By Claire Martin, 6th February 2026
The protected party, a man in his 40s with Down Syndrome and learning disabilities, has lived with his father all of his life, and he and his father want that to continue.
The problem is that in 2024, he was diagnosed with Stage 5 kidney disease – which means he needs kidney dialysis to keep him alive, and it needs to be done regularly and for long enough on each occasion to be effective.
The court has been presented with evidence that – contrary to court orders (now with a penal notice) – his father is not taking him for the required treatment. He’s thereby putting his life at risk. This is a very sad, and very long-running, case (COP 20000635) which we’ve blogged about before, following hearings in October 2024 (“An urgent case: Renal failure and an application for forced ‘extraction and conveyance’ to hospital” and “A protracted hospital stay: A next hearing in the ‘renal failure’ case”). The case was closed in November 2024 with a final court order allowing P to be discharged home on condition that his father would take him for out-patient dialysis three times a week for the full amount of time recommended by the Trust clinicians. Proceedings concluded at that point, without a published judgment.
But the case was back in court a year later (blogged here: “Renal Failure Case Returns: Dialysis problems and Barnet’s non-compliance with a court order”). P’s medical condition was said to be worsening due to his father’s non-compliance with the court order:
“The Trust says that, over the past year P has increasingly been missing his dialysis sessions at hospital. In June 2025, P was admitted to hospital for dialysis for three days, following some missed sessions. Since then (up to mid-September 2025) the Trust says that P has missed 11 out of 40 dialysis sessions and has not stayed for the full 4 hours on more than half of the sessions, and that they could not persuade P’s father to allow P to stay for the full treatment period. Further concerns have been raised by the Trust that P is not taking his medication as prescribed or eating the right diet (resulting in high phosphate levels). The position of the Trust (represented by Victoria Butler-Cole KC) is: “P is at risk of very serious complications as a result of under-dialysis including sudden death from an electrolyte abnormality, fluid accumulation leading to difficulty breathing and pressure on the heart, chronic damage of blood vessels, and the development of calciphylaxis, a painful and sometimes fatal ulcerating skin condition.” This application also asks the court to ‘fully investigate’ the option of removing P from his father’s care. He has lived with his father all his life, so this would be a draconian step for the court to authorise.” [Quoted from blog]
The Approved Order from that hearing (8th October 2025) states that the Local Authority (London Borough of Barnet) had been: ‘… directed to file a report by a psychologist by 7 February 2025 which was not complied with, and no application was made to vary or discharge that order before the proceedings stood dismissed on 20 February 2025’. That hearing was focused on the non-compliance of the Local Authority and the need for a psychologist’s report to enable the court to consider P’s best interests for residence and care, to ensure that his life is not at risk from lack of renal care.
There have been 3 hearings since then – all before Mr Justice McKendrick . In the next two sections, I’ll describe: (1) what happened in the two December hearings (on 4th December 2025 and the ‘final’ hearing on 17th-18th December 2025); and then (2) the 14th January 2026 ‘review’ hearing.
1. December 2025 hearings
At the hearing on 4th December 2025, Mr Justice McKendrick ordered that, in readiness for the ’final’ hearing (17th-18th December 2025), witness statements must be filed by the NHS Trust and by the Local Authority (Barnet) and he outlined the issues he wanted them to address.
