
By Celia Kitzinger with Claire Martin, 6th September 2021
The case before Mr Justice Hayden (COP 13783897, 17th-19th August 2021) concerned “AH”, a woman in her fifties who is emerging into consciousness following brain injury caused by Covid 19.
The question the court had to decide was whether she should continue to receive ventilation.
She is currently in a minimally conscious state in Addenbrookes Hospital in Cambridge.
Everyone agrees that AH lacks the capacity to give or withhold consent for medical treatment. This means that the decision needs to be made for her.
The treating doctors and the family were not able to agree the best course of action, which is why the case was in court.
Mr Justice Hayden’s decision was that ventilation should be discontinued by the end of October 2021, but should be continued as long as necessary up to that date to allow the opportunity for this close and loving family to be together at the end.
The judgment was published on Friday 3rd September 2021 and has since been widely reported in the media[1].
Press reports seem to be based on a press release from PA Media (what used to be called the “Press Association”) by Brian Farmer, although other bylines are sometimes used instead or in addition. Some incorporate a short statement put out by the Communications Department at Cambridge University Hospitals NHS Foundation Trust. The stories I have seen are accurate, as far as they go, but they focus – perhaps inevitably – on the outcome (what the judge decided) rather than the process (i.e. how the judge went about considering the evidence and arriving at a decision).
This post focuses on the reasoning behind Mr Justice Hayden’s decision.
The decision-making process
If doctors consider a treatment to be wrong clinically – i.e. it will not ‘work’ – they cannot be compelled to give it: not by a patient, not by family, not by the court.
But the ventilator ‘works’ in the sense that it is keeping AH alive while she cannot breathe for herself.
The question, then, is whether continuing ventilation, which is keeping AH alive, is in AH’s best interests. If it is, ventilation should be continued. If it is not, it should be stopped. This is what the judge had to decide.
The starting point is always strongly in favour of prolonging life where possible (in accordance with Article 2 of the Human Rights Act). As Lady Black, giving the judgment of the court in An NHS Trust v Y [2018] UKSC, said, there must be “a full recognition of the value of human life, and of the respect in which it must be held. No life is to be relinquished easily” [92]. In law, however, the strong presumption that it is in a person’s best interests to stay alive is not an absolute principle, but “must yield to the principle of self-determination” (Bland at 864D).
Some people believe that if a treatment is keeping someone alive then it is always, by definition, in a patient’s best interests – because life is sacred, or because we should never ‘give up’ on life, however tenuous our hold on it, until death is inevitable. They may see stopping treatment as tantamount to suicide or euthanasia. They say they would want all possible treatments to the end.
Other people say that if they can only be kept alive “with machines and tubes”, they’d rather be “let go”. I’ve heard many stories from people who’ve witnessed “bad deaths” of loved ones who received invasive medical treatments up until they died, and that’s not what they want for themselves.
Doctors, family members – even the judge – may have strong views about what they would want if they were in the patient’s situation.
But what matters here is: what does AH want? What would she decide if she could? How best can the judge promote AH’s autonomy and self-determination?
The Mental Capacity Act 2005 (MCA) lays out what the person making the decision about best interests (in this case Mr Justice Hayden) must “consider” and “take into account”:
So the task before Mr Justice Hayden was to establish (as s.6 MCA specifies) what AH’s past and present wishes and feelings are, the beliefs and values that she would take into account if she could, and the other factors she would think relevant if she were able to decide for herself. This means considering questions like: What sort of person was AH? How do her character and personality and the way she chose to live her life – her commitment to her family and to her faith – shed light on the choice she would make now?
In considering these questions, the judge must consult the people listed in s.7 MCA. AH had not named anyone to be consulted, nor appointed anyone with Lasting Power of Attorney, so, for her, the people to be consulted were those “engaged in caring for [AH] or interested in [her] welfare”: the treating team in the hospital, and AH’s family.
In the final hearing, spread over three days (Celia was only able to observe the first day; Claire was only able to observe the second), the judge heard from the treating team and from the family to establish, as best he could, what AH would want for herself in this situation.
This was a challenging task.
