’. The judge didn’t provide any reasoning as to how this P is deprived of his liberty under the AGNI interpretation. Simply referring in passing to a “multi-factorial approach” without spelling out any of the multiple factors purportedly considered in making a DOL assessment really doesn’t illuminate how she arrived at her decision. At the very least, I expected a reference to P’s active objections to treatment: that must be relevant to (if not determinative of) the decision that he’s deprived of his liberty (§187 AGNI)
I’m not disputing that the man at the centre of this case is deprived of his liberty, or that the judge made the correct decision. My gut reaction is that he is deprived of liberty and that also seemed to be the undisputed view of all professionals and the judge in this hearing. I expect that’s why it wasn’t really argued orally in court. I imagine the relevant arguments had already been provided in the written documents before the judge.
How would one apply AGNI to this case? After the hearing, I posted my own summary of the case and some questions about it on various group discussion forums with MCA professionals about how to apply the AGNI multi-factorial approach. Not surprisingly, I received contradictory and speculative responses from a range of people (including COP lawyers). One common response was simply “because he’s objecting to treatment” (drawing on §187 and §151 AGNI, although these paragraphs weren’t cited orally in court by counsel or by the judge). Then there’s the FG case (a court-ordered caesarean) as precedent for claiming that Article 5 is engaged if P is being sedated to stop them leaving to avoid treatment: AGNI did not suggest that this was wrong. But there’s this: “In ordinary circumstances, an individual in hospital to receive treatment (and who, for their own protection, would be prevented from leaving while, say, confused and unable to think because of medication) would not be regarded as suffering a deprivation of liberty within the meaning of article 5.” (§145, AGNI). This P’s circumstances, it was suggested, are not “ordinary” – because he’s objecting. There was some discussion of the order in which the “objective” (not free to leave etc) and “subjective” (he’s objecting) elements should be assessed – and if it’s “iterative” so that the subjective is part of the objective, how exactly that should be done in this case? Some suggested that this P meets the requirements for being deprived of his liberty because the restrictions go beyond what other patients with the same illness receiving the same treatment would need (because their treatment would be ward-based, without general anaesthesia and sedation). Others speculated that perhaps it was simply that the court was more focused on the (urgent) best interests issue and just played it safe on the DOL issue without detailed arguments (which seems to me to be absolutely true!).
In seeking to understand how the DOL decision was made in this case, I did not have the benefit of Position Statements. In compliance with the Court of Appeal decision in Gardner, I was sent a “Case Summary” instead – a detailed (5-page) document covering helpful information about P, the parties, and the application, as well as a “chronology of factual background” (essentially a list of medical events extracted from the consultant neurologist’s witness statement). But the “Case Summary” does not cover any legal arguments made by the parties – and it barely mention ‘deprivation of liberty’ (it just provides, in the chronology, a date on which a DOLS was sought). I strongly suspect that the relevant legal arguments, with case law and citations from paragraphs of AGNI, are in the Position Statements, and that they underpinned and were relied on by the judge in making her decision. But without the Position Statements, and without substantive oral argument, observers can’t know why or how a decision is made. In the end, despite having watched the hearing and heard the oral judgment, I don’t know the legal basis on which this judge made the decision she did about deprivation of liberty – which pretty much defeats the purpose of observing the hearing in the first place.
Facts about P can be sensitive, and that was given as a reason in Gardner (in the Court of Appeal) for withholding Position Statements from observers. But position statements are supposed to be legal arguments and they should be the least sensitive of the legal documents. The ironic result in this case is that I now have information about P’s testicles conveyed in a “Case Summary” but know virtually nothing about the legal basis for decision-making concerning them. And the one thing I most wanted to understand in the wake of AGNI – on what legal basis did this judge decide that P is deprived of his liberty – was entirely opaque to me.
Celia Kitzinger is co-director of the Open Justice Court of Protection Project. She is on LinkedIn (here), and also on X (@KitzingerCelia) and Bluesky (@kitzingercelia.bsky.social)
[1]For a helpful resource on the AGNI judgment see https://www.39essex.com/wp-content/uploads/2026/06/2026-UKSC-16-Summary-for-website.pdf. What I’ve seen frequently, since the AGNI judgment was handed down, is (a) a decision to delay until a future hearing judicial determination as to whether or not residence and care constitutes a deprivation of liberty; and (b) ending of proceedings because they are newly recognised as having been “improperly constituted” as DOLS or s.21A under the now superseded CheshireWest definition.