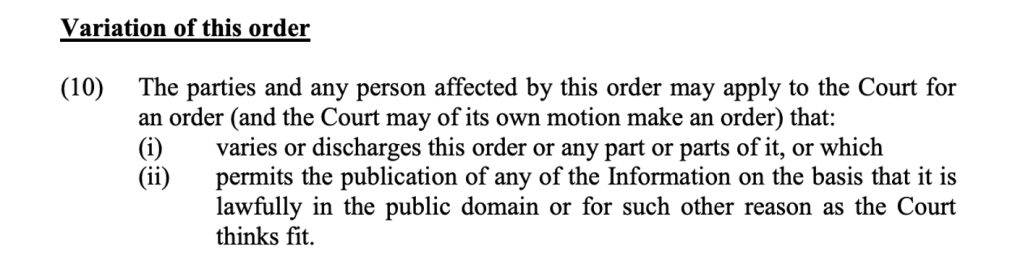
The judge wanted to hear from the Trust regarding “DM’s [the protected party’s] clinical presentation, his prognosis and life expectancy if he remains in the care of [his father] or if he moves to supported living and in particular if he a) receives dialysis in accordance with the current plan, b) continues to receive dialysis in line with the partial compliance of the last year, or c) if he refuses dialysis altogether, and d) whether dialysis could or should be enforced in the event that DM does not comply with it and e) in the event DM were to require compulsory detention under the Mental Health Act 1983 whether he would be able to have enforced dialysis at that time if needed, any other considerations relevant to DM’s best interests as regards his care and residence”.
The judge wanted information from the Local Authority (Barnet) regarding “a. The concrete option for DM’s care and residence that it has identified. b. The proposed care plan for DM at that placement including staffing levels, arrangements for DM to be taken to hospital for dialysis and activities; details of DM’s living environment; the psychology support that would be available for the placement to support staff; and a proposed plan for contact between DM and MM c. The plan for transferring DM to the placement. d. Its analysis of DM’s best interests as regards his care and residence and contact with [his father]. e. Such further correspondence from [the psychologist] as may be available.” [Quotes from the Approved Order dated 4th December 2025[i]]
At the hearing on 17th-18th December 2025 (of which I was only able to observe part of the day on 18th December) P’s treating renal consultant and his previous social worker both gave evidence in person. P’s father was able to put questions to them both.
The evidence squarely indicated that P was not receiving his dialysis as required and that this was a result of P’s father’s lack of compliance with the court order.
P’s father’s questioning of the professionals and responses to questions put to him made me think that he was scared for his son yet, possibly, did not understand the magnitude of the risk to P’s life caused by his own actions. Debra Powell KC (counsel for P’s litigation friend, the Official Solicitor) cut through the stalemate by establishing P’s father’s view of what his son would want for himself:
Counsel for OS: He’s supposed to go three times a week, but you don’t take him.
Father: Sometimes he doesn’t want to go.
Counsel for OS: Why do you take him?
Father: Because I have no choice
Counsel for OS: Why do you have no choice?
Father: Because of infection. [P’s father started to talk about a second opinion doctor]
Counsel for OS: I don’t want to talk about a second opinion. When you take him to hospital, he stays for 3-4 hrs and has dialysis.
Father: Yes
Counsel for OS: Do you think that does him any good?
Father: If I don’t take him, he might get infection.
Counsel for OS: Do you think the only thing is to stop an infection?
Father: No [it’s] for his blood.
Counsel for OS: So yes, you accept the dialysis cleans his blood because his kidneys can’t do it?
Father: I didn’t know it before.
Counsel for OS: Let’s focus on now, not before. You accept that dialysis cleans his blood?
Father: Yes the doctors say …. I am not talking about dialysis.
Counsel for OS: I am talking about dialysis and I am the one asking the questions. You accept that the dialysis cleans his blood. Do you accept we all need to have our blood cleaned – for most of us our kidneys do it for us. [P’s] kidneys don’t work anymore. Do you accept that?
Father: Yes, if you say. That’s why I am taking to hospital.
Counsel for OS: It’s not just me, it’s six consultants.
Father: Can I have their names?
Counsel for OS: I am sure they can be provided. [Renal consultant] has explained that if P doesn’t have his blood cleaned three times a week, he is going to die.
Father: Yes, they say that.
Counsel for OS: Do you accept that?
Father: Yes …
Counsel for OS: Do you think [P] would … he wouldn’t want to die? Would he rather die than have dialysis three times a week?