Assessing AH’s best interests
The parties in court were:
- the applicant, Cambridge University Hospitals NHS Foundation Trust represented by Katie Gollop QC);
- the Official Solicitor for AH (represented by Nageena Khalique QC)
- and four members of AH’s family, as litigants in person: her two sons (A and K) and two daughters (S and M). (One of her sisters also gave evidence, but was not a party.)
The applicant Trust took the position that continuing ventilation was not in AH’s best interests. Some members of the family (especially A and M) took the position that ventilation should be continued. The Official Solicitor reserved her position at the start of the hearing, wanting to hear further evidence before expressing a view on behalf of AH.
At the time of the hearing AH had been treated in the intensive care unit at Addenbrooke’s for more than 230 days.
Evidence from the clinicians
Mr Justice Hayden heard evidence from three members of the treating team: a Consultant in Neuroscience and Trauma Intensive Care Medicine (Dr A); a Consultant Neurologist (Dr B); and the Matron in Adult Critical Care (Ms C).
The clinicians were in agreement that AW had suffered “devastating injuries” as a result of covid infection including:
- A necrotising myopathy that has killed and scarred muscle tissue, leaving her with profound muscle weakness.
- A motor neuropathy such that the nerve cells supplying muscles have died (similar to motor neuron disease): this has affected 90% of her nerve cells. There is no possibility of regeneration or recovery of function – she won’t be able ever to walk again, or to use her hands. Sensory nerve activity is preserved, so it is likely that she experiences pain (and can receive comfort from touch).
- A brainstem encephalopathy, which affects eye movement, facial movement, swallowing and the Reticular Activating System (RAS, the nerves that awaken the rest of the brain). There has been some partial recovery of the RAS, which is why AH is more aware and conscious now than she was a few months ago. According to one of the treating doctors: “As AH has become more awake and intermittently aware of her extreme disabilities she has predictably become more distressed. AH frequently cries and has a distressed countenance.” (Dr. A)
- Cerebral encephalopathy, which has caused damage to the cerebral cortex (which provides memory, speech, experience, planning and thought) and to the basal ganglia (meaning that the brainstem RAS ability to wake the cortex is impaired).
In the professional opinion of the doctors treating her:
“She will be almost totally paralysed for the rest of her life. It is likely that she will be dependent on mechanical ventilation via a tracheostomy. She will be unable to move, talk, wash herself, adjust her position if she is uncomfortable, get up in the morning, put herself to bed. Furthermore, she will develop the complications of immobility which will include pressure sores, recurrent pneumonia and other infections, and painful joint subluxations and contractures.” (Dr. B)
The court had also received written reports from two independent experts who had examined AH: Professor Derick Wade, a Consultant in Neurorehabilitation (instructed by the Trust) and Dr Chris Danbury, a Consultant Intensive Care Physician (instructed by the Official Solicitor) – although only Dr Danbury was in court to give oral evidence. The expert reports substantially endorsed the Trust’s diagnoses and prognosis. Dr Danbury stated that AH has a “less than 1% chance of long-term liberation from mechanical ventilation”.
The Trust position is that “those caring for AH have come to the unanimous view that of the limited options available to her, no longer receiving ventilatory treatment is her best way forward”.
This was also the professional opinion of both the independent experts. According to Dr Danbury, AH’s experience is “slanted towards pain and discomfort” and sooner or later she will “inevitably” develop an untreatable infection “which will be fatal”. He concluded in his report that “the current situation … revolves around slowing the inevitable process of her death rather than giving meaning to her life”.
The treating team has come to believe that AH is often in pain, and frequently feels “anguish” “fear” and “distress”. She often cries. They say there is nothing they can do to alleviate her suffering. It’s impossible to reverse her brain damage or the damage she has suffered to her peripheral nervous system.
Although, as the Matron said, “we all agree she takes comfort when her family are there and she’s calmer and more relaxed” (Ms C), this is a small part of her experience.
One of the treating doctors, Dr A, is “now deeply worried that her awareness has reached a point where all she is able to focus on is fear, anxiety, and hopelessness”. He concludes: ““I cannot reasonably believe that she would choose to live in this way, unless there was a clear signal from prior discussions with her family, or evidence of any previous statements she may have made or written”. They fear that the treatment they are giving amounts to “daily torture” and that it is “morally and ethically wrong” to continue treatment.