Editorial Note: This is the third ‘commentary’ blog post we have published in the wake of the Supreme Court decision, handed down in June 2026, changing more than a decade of law and practice on ‘deprivation of liberty’ (see Endnote for more information).
For people who consider their loved ones well cared for, safe, and happy, the pre‑AGNI deprivation of liberty (DoL) processes were nonsensical and often intrusive. For that reason, the current judgment brings a sense of relief to many. But for other individuals, whose daily lives are dictated and constrained by institutional or quasi‑institutional regimes, with simple choices removed from their decisional space, and an array of human‑rights abuses hidden behind closed cultures, this judgment may have a more detrimental impact.
While some individuals in these circumstances may not be fully aware of the restrictions imposed on their liberty (or may have grown to accept the narrowed decision spaces they inhabit), many advocates and activists acutely recognise the implications of the judgment and strongly convey a sense of agony.
The positives and negatives of AGNI.
In many situations, DoLS and judicial authorisations have mopped up the mess created by an under‑resourced health and social care system that has had to firefight and prioritise significant need over promoting human rights.
Article 5 safeguards have effectively compensated for a lack of appropriate or accessible mechanisms to address what are often Article 8 abuses.
There certainly should be accessible safeguards outside DoL processes, and perhaps this judgment will open the door to broader awareness and embedding of human rights and Mental Capacity Act (MCA) principles. I hope it does, and many proactive colleagues are pushing this agenda.
Although the judgment landed as a bombshell, there have been concerted efforts to make practical sense of it, and there are positive aspects to narrowing the objective definition of DoL.
Rather than the broader ‘bright line’ threshold provided by the acid test, the objective element is realigned with the Guzzardimultifactorial test, which interrogates the degree, intensity, and effects of the restrictions. This encourages a more nuanced assessment of the cumulative impact of the arrangements, in which any coercive approaches are crucial considerations.
Similarly, the greater emphasis on determining wishes and feelings is very much welcomed. Of course, all practitioners should centralise wishes and feelings regardless of this judgment, but it serves as a strong reminder for those who are less conscientious.
Overall, the revised criteria for establishing what constitutes a deprivation of liberty will mean that significantly fewer people will be subject to DoL assessments or authorisation frameworks. This will enable more targeted support for individuals in the most critical need of Article 5 safeguards.
Nevertheless, individuals who struggle to express their concerns, who have no one to speak up on their behalf, or who remain silenced by systems that pathologise their distressed or withdrawn behaviour, will remain invisible[i]. In particular, this will affect people who are privately funded and who may not be reviewed under any other statutory process[ii].
Furthermore, there is a real risk of inconsistency and confusion about what this judgment means. Formal guidance will go some way to alleviate uncertainty, but how well that guidance cascades into care settings and day‑to‑day practice is another question.
The main problems I foresee stemming from AGNI are threefold.
One: the risk that valid consent under Article 5 is conflated with consent more generally, thereby diminishing the understanding that informed consent and the processes set out in the MCA 2005 are fundamental to the delivery of care and treatment.
Two: the risk that compliance and acquiescence are regarded as the accepted standard for valid consent under Article 5, or that such compliance, which may be an ingrained pattern of behaviour, is misconstrued as a positive expression of wishes and feelings. This prompts considerable ethical and philosophical debate, which requires far fuller exploration than I have space for here.
Three: that the purpose and relative normality of the arrangements are now treated as relevant to whether a person is deprived of their liberty, which could be interpreted in a way that minimises the extent and effects of the concrete situation.
In terms of purpose, it would be highly concerning if any health or social care providers were to use restrictive interventions as punishment, rather than solely to keep the individual safe. In practice, the purpose is always likely to be protective; it is therefore unclear what this distinction adds.
As for relative normality, this term functions as an empty signifier, in that the judgment does not define what relative normality means. It is therefore left to subjective interpretation, which may drift into a regressive disablist approach, whereby what is classed as ‘normal’ for a disabled person is positioned differently from that for a non‑disabled person, moving us away from a universal concept of liberty.
45. [.] axiomatic that people with disabilities, both mental and physical, have the same human rights as the rest of the human race. It may be that those rights have sometimes to be limited or restricted because of their disabilities, but the starting point should be the same as that for everyone else. This flows inexorably from the universal character of human rights, founded on the inherent dignity of all human beings, and is confirmed in the United Nations Convention on the Rights of Persons with Disabilities. Far from disability entitling the state to deny such people human rights: rather it places upon the state (and upon others) the duty to make reasonable accommodation to cater for the special needs of those with disabilities.