Father: [missed – I think he said that P doesn’t always want to go]
Counsel for OS: You let him not go. I am not asking whether [P] understands that. [P] likes his life, doesn’t he? He likes football, playing snooker ….
Father: Yes [P] … the dialysis you are saying … is there any time he’s fallen ill?
Counsel for OS: You are not asking the questions. Do you think he hates dialysis so much he would rather die than go to dialysis? Please, really listen to the question [repeated question]
Father: No he not hate no…. he get used to it now.
Counsel for OS: Do you think [P] would want to live?
Father: Yes.
The style of questioning seems quite harsh, written in black and white. The tone of Debra Powell’s questioning wasn’t harsh though. It was firm and focused, but not harsh. P’s father did understand the questions it seemed to me – and I think he would have preferred a different focus, which is why he turned the answers back to his own concerns (wanting a second opinion doctor, or the fact that P sometimes doesn’t want to go for dialysis). I thought that Debra Powell skilfully and fairly ensured that P’s father focused on and answered the questions that she wanted to put to him – focusing on what P would most want for himself. Nevertheless, I can imagine it might have been a difficult experience for P’s father, since he is very sceptical (as are many people) about health professionals and social workers.
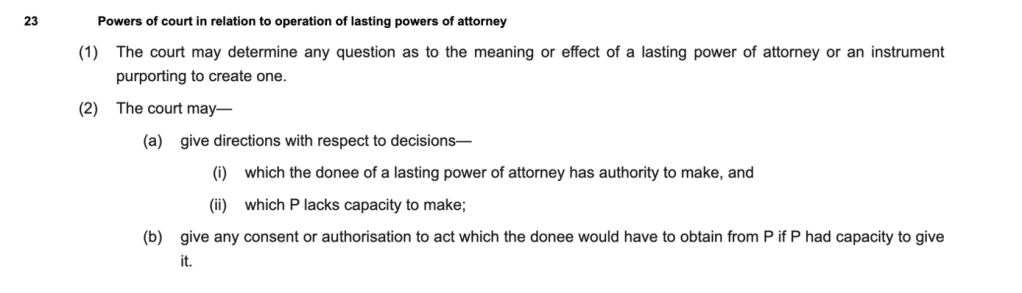
Mr Justice McKendrick authorised the removal of P and authorised his residence in a supported living placement in his best interests. There’s a published judgment: Royal Free NHS Foundation Trust v EF & Ors [2025] EWCOP 52 (T3) (19 December 2025).
The judgment states (initials in this judgment are NN for P’s father and EF for P, see endnote for further explanation of changes to initials):
- NN was told clearly that supported living may be required, as recorded in Recital C of the November 2024 order. It recorded: “NN has been informed by the court that if he does not support and facilitate EF to attend his dialysis treatment sessions and take his prescribed medications, the court will have to give serious consideration to authorising a transfer of EF to a supported living placement as proposed by the local authority.”
- The court has provided time and latitude to NN because it is recognised that there are likely to be emotional, psychological and possible even psychiatric consequences for EF of his separation from NN. He will live apart for the first time in his life. He will miss the daily contact with his father. He will miss the familiar environment of his home. He will be supported by strangers who are paid to be with him. He will be in an unfamiliar home around two miles from NN’s home. He will be required to adapt and understand a new home and routine and unfamiliar people. All this will be difficult for him. I factor into the best interests the risks of harm to his mental health. I readily accept Dr T’s evidence summarised above. I accept the concerns of Mr Q the social worker.