According to Dr A, AH’s situation is:
“… associated with a loss of dignity and a total loss of autonomy – she is unable to provide consent and cannot participate in any meaningful choice about how she is treated. This extends from decisions of the utmost gravity, such as withdrawal of treatment, to very modest choices like whether her head faces the window so that the sun warms her, or whether her head does not face that way because the light hurts her eyes.” (para 69 (iii)).
There is a great deal more detail in the judgment about the course of AH’s illness, and the nature of her brain damage. In court, the doctors were asked a lot of questions about details of diagnosis and prognosis, the detailed answers to which were sometimes quite difficult for a non-medic to follow. One daughter asked about whether AH’s nerves could regrow so that her arms and legs could work again (the answer was no). Another issue was whether she would ever be able to communicate beyond indicating “yes” and “no”. Clinicians agreed that it was highly unlikely that she would ever be able to speak again, because she is unable to exert sufficient control over her mouth and tongue, but pointed out that there are many technologies available that could offer the possibility of communicating in ways other than via speech – if only she were cognitively able to do so.
“She has more than enough motor control to establish a much more sophisticated communication system than just ‘yes’ or ‘no’. If you can move just a single muscle you can do that. What she doesn’t have is a long enough period of attention and a long enough period of capacity to get beyond ‘yes’ and ‘no’. The speech and language therapists have worked for hours to try to get her to spell out words… I don’t think she will ever get to that level of consciousness.”
One of the daughters pointed to the (generally accepted) fact that AH had become more conscious recently and asked if this didn’t suggest the possibility of further recovery. She pointed to the fact that Covid-19 is a very new illness and there’s lots that isn’t known about it. But AH no longer has COVID and the neurological damage she has (as a result of COVID) is very familiar to clinicians.
Dr B replied using an analogy borrowed from one of the expert reports before the court.
“She’s had an upward trajectory, but Professor Wade’s analogy was very helpful. If the floor is zero (completely unconscious) and the ceiling is 100, she was at 2 or 3 and now she’s at 5. This is really, really hard for a layperson to grasp. I fully agree there has been an improvement, but the significance of the improvement and the extent of the improvement are not agreed amongst us. The doctors see it in a particular way from our experience of brain injury. There is no sign of Covid in AH now. This is the consequence of brain injury. We are drawing on our experience as doctors of people who’ve had brain injuries for other reasons”.
Mr Justice Hayden addressed the crux of the matter:
Hayden: “It isn’t a question of will she ever be what she was, or will she walk and talk again. It’s a question of whether she might ever have restored to her a quality of life that you or I might reject, but she would want – because it reflects the way she lived her life and the values she has. She will never get to 90 but will she get from 2 or 3 to 5 or 10, and 10 – if it enables her to absorb the presence of and enjoy her grandchildren, might be something that would be good enough for her. Are we in that territory?”
Dr B: “In my view, no, My Lord”.
At another point, the judge and Dr B had this exchange:
Dr B: I would not be able to live that life. But that doesn’t matter.
Judge: If you felt that God makes that decision and not you or the doctor, then whether you can live that life or not wouldn’t be the point, would it. It would be the will of Allah.
Dr B: [Son A] has pointed that out to me.
Later Dr B said:
“We doctors who are looking after her, who started this ventilation, feel increasingly that it’s ethically and morally difficult to continue this treatment. How long does she have to suffer like this for the prospect that she might get to 10? … We feel desperate for the court to confirm that we are doing something that is lawful.”
This is how Mr Justice Hayden summarised his thinking during the course of the medical evidence:
“Putting it bluntly, she’s never going to change dramatically from the way she is now. She may have slightly more awareness than she has now and a greater understanding of what is going on around her, and a greater receptivity to pain. So the doctors say that, medically, this points to discontinuing ventilation. But factored into that has to be what I think she wants, based on the code by which she lived her life. I have to ask what are her values and beliefs and how do I most effectively respect her autonomy, which I don’t regard as having been extinguished. […] The doctors describe psychic distress, mental anguish, distress of the soul, however one might put it – but they recognise, in all humility, the limitations of their interpretation of how they find her.” (Hayden J)
Evidence from the family
At the earlier ‘directions’ hearing (14th July 2021), blogged here, AH’s family seemed to be (as Mr Justice Hayden put it) “unified around the same position” – that treatment should be continued. At that hearing, the judge asked them to prepare written statements for this final hearing and he spent all of the second day listening to their evidence.