That said, I am optimistic that AGNI will be applied in a non‑disablist manner, with an initial focus on whether the circumstances meet the threshold for confinement under the multifactorial approach (which, arguably, will capture a minority of those previously caught, given the narrowing of the objective definition). Where an individual lacks capacity (under the MCA) to decide on arrangements that amount to their confinement, this should be followed by a holistic evaluation of whether valid consent can be derived from the person’s basic understanding of their situation, and their wishes and feelings over time. I hope this will foster more meaningful, relational engagement with the person and their loved ones during DoL assessments.
Above all, I hope that any financial savings arising from the reduced applicability of the DoL safeguards are reinvested into person‑centred, accessible, rights‑based services. I would urge that wider advocacy mechanisms be made available to safeguard Article 8 rights, beyond time‑limited, issue‑specific advocacy roles such as IMCAs and Care Act advocacy. Article 8 safeguards should be offered to all individuals who remain in restrictive care outside the scope of the AGNI – DoL threshold, including those in privately funded arrangements.
In summary, AGNI may prompt a much‑needed re‑evaluation of MCA practice; however, for this to be effective, it must be accompanied by an inter‑agency and cross‑sector commitment to meaningful investment in human rights, advocacy, and person‑centred care. Without that, the judgment risks creating more problems than it resolves.
Eleanor Tallon is an Independent Social Worker, Expert Witness, and BestInterests Assessor. Eleanor is also an ESRC-funded Doctoral Training Pathway (DTP) student at the University of Birmingham. Her research focuses on the application of the Mental Capacity Act 2005 in private brain injury case management. Eleanor can be contacted via email eleanor@mcaprofessional.co.uk or through her website mcaprofessional.co.uk and found on LinkedIn or X(Twitter) @Eleanor_Tallon
[i] HL v UK provides a compelling example of how individuals who struggle to express their concerns can become effectively invisible. HL was treated as having consented to admission because he did not attempt to leave; this was interpreted as compliance. His distressed behaviours, including agitation and self-harm, were medicalised and used to justify continued hospitalisation.
[ii] Although all adults with eligible needs have a right to an assessment under the Care Act 2014, in practice this may not be realised for “self-funders”. This may occur because individuals or their relatives are unaware of their entitlement to a Care Act assessment, they are given inconsistent information or experience extensive delays due to the prioritisation of other cases. As a result, many self-funders remain outside statutory systems (Henwood et al., 2022).
Endnote (by Daniel Clark)
Back in 2014, In Cheshire West, the Supreme Court considered the meaning of a deprivation of liberty (DoL) through reference to Article 5 of the European Convention on Human Rights. Lady Hale, giving the majority but not unanimous judgment of the Court, presented an ‘acid test’ for deprivation of liberty: is a person under continuous supervision and control, and not free to leave?
On Tuesday 2 June 2026, the Supreme Court handed down judgment in what is increasingly being referred to as “AGNI’ (the case was brought by the Attorney General of Northern Ireland). The Supreme Court overturned Cheshire West, finding the acid test to be wrong in law, and directed a different approach.
First, the identification of the objective element of a deprivation of liberty must entail a multifactorial analysis, which includes consideration of the intensity and purpose of confinement. If these conditions are not satisfied, there is no deprivation of liberty.
Second, a person may lack capacity to make decisions about their care and residence but can nevertheless give valid consent through an expression of their (positive) wishes and feelings. If a person is giving such consent, they are not deprived of their liberty.
To access the judgment, see: Judgment (PDF) (hyperlinked)
To access the court’s approved press summary, see: Press Summary (PDF) (hyperlinked)
If you would like to contribute a commentary about this judgment, please contact openjustice@yahoo.com, and mark your email for the attention of Daniel Clark.
The judge has made a declaration that P died at 16.41 on 26th June 2026. Our condolences to his family.
UPDATE from 2nd July 2026
The case was heard this afternoon by Garrido J. The Trust has now made an application for a declaration of death. Since the last hearing, the “apnea” test has been done (twice) by two independent experts who conclude that P is dead according to neurological criteria. Some family members dispute that P is dead: they report having seen him trying to breathe. The ‘red triangle light’ on the ventilator goes on from time to time which family take as evidence of attempts at breathing, but according to medical professionals (including the nurses who’ve witnessed it), that light goes on if there is air movement caused by P being moved, or by his reflex movements, or even by condensation building up in the ventilator which alters the air pressure. The hearing will continue at 11am tomorrow (via MS Teams): this was a late decision so it may well not appear in the public lists. It is possible that P’s partner will give evidence about what she’s seen (P trying to breathe). It’s possible the family will pursue an application for another independent expert to examine P. There will be “closing submissions” from the Trust (Parishil Patel), the family representative (Arianna Kelly) and the Official Solicitor (Nageena Khalique) and a judgment.