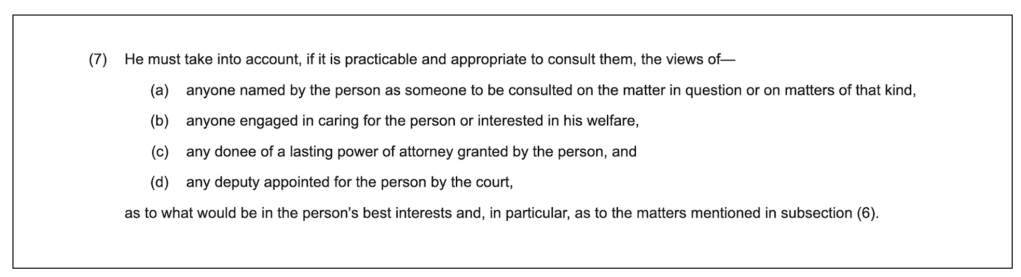
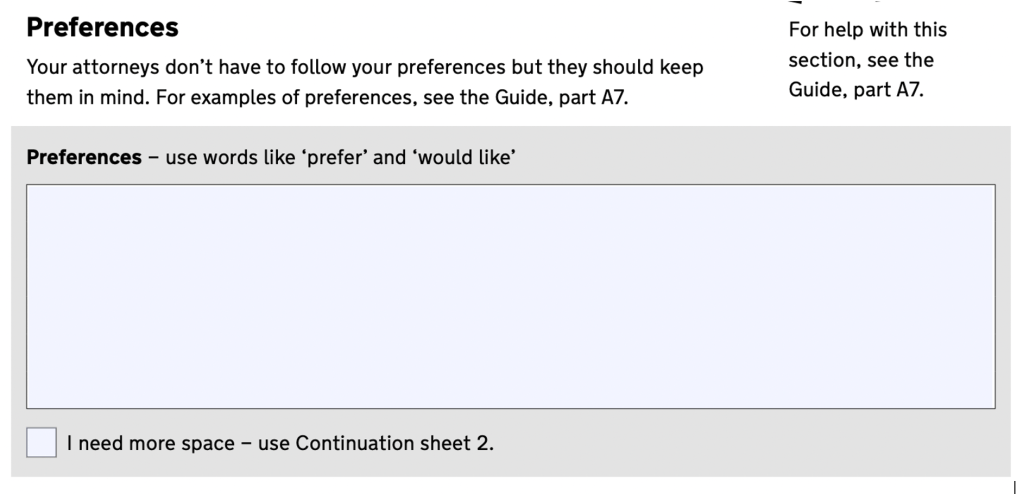
- Ms Powell questioned NN on the issue of EF’s wishes and feelings. He told her that EF would rather properly attend dialysis than die. I accept that evidence. I consider EF enjoys much of his life, his sports and his social time. His wishes and feelings are to live. His wish conflicts with his wish to live at home and with NN. I have weighed these matters up carefully. His past and present wishes, feelings beliefs and values are all important. His desire for life must be considered holistically with his other wishes and feelings. But ultimately this is a case where reducing the risks of EF’s early death carry very great weight in the balancing exercise.
- I have factored in EF’s Article 2 ECHR right to life and EF and NN’s Article 8 ECHR rights to respect for family life. As case law makes clear these rights have been factored into the section 4, MCA best interests analysis. Any interference with NN’s Article 8 ECHR right to respect for his family life with his adult son are fulsomely justified as being proportionate, necessary and in accordance with the law to keep EF alive and accordingly there is no violation of NN’s Article 8 ECHR rights.
- The represented parties have spent much time drafting a transition plan, a contact plan and a conveyance plan. The Official Solicitor supports all three plans. The transition takes place gradually between now and 6 January 2026, when EF will move to his new supported living placement. I raised the risk of NN undermining the move over the weeks ahead. The represented parties accepted that risk but considered there were lesser risks to the gradual transition than that attached to the immediate move. Dr T supports the plan. The contact plan provides for EF to settle into his new home and for contact with NN to take place on a regular basis. There are some reasonable limitations on the contact. These are necessary and in EF’s best interests to assist him to build relations with his new staff and for him to settle. I also accept the conveyance plan but I do not authorise, as the parties agreed I should, the involvement of the police on the ‘second’ attempt to convey EF from his current to his new home. This would be frightening for him. It may then create an association for him between the police and his new home and it would be the worst possible start for this new chapter in his life.