The judge’s description of the oral evidence is “AH’s family members have exhibited a wide spectrum of views whilst endeavouring to advance a collective and unified response. In truth, each family member has, both knowingly and otherwise, vacillated as to the best way forward” (para. 3). The diversity of views and “vacillation” emerged largely as a consequence of skilled probing by the judge. In the judgment, Hayden J observes that “there is at the very least one family member who unambiguously supports the professional consensus” (para. 68).
This second day was a ‘hybrid’ hearing, i.e. some participants were in the physical courtroom, while others (including observers) joined remotely. This was at the request of some of AH’s adult children who wanted to meet the judge face-to-face. All but one – S, who lives in Australia – were in the courtroom.
In questioning the family, Mr Justice Hayden wanted to understand who AH was as an individual and to identify the “code by which [AH] lived her life so as to understand what decision AH would make for herself in this situation if she were able to do so”.
The family described AH as a strong and independent woman who had overcome considerable adversity in life – including leaving a violent and abusive husband, fleeing to a women’s refuge when the youngest child was five years old. It was suggested by some of the doctors, and by Mr Justice Hayden, that AH would find her current state of complete dependency and lack of privacy entirely unacceptable
She is an observant Muslim (listening to Islamic prayers, eating only Halal food) but “though it has been raised, the family has not emphasised an objection to withdrawal of ventilation on the grounds of Islamic belief” (para. 67).
Family members described some moments of pleasure and comfort that they had observed in AH while they were present, leading Mr Justice Hayden to reflect on the “delicate balance” between the small pleasures AH is said still to enjoy – the comfort she finds in the presence of her family, listening to religious recordings, watching Mr. Bean. On the other hand lies “the unimaginable burden of living for months subject to the rigors of ICU care, and suffering an unplanned death from infection.”
This exchange took place on the first day of the hearing:
Judge: The irony of it is that if I accede to what I might call ‘the family’s case’, it might be that I deliver a degree of misery to their mother.
Son (A) : I think she’s well aware of her existence now and has accepted it. You say that it would be for her best interest and for our interest to bury her. We would rather have a mum we can look after than one that we can visit at a grave.
***
By Claire Martin
Mr Justice Hayden’s approach is to help family members and witnesses to feel valued and as comfortable as possible. It is an approach that seems to enable people to speak with candour, having a sense that the judge is genuinely interested in them as a person and in what they have to say.
I remember wondering what it might be like for AH’s family to speak in court at such a difficult and upsetting time for them all. I felt admiring of their fortitude, and grateful that Mr Justice Hayden worked hard to put them at ease.
For example, at some point in the hearing, Hayden J interrupted Nageena Khalique (when she was questioning one member of the family in a direct way) to say ‘You know I like to take a long run at the wicket….’. He then proceeded to ask (I think it was A, AH’s youngest son) about what he did for a job and other more general questions. My sense is that, given that a judge has to make a decision one way or another in a contested case and at least one party will be disappointed, he wants to ensure that all parties feel, and are, genuinely heard and seen.
I have recorded here my recollection of what each family member said, with the exception of K – who must have given evidence, since he is quoted in the judgment (e.g. saying that he thinks his mother is in pain) but unfortunately I have no record of this.
Daughter [S]
AH’s daughter in Australia (S) was the first family member to give evidence. She looked very nervous initially, understandably.
In her written evidence, S said that her mother would “want us to do everything possible…to exhaust every possible avenue to get better”. In court, S was at first cautious in her responses to Mr Justice Hayden. He referred a few times to his understanding that she did not want to cause conflict within her family and that he would still like to hear her honest view of her mother’s values and expressed views before she was unwell, and what she thought her mother would want for herself in her current situation.