*****
The key question in this case, which will be back in court on 2nd July 2026, is whether or not a man in his 40s, who had an out-of-hospital cardiac arrest on 24th May 2026 (so about a month ago) is now “brain stem dead”.
What is brain stem death?
Brain stem death is the irreversible loss of all functions of the brain stem – the part of the brain that controls breathing, swallowing and other reflexes (e.g. pupil response to light, gagging, response to pain). In many countries, including England and Wales, this is considered to be “death” in law, even if the heart continues to beat, with the assistance of a ventilator. Some legislatures (but not England and Wales) allow a religious exemption to the neurological criteria for death, and there are a few controversial cases of ‘brain dead’ people being maintained for years (e.g. famously, Jadi McGrath[1]). These cases underscore the importance of correctly testing for brain death and also the ethical concerns that arise in these cases.
A neurological definition of death has been accepted and endorsed by the courts from at least 1992 onwards (Airedale NHS v Bland [1993] AC 789). “In medicine, the cessation of breathing or of heartbeat is no longer death. By the use of a ventilator, lungs which in the unaided course of nature would have stopped breathing can be made to breathe, thereby sustaining the heartbeat. Those, like Anthony Bland, who would previously have died through inability to swallow food can be kept alive by artificial feeding. This has led the medical profession to redefine death in terms of brain stem death, i.e., the death of that part of the brain without which the body cannot function at all without assistance. In some cases, it is now apparently possible, with the use of the ventilator, to sustain a beating heart even though the brain stem, and therefore in medical terms the patient, is dead; “the ventilated corpse”.” (Lord Browne-Wilkinson in Bland).
Clinical guidance about “brain stem death” is provided in the Code of Practice for the Diagnosis and Confirmation of Death by the Academy of Medical Royal Colleges in 2008. It says: “Death entails the irreversible loss of those essential characteristics which are necessary to the existence of a living human person and, thus, the definition of death should be regarded as the irreversible loss of the capacity for consciousness, combined with irreversible loss of the capacity to breathe.”
There’s an NHS page about brain death and its diagnosis here. If someone is brain dead, the damage is irreversible and, according to UK law, the person has died:”It can be confusing to be told someone has brain death, because their life support machine will keep their heart beating and their chest will still rise and fall with every breath from the ventilator.“
The question before the court: Declaring death vs considering best interests
Almost all applications to discontinue mechanical ventilation or clinically assisted nutrition and hydration are decided on the basis of ‘best interests’.
But when a person is already dead (on the basis of neurological criteria), so that the effect of the medical treatment is not to keep the person alive but simply to maintain a beating heart in an otherwise “dead” body, ‘best interests’ decision-making does not apply. All the court can do is make a declaration of death.
In an earlier blog, we reported on a case seeking a declaration of death (Withdrawing treatment after brain-stem death: A case in the Family Division). In that case all the proper tests had been done to make a declaration of death, and the Official Solicitor declined to act (because P must be alive to have “best interests”).
This is the approach also used in previous court cases in the Family Division: “If a patient is brain stem dead, then there are no best interests to consider. Once those criteria are met the patient has irreversibly lost whatever one might define as life…[…] Once a court is satisfied on the balance of probabilities that, on the proper application of the 2008 Code (and where appropriate the 2015 Guidance), there has been brain stem death there is no basis for a best interests analysis, nor is one appropriate. The court is not saying that it is in the best interests for the child to die but, rather that the child is already dead. The appropriate declaration is that the patient died at a particular time and on a particular date without more.”Sir Andrew McFarlane §96 Re M (Declaration of Death of Child)[2020] EWCA Civ 164,
Directions hearing
This was a very short (35 minute) directions hearing before Mr Justice Garrido, sitting in the RCJ on 24th June 2026.
There was no substantive opening summary, and although I asked in the usual way, I was not sent position statements, or any of the three documents recommended for disclosure to COP observers in Gardner (i.e. a case summary or chronology or statement of ‘issues before the court’). This report is as accurate as I can make it in their absence.