- I will also authorise the deprivation of EF’s liberty at his new placement. This is necessary and in his best interests to keep him safe.
- The plan is fraught with risk. Ms Powell candidly acknowledges it may not work. But she is clear on EF’s behalf that the efforts must be made to provide him with the opportunity to secure for him a longer and better quality of life.
- The third respondent submitted I should attach penal notices to the order and make an all ports alert. I declined to make these additional orders as they are not currently necessary. There is no proper evidence NN and EF are flight risks.
- I have listed the matter for a half day review hearing on 14 January 2026.
2. January 2026 hearing
I was expecting P to have been living at his new home for a few weeks by the date of this hearing, and for the review to be about how that was going. But the move hadn’t happened – due to resistance from P’s father. Attempts made on 6th and 8th January were unsuccessful. The Local Authority and the Official Solicitor both now sought an immediate move for P (currently at the hospital for dialysis) into his new residence, with subsequent restrictions on contact with his father.
Submissions for the Local Authority (Catherine Rowlands)
My Lord, the situation is that that on the last occasion you made an order that [P] should move. [There has been] progress but also obstacles. Progress is that the placement itself is set up. It could receive him at the drop of a hat. They have got things ready, like toiletries and […] if a move in short order [is necessary]. [P] has asked questions about it and has at times shown interest in moving. He has one carer [E] who will move with him, giving reassurance. Carers are getting to know him, familiarising themselves with him and vice versa.
This morning [P] has been taken to dialysis. I am not sure if he had the full session. He indicated that he would like to come to court but it was decided that by the time he got here, it could be all over, so it’s better to go to McDonald’s. He hasn’t been having full sessions. His potassium levels are significantly raised. Nobody in court other than [P’s father] is of the view that [P] should not move.
Last time I asked for a penal order to be attached and I repeat that today. [There is] a potential way forward today. Because [P] was with carers at dialysis – he could be taken to his new placement with them after dialysis. He would not be going straight from dialysis, which the Trust has expressed concerns about. There would be a move from the hospital to a positive environment such as McDonald’s, then on to the placement. We would like you to authorise that deprivation of liberty today.
We ask that you approve taking him there [to the placement] with [agency] transport. There will be people there to show him around, people he knows, to settle him in.
We request an order for [P’s father] not to go there for three days, to allow [P] to settle and for them both to come to terms with what has happened.
This is set out in the Local Authority witness statement. We are in contact with the carers at the moment and have advised them to await instructions.
Submissions for P via the Official Solicitor (Debra Powell KC)
Unfortunately, since December, matters have continued in the same way. [In relation to dialysis sessions] – eight attendances have been shortened and three have been missed entirely. [P’s] potassium on the 3rd January was 6. When it’s above 6 it’s dangerous, and when it’s 6.5 it needs admission. [P’s] life, I am afraid, is in the balance if this continues. Sadly …. [P’s father] simply doesn’t believe or grasp that if things continue, the chances of [P] surviving are [reducing?]. I am going to repeat it in open court – the way that disordered potassium works is that as potassium rises, it leads to a risk of the patient having a sudden, unpredictable heart attack and dying. And that could well be the consequence of [P] not having regular dialysis for the prescribed amount of time.
His father needs to understand that, and if he won’t or can’t understand that, his influence over [P] needs to be reduced so that [P] has a chance of receiving his dialysis that he needs. There is no reason for optimism.
