
By James Walker, 11th June 2021
Other experts who have contributed to this Project’s discussion of the Court of Protection case of An Expectant Mother [2021] EWCOP 33 are not alone in the misunderstanding of the data surrounding home births. This is largely due to the fact that the presentation of the data is influenced by underlying beliefs of those presenting it. There are very few good trials into home birth and the cohort trials are from different parts of the world and not necessarily well controlled or detailed in their information. The meta-analyses are therefore flawed due to the mixture of the case cohorts included as well as coming from different clinical backgrounds.
It is often stated that home birth is safe for the low-risk woman. No birth is safe: safety is not binary, it is a continuum, and it changes over time. Risk is poorly assessed in most cases and is assessed as higher or lower depending on your starting point and your own beliefs. None of us is impartial.
When considering home birth, there are four things to consider:
- the underlying risk and the awareness that this may change
- the environment where the birth will take place
- the difficulties in transferring a woman to hospital if required
- the wishes of the mother.
Fundamentally, it is the mother’s decision after she has had fully informative information to help her decide. If a woman with the mental capacity to do so decides on a home birth, then irrespective of the hospital staff views or feelings, there is an obligation to support this and provide midwifery input.
I obviously cannot discuss the specifics of this case, in which I gave expert evidence, but it is fair to say that there were some concerns about obstetric risks to the baby but the emphasis of concerns was on the ability to transfer to hospital. This centred around the mother’s agoraphobia, and the effect it may have on her decision making.
The risks of an incident occurring for any individual birthing at home are not different from the risks of birthing in hospital, apart from the ability to monitor the mother and baby if there are concerns and the ability to transfer if required. So is not the home birth that is the problem, it is what you can do if something goes wrong. In many instances babies are lost or damaged during home birth due to slowness to observe deterioration, slowness to escalate and transfer to allow “rescue” to take place.
The best UK figures on home birth are published here and are used by the NHS website:
Perinatal and maternal outcomes by planned place of birth for healthy women with low risk pregnancies: the Birthplace in England national prospective cohort studyBMJ 2011; 343 doi: https://doi.org/10.1136/bmj.d7400 (Published 25 November 2011)
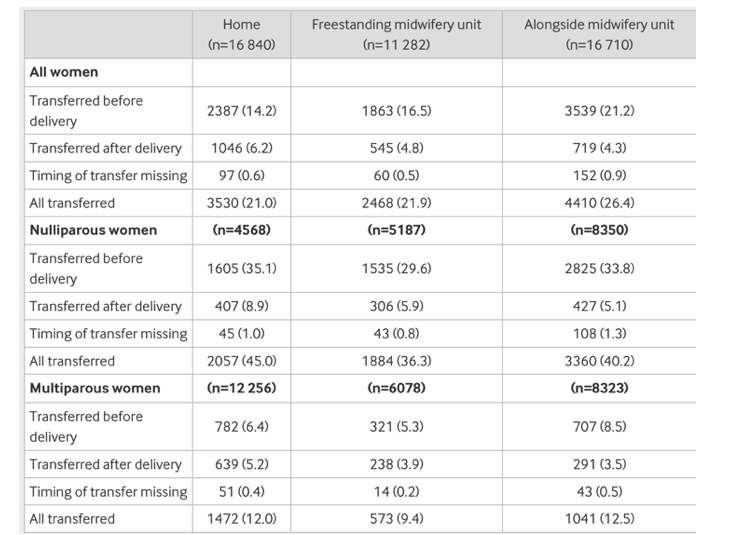
For transfers in labour or in the postnatal period, the study showed that 45% of primigravida are transferred: 35% before delivery and 8.9% after. For multiparous women the figures are 6.4% transferred before delivery and 5.2% after delivery. The figures were not much different for women giving birth in Freestanding Units or Alongside Midwifery Units, demonstrating the risk is not home birth per se but primigravida pregnancy. Many of the figures quoted by supporters of home birth do not differentiate between woman having their first baby at home and those having their second or more baby at home. That is why transfer figures are usually quoted as being a lot lower.
Half of the reasons for transfer was failure to progress (17.9 of the 35.1%), then fetal concerns (8.2 of the 35.1%), desired pain relief (2.8 of the 35.1%) and other concerns. After delivery, the reasons were requirement of suturing the perineum (4.4 of the 8.9%), haemorrhage or retained placenta (3 of the 8.9%), baby reasons (0.9 of the 8.9%) and other concerns.
Although emergency (urgent) ambulances were called in 11.5% of all primigravida, a “blue light ambulance” was probably needed in only 1% (my guestimate). The transfer times from decision to transfer to arrival in the obstetric unit was around 49 minutes on average.
The primary perinatal outcome was a composite of perinatal mortality and specific neonatal morbidities: stillbirth after the start of care in labour, early neonatal death, neonatal encephalopathy, meconium aspiration syndrome, brachial plexus injury, fractured humerus, and fractured clavicle. This composite measure was designed to capture outcomes that may be related to the quality of intrapartum care, including morbidities associated with intrapartum asphyxia and birth trauma.
The study showed that when correcting for pre-existing risk, primigravida had a 2.8 increased odds ratio of poor baby outcome (9.5/1000 or 1/100) compared with hospital birth 3.5/1000 or 1/300). This is largely due to the time taken to escalate the problem and transfer the mother. These figures are slightly worse than those quoted in court which were the unadjusted figures.

This is the basis of the figures I used in my evidence as they are the best that are available for the UK and would be relevant in this case.
To emphasise, the risks of home birth is not related to the incidents that occur but to the ability to transfer and rescue.
James Walker is Emeritus Professor in the Department of Obstetrics and Gynaecology at Leeds University and author of Planned home birth. Best Pract Res Clin Obstet Gynaecol, 2017.
Photo by Beth Macdonald on Unsplash

2 thoughts on “Evidence of risk of planned home birth”