Counsel for the applicant Trust (University Hospital Southampton NHS Foundation Trust), Parishil Patel KC, explained that it is the view of the treating doctors that the man at the centre of this case has “suffered catastrophic and irreversible brain injury with permanent loss of brain stem function” – meaning that they believe he meets the criteria for ‘brain stem death’. I gathered that this is accepted by some family members and not by others: they are “split into two camps”. Counsel for the patient (Nageena Khalique KC) instructed by the Official Solicitor reported that “a lot of the information has been discussed and debated albeit not accepted by the family”.
However, one of the tests required by law for determination of brain stem death – the apnea test – has apparently not been performed at the level needed. Counsel for the Trust said that, for that reason, the applicant Trust is not currently seeking declaration of death, but rather, in light of P’s condition and poor prognosis, is applying for a declaration that it is lawful and in P’s best interests to withdraw life-sustaining treatment. This might, however, change.
Test for brain stem death – and why has it not been done
The judge said that he understood the reason for the apnea test not being done was an inability to do it to the relevant standard “because the patient is being ventilated”. Parishil Patel, for the NHS Trust, said that when the relevant tests were being conducted that was the situation, though it might not be the “position forever”.
A second opinion doctor is being engaged to repeat the relevant ‘brain stem’ tests and may perform the outstanding apnea test. The court was informed that two doctors must be present to carry out the tests.
Judge: Everybody realises there are any number of demands on doctors which may result in delay, but, anyway, your Trust is doing the best it can to obtain a second opinion doctor.
Counsel for the Trust: Yes, and everyone recognises the urgency. If in fact [P] is brain stem dead, the quicker we get on to that moment the better, if only because, if he is brain stem dead, we are providing treatment to someone who is dead.
Judge: What does [treating doctor] say about the realistic chance of performing the relevant test?
Counsel for the Trust: Two things – he DOES think the test can be performed and that’s why he is asking the second opinion doctor to do it. There are also ancillary tests upon which the court can rely. There’s a reasonable degree of confidence that the second opinion doctors may well be able to (pause)
Judge: …. opine on the issue of brain stem death.
Counsel for the Trust: The case would then be a different sort of case …. to withdrawal of life-sustaining treatment. […] Is this a declaration of death case or is this a continuation of the case that is currently in the application which is withdrawal of life-sustaining treatment?
What next?
The judge was clearly concerned that some family members might dispute a diagnosis of death, even after expert evidence was obtained. “Any suggestion that additional evidence ON TOP OF the second opinion doctors – that needs to be cauterized at the earliest opportunity. Any additional application for expert evidence would need an application in advance.” [judge’s emphases]
Counsel for the Official Solicitor hoped that “at the next directions hearing we will have some more useful information from the second opinion doctors. That will be pivotal in shaping the case.” She went on “Until we see that evidence, the OS position is cautious, because it may be that further questions need to be asked or different expertise is required. […] I am grateful that an application for further evidence CAN be made within the timescale that’s proposed.”
The judge was hopeful, asking whether it was “realistic, Ms Khalique, to expect any questions of the second opinion doctors to be raised and answered in advance of the hearing on Thursday next week.” She replied that there may be “some questions that become obvious [and it] might precipitate the instruction of an expert“.
The current position of at least some family members means, however, that there is likely to be a contested hearing, with at least one family member opposing the application (whether it’s for treatment withdrawal in P’s best interests or for a declaration of death resulting in treatment withdrawal). Chloe Moran, a solicitor from Irwin Mitchell representing P’s brother, told the court that her client opposes the Trust’s application and wishes to be joined as a party.
The next hearing is scheduled for the afternoon of Thursday 2nd July 2026.
Claire Martin is a Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a member of the core team of the Open Justice Court of Protection Project and has published dozens of blog posts for the Project about hearings she’s observed (e.g. here and here). She is on X as @DocCMartin, on LinkedIn and on BlueSky as @doccmartin.bsky.social
[1] Jahi McMath was 13 years old when she suffered a massive haemorrhage following a tonsillectomy on 9th December 2013, in Oakland Children’s Hospital in California. Three days later she was diagnosed as ‘brain dead’ (confirmed by two staff physicians and three independent specialists). Her mother, who did not believe her daughter to be dead since her daughter was breathing (with a ventilator), her heart was beating, and her body was warm, made an application to court for appointment of a “neutral” neurologist to assess the patient’s medical status – that expert confirmed Jahi was brain dead, and the judge had no alternative but to authorise withdrawal of medical treatment. A death certificate was issued, listing her date of death as December 12, 2013. (see “Brain death,”“dead,” and parental denial: the case of Jahi McMath). The family fought a protracted battle to keep her on mechanical ventilation until she “died” (again) in 2018 (see https://edition.cnn.com/2018/06/29/health/jahi-mcmath-brain-dead-teen-death). There’s a thoughtful discussion of the implications of “brain death” here: https://aeon.co/essays/why-medics-and-the-law-clash-with-family-in-brain-death-cases
Editorial Note: This is the second ‘commentary’ blog post we have published in the wake of the Supreme Court decision, handed down in June 2026, changing more than a decade of law and practice on ‘deprivation of liberty’ (see Endnote for more information).