The court has made clear orders which [P] and his father are thwarting. This can’t be allowed to continue. It is not a matter of choice. [P’s] father makes it clear to court today that he considers it a matter of choice. It’s not. There are no good options available. As is apparent from the Local Authority evidence, when proper professional efforts are made to secure the transition plans, his father has thwarted those by behaving in an unfortunate manner – shouting, saying ‘my son will leave here over my dead body’, saying that the authorities are trying to harm his son, all of which must have the most terrible impact on [P]. It must be immensely distressing to be exposed to this language from a man who he loves and trusts. Unfortunately, in my submission, the least worst option is that [P] is taken from McDonald’s today, straight to [name of] placement. It will be necessary for him not to receive visits from his father for a period of time. It’s not clear from the Local Authority Position Statement whether they submit [his father] should not see [P] on Friday at dialysis. It says not to attend the placement for 72 hours. [We would] welcome from counsel for the Local Authority whether that should apply to dialysis on Friday.
Sadly, the OS position is that it seems vanishingly unlikely that [P’s father] will comply with it [the court order] and if we wait until tomorrow when [P] is at home, it’s likely to be unsuccessful. Then Friday is dialysis day.
What will have changed by next Tuesday? [P’s father] is not going to comply with the injunction. The Local Authority will have to apply to have him committed for contempt, and this is what nobody wants to see.
Judgment
The judge gave an ex tempore (oral) judgment authorising the immediate move of P to the new placement (via MacDonalds):
I anticipated that there would be difficulties in moving [P] to the placement, which is why I listed the hearing today. It was really my hope that [P’s father] would have really listened and understood from December that the sensible route to take would be to take [P] for dialysis for every session for the full period of time. If he had done that, the nature of today’s hearing would be very different.
Today he is clearly of the view that the kidney problems are related to the actions of a social worker or a nurse. His continues to believe … [it is] patently false and based on his own false beliefs. There is no possibility of him accepting the seriousness of [P’s] medical condition. He has been given every opportunity from November 2024 to today. In answer to my questions today, he tells me he has not even read my judgment from December [2025] which sets out why [P] should be moved.
[…]
There was an attempt at conveyance on the 6th January [2026], set out in the witness statement. Following this [P’s father] was resistant. [P’s father] is said to have dominated the conversation. [P] was physically and emotionally uncomfortable – [he was] scratching. [P’s father] used inflammatory language, he made allegations against professionals. [There was a] second attempt on the 8th January 2026. [P’s father] resisted. He allowed professionals to enter. He displayed visible rage, shouting “over his dead body’, [they] want to “kill” his son. [P] mirrored his father’s allegations. His father made historical allegations. He demanded professionals leave. He absolutely refused to comply with the court order.
[…]
The medical evidence is clear. [P] needs to attend ALL sessions for the full hours on ALL occasions.
[P’s father] has been given EVERY opportunity [Judge’s emphasis] to understand. He remains in denial of the necessity for [P’s] treatment. The treating team is extremely concerned. […] As Ms Powell summarised, higher potassium levels could lead to the early death of this delightful man at the early age of 44.
[…]
This is just to give effect to the order I made previously – it is convenient because it protects the best interests order to ensure he receives dialysis to keep him alive. There is no injustice to [P’s father]. He has had proper notice today. His position is wholly unrealistic. He advances a case that he loves his son, but prevents his son receiving the treatment he needs to prevent his death.
My judgment is that he is conveyed today after enjoying a meal at McDonald’s or somewhere else.”
I very much hope that P is doing okay, and that his father will be able to see that regular dialysis is improving the health of his son, so that they can see each other without this issue hanging over them in future, and can enjoy their time together going to football, playing snooker and having a nice time after what must have been a very traumatic period of time for them both.
Claire Martin is a Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a member of the core team of the Open Justice Court of Protection Project and has published dozens of blog posts for the Project about hearings she’s observed (e.g. here and here). She is on X as @DocCMartin, on BlueSky as @doccmartin.bsky.social, and on LinkedIn.
[i] Throughout the proceedings, the initials used for P in the public listings and in the (public) Approved Orders are DM for P and MM for his father. However, in the published judgment (also quoted here), the initials Mr Justice McKendrick uses are ‘NN’ for P’s father and ‘EF’ for P. For simplicity, I refer to the protected party as ‘P’ but as the reader will note, different initials are used in different extracts quoted in this blog.