In overruling Cheshire West, the Supreme Court concluded that its “acid test” alone was not sufficient to establish a deprivation of liberty. There are arguments that the safeguards had become too broad and too burdensome for an already overwhelmed system. But my family’s experience sits uneasily with that account. For us, this did not feel like a system overwhelmed by safeguards. It felt like one that was under-resourced, adversarial, and unwilling to make those safeguards accessible when they were most needed.
In 2014, in Cheshire West, the Supreme Court held that a person was deprived of their liberty if they were under continuous supervision and control and not free to leave. Those protections should have been in full working order by the time my Grandma needed them in 2018, but when it came to that point not only were they not put into place for her, we weren’t even told they existed.
Born in 1930, my Grandma was funny, cheeky, loving and firmly opinionated. She had been diagnosed with end-stage heart failure and vascular dementia, with fluctuating capacity and had been living happily in a small nursing home funded by Continuing Healthcare. The nature of her dementia meant she was able to make some decisions independently and needed support with others, but she never lost the ability to express her wishes.
In 2018, I was due to get married. A week before the wedding, the manager of the nursing home told me to prepare myself as my Grandma was “hanging on” for my wedding and would die shortly afterwards. Just four days after the wedding, I received a call from the same manager informing me that, as “I was no doubt aware”, my Grandma had not died, and so needed to move out of the home.
We were told that my Grandma had met with several managers from the local CCG and agreed to move to a particular care home that we knew instantly she would never have agreed to. It was a place she called “the death house”, where her best friend had died two weeks after moving in following complications triggered by dehydration. My Grandma blamed the home for her death and would shake her fists and blow raspberries at it whenever we drove past.
My parents, who held lasting powers of attorney, had not been told about the meeting. They were told this was because my Grandma had now been assessed as having “full capacity” and so did not need anyone present. There were no minutes or meeting notes recording what was discussed, how the move had been explained, how her capacity had been assessed, or whether she had been asked if she wanted a family member present. My Grandma, for her part, had no memory of either the assessment or the meeting.
When we explained the proposed move to her, she told us in unmistakable, and quite fruity, terms that she would not go to “the death house”. By chance, later that week, I was visiting when two managers from the CCG unexpectedly arrived to get my Grandma to sign paperwork. This was another meeting we had not been told about. I was asked to leave but my Grandma grabbed my hand and said she wanted me to stay. During the meeting, it was clear that my Grandma did not understand what was being explained and notably she no longer recognised the name of the home. When I showed her a picture and explained it was where her friend had moved to she immediately told the managers that if they wanted her to go to the “death house”, they should “kill her now to save some time”.
Despite this, the move went ahead on the basis that she had already consented and had full capacity.
I cannot detail every horror that followed, but some are impossible to ignore: the lack of a bed, or any medication and oxygen for her on arrival on moving day, the constant broken equipment, the daily missed medication, the lack of staff, the reused linen covered in the discharge from another resident’s bed sores, the use of restraint to stop her attempts to leave, being left hungry, soiled and distressed and the threats that we would never see her again if we kept raising concerns. Nor will I ever forget the moment she clutched my hand in visible fear at the end of visiting and told me: “You don’t know what it’s like here at night.”
Each day brought a new crisis but when we raised concerns and showed videos of my Grandma saying she did not want to be there and explaining how badly she was being treated, we were told that she lacked capacity and so this could not be taken seriously.
During this same period, my mother was in intensive care after cancer surgery, and I was leaving work twice a day to go to the home and check that my Grandma had been fed, had oxygen and had been given her medication and taken to the toilet. Despite constant contact with the NHS, the local authority and the care provider, nobody told us about deprivation of liberty safeguards, best interests decisions or the Court of Protection. I was too overwhelmed and sleep-deprived and too consumed by the immediate task of keeping her safe to research beyond the advice given by those same bodies.
After a final dramatic escape attempt, which we only learned about later through a subject access request, the home evicted her. My bedbound Grandma had somehow managed to get over the bedrails (in use without risk assessment or consent to stop her leaving), crawl out of her room and across the corridor, and climb down the stairs towards the main doors before staff found her. It was only then that we heard about deprivation of liberty safeguards, when they were cited by the home in the eviction decision following my Grandma’s repeated escape attempts and her repeated statements that she did not want to live there.
She was thankfully then moved to a wonderful home, where she lived for another year before dying peacefully surrounded by her family. It later turned out that everything that happened was entirely avoidable, as this other home could have taken her sooner, having had a room available when she was forced into “the death house”.
I still carry an immense amount of guilt that I did not get her out sooner, and I have to stop myself from thinking too long about what else may have happened that we did not know about. But I also know that families cannot use rights they do not know exist, especially when they are exhausted, frightened, and firefighting one crisis after another.
Like many people, I was brought up to trust that public institutions will protect us when we are at our most vulnerable. Even when I could not understand the motivations of decision-makers in my Grandma’s case, and even when I witnessed first-hand the severe neglect and appalling conditions she and other residents were experiencing, I still believed that someone, somewhere, would do something to help. I believed it could not be possible for people to be effectively imprisoned in such appalling conditions, against their will. Discovering that my belief and that trust was misplaced felt like a betrayal so deep it is still difficult to look at directly.
This is what troubles me about the current debate. We are told Cheshire West overwhelmed the system. Yet my family never experienced an excess of scrutiny. We experienced decisions made without us, safeguards we knew nothing about and could not access, and a system that placed excessive responsibility on us to keep my Grandma safe while in care but then threatened us when we advocated for her wishes and wellbeing.
If safeguards are not visible, understandable and enforceable for all people who need them, then they are failing. But that is not an argument for fewer safeguards. It is an argument for better ones. The overwhelm in the system is real, but it is multi-faceted. It reflects long-term underfunding across the NHS, social care and the legal system, which has left families to fill the gaps in health and social care alone while being expected to navigate complex legal processes without professional guidance.
Poor accountability, inaccessible processes and defensive decision-making compound that underfunding, turning safeguards that should protect people into systems families struggle to find, understand or use. Too many people are living and dying in conditions that should shame this country.
My Grandma’s experience does not persuade me that we need weaker protections. It taught me that robust safeguards are essential, and that they must exist in practice, not just on paper, for everyone who needs them. If doing so overwhelms the system, then the system is not fit for purpose and an urgent and far more radical rethink is needed.
Elissa Novak is an unpaid carer to her son and studies Law part-time with the Open University through its Carers’ Scholarship Programme.
Endnote (by Daniel Clark)
Back in 2014, In Cheshire West, the Supreme Court considered the meaning of a deprivation of liberty (DoL) through reference to Article 5 of the European Convention on Human Rights. Lady Hale, giving the majority but not unanimous judgment of the Court, presented an ‘acid test’ for deprivation of liberty: is a person under continuous supervision and control, and not free to leave?
On Tuesday 2 June 2026, the Supreme Court handed down judgment in what is increasingly being referred to as “AGNI’ (the case was brought by the Attorney General of Northern Ireland). The Supreme Court overturned Cheshire West, finding the acid test to be wrong in law, and directed a different approach.
First, the identification of the objective element of a deprivation of liberty must entail a multifactorial analysis, which includes consideration of the intensity and purpose of confinement. If these conditions are not satisfied, there is no deprivation of liberty.
Second, a person may lack capacity to make decisions about their care and residence but can nevertheless give valid consent through an expression of their (positive) wishes and feelings. If a person is giving such consent, they are not deprived of their liberty.
To access the judgment, see: Judgment (PDF) (hyperlinked)
To access the court’s approved press summary, see: Press Summary (PDF) (hyperlinked)
If you would like to contribute a commentary about this judgment, please contact openjustice@yahoo.com, and mark your email for the attention of Daniel Clark.
The Trust brought an application to the Court of Protection for a declaration that it was lawful and in P’s best interests not to detain her under the Mental Health Act and not to impose feeding upon her.
As emphasised throughout the hearing, this is a case of “unanimity”: P’s mother, the Official Solicitor, P’s treatment team—and, now, an independent medical expert (whose report was not available at the time the application was made)—are all in agreement that it is not in P’s best interests to treat her under compulsion.
In light of this independent medical opinion, the Trust (represented by James Berry KC) no longer believes it requires declaratory relief from the Court of Protection. Their submission today (initially before the court on Friday 19th June 2026 in advance of what was otherwise to have been a two-day substantive hearing about declarative relief on 22nd and 23rd June 2026) was to withdraw their former application pursuant to CoP rule 13.2. That was not opposed by the other parties (P represented through her litigation friend the Official Solicitor by Katie Scott and P’s mother, represented by Victoria Butler-Cole KC).
The importance of this case is that, in response to the Trust’s application to withdraw, the OS invited the Court to give a full reasoned judgment, addressing:
(1) The circumstances in which a Trust should make an application to the Court where it proposes not to detain a patient under the MHA 1983, and not to provide potentially life-saving treatment to the patient (e.g. by way of NG feeding under restraint); and
(2) Which Court has jurisdiction to determine such an application (it being the position of the OS that, to the extent that the Trust requires any relief on the facts of this case, that relief should be granted by the High Court in the exercise of its inherent jurisdiction.[1]
Counsel for the Trust said they were “agnostic” on the first issue. Regarding the second issue, the Trust’s position was that no such guidance should be given because “there are plenty of authorities that say the court should not be used as a general advice centre, and this is a contentious issue on which there is no clear authority”. The Trust also submitted that if the Court of Protection were to tackle such an issue it should do so in a case where there is a contested substantive issue. These submissions were successful. Mrs Justice Theis accepted that the jurisdiction question was ill-suited to the facts of this case, because the application had been issued (and was being withdrawn) without dispute from any party. I found myself wondering if this was persuasive: why would it be more appropriate to deal with the jurisdiction question in a case where there is disagreement, given that it is fundamentally a question of legal principle? Nevertheless, it became clear early in the hearing that this issue would not be tackled in this case.
The first issue led to a much longer discussion. Mrs Justice Theis was keen to “steady the ship” by creating a list of factors to be considered when deciding whether to issue an application for declaratory relief in these circumstances. That list is likely to include:
Whether an independent, external second medical opinion has been obtained
Whether there is any dispute (a) as to P’s capacity, and (b) as to the treatment plan, between the treating team, the treating team and the expert second opinion, and between them and P or those with an interest in P’s welfare (including an IMCA if there is no-one else, s.37 MCA)
The impact on P of bringing these kinds of applications (it was reported that P was very upset on learning of these proceedings)
The relevance of the framework used for withdrawal applications relating to patients in prolonged disorders of consciousness
What other steps can be taken to, for example, shorten proceedings
Some of these factors are quite vague, but will no doubt be refined in the published judgment.
The point, concerning “the impact on P of bringing these kinds of applications” was expanded upon by Ms Katie Scott, for the OS, in a manner tailored specifically to the experiences of patients with anorexia nervosa. She listed three ‘impacts’ to be considered. First, the fact that court proceedings are inherently stressful for Ps. Second, the need to avoid confusing P when applications are “legally complex and difficult to understand” and are often procedurally complex as well. Third, the need for clarity as to the scope of the application: what the court is being asked to do and what the powers of the court actually are. Ms Scott drove home the point that this is particularly important for patients with anorexia nervosa, who are, in her words “invariably intelligent, extremely engaged in their treatment and decisions being made about them…have been in the system for decades, [and are] very familiar with the powers of the MHA”.
Ms Scott demonstrated great respect for patients with anorexia nervosa with these submissions. The need for control is a core feature of anorexia, and proceedings in the Court of Protection are often both legally and procedurally confusing in a way that epitomises lack of control. It is to be hoped that Ms Scott’s insights are reflected in the list of factors that results from these proceedings.
The Trust was granted permission to withdraw its application, Although Mrs Justice Theis did not go as far as she might have in response to the OS’s submissions, she did indicate that she would take this opportunity to consider how, in her published judgment, she could support decision-making about court applications in this contentious and complex area of law.
I await with great anticipation the published judgment, which will no doubt serve as a useful tool for clinicians, legal practitioners, patients with anorexia nervosa, and those with an interest in their welfare.
[1]I was not granted access to the skeleton arguments (or any other documents) relating to this hearing. I am grateful to Celia Kitzinger, who was granted access to, and received, written versions of the legal arguments from the Trust and the Official Solicitor via an order from Judd J at an earlier hearing: she drew on them to help me to elucidate the issues as presented by counsel orally in this hearing.