I don’t have notes of S’s evidence, so I am relying on my memory and impression of her – she was articulate, calm and composed. It must have been very hard for her. She said that she did not think her mother would want to ‘suffer’. Mr Justice Hayden asked S what her mother would define as ‘suffering’. I can’t recall the detail of her answer, but remember that her response was remarkably considered and empathic. She clearly outlined four different experiences that she thought her mother would define as ‘suffering’ – and they included specific descriptions of physical discomfort and emotional distress. They clearly encapsulated what AH is currently enduring.
It became evident to me, as the hearing continued, that the family members were not all of one mind in relation to AH’s best interests – and this itself was a difficult and upsetting situation for them all. I very much felt for them – AH’s situation was devastating, having contracted COVID less than a year ago and its impact being so severe, and irreversible, neurologically.
AH had started working at Cambridge University not long before the pandemic started; she was enjoying life with her family and her new job. All of the family accepted that AH would not ever be able to return to that life. There was less agreement about whether AH might improve in her functioning and subjective experience – and even if she did not, whether or not her current condition would be, to her, intolerable.
Sister (T)
AH’s sister (T) was the second family member to give evidence, via remote link. She talked about her sister with love, about happy times they’d spent together and about her sister’s faith. She described how AH’s children were central to her life and happiness.
She came across as very concerned about her nieces’ and nephews’ wellbeing – I saw her communicating with them with body language throughout the hearing and she clearly wanted to convey warmth, support and encouragement to them all. T really struggled, I thought, to reach a view about what AH herself would want in her current situation. She said that she knew her sister was in pain because she had asked her, to which AH had nodded a ‘Yes’.
Daughter [M]
AH’s youngest child, her daughter M, then came to speak to Mr Justice Hayden from the witness box.
As I’d been observing the hearing, M (and her brother A) were generally visible on screen too. Their emotional responses were plain to see at times – nodding or shaking their heads, especially A, AH’s son. My observation was that the energy in the room, embodied by M and A, was notable – they were a physical presence in the court. I had a sense that they were fully ready to speak up and wanted a voice.
M’s evidence was extremely affecting. She, too, was articulate. She was vibrant and engaged. Mr Justice Hayden had clearly worked hard to develop a trusting relationship with her – this felt very important, given what I witnessed during her evidence.
A consistent message that Mr Justice Hayden gave to the family, and most starkly to M and A, was (something like) this: ‘Your mother is dying. The question before us is not whether she is dying, but when and how she might die.’
At times, the judge was blunt and forthright with this message – though it was always infused with kindness and compassion for the impact such a statement might have.
When Mr Justice Hayden said this at one point during M’s evidence, she stopped dead. She looked at him square in the eye and said ‘She’s NOT dying’. She described how, in her view, AH had changed over the months and become more able to communicate, respond, react and understand what is going on around her. She viewed this as evidence for gradual recovery. She did not accept the expert evidence of Professor Wade and the other medical evidence, and stated that she believes ‘doctors do not know everything’.
I saw how M could not reconcile what she sees with her own eyes – that her mother’s situation had changed from no consciousness several months ago to some consciousness and communication now – with the idea that her mother is ‘dying’. As a daughter who desperately wishes her mother to come back to her, this is clear evidence of things moving in that direction.
M struggled to hear and absorb the medical opinions (all of one voice) that her mother’s life, in any event, would end within a year, at the outside. The question of whether it remained in AH’s best interests to continue with the life-sustaining treatment, given her pain and distress, felt too much for M to consider, given her own position that her mother was not dying, and in fact that she was improving.
Mr Justice Hayden encouraged M to describe her relationship with AH. M talked about a close, caring and fun relationship. She described looking after her mother (before she was unwell following COVID, as well as during her time in hospital this year). M would go to spas with her mum, take her on holiday and enjoyed pampering sessions at home together.
She (and her siblings) showed the judge videos of AH before her illness and also of her in the hospital – and Mr Justice Hayden expressed pleasure in being able to see those precious family memories and the court could also hear the sound of AH’s laboured breathing that the ventilator creates. He said he would ‘watch anything you want to show me’. I was moved by that – the judge was open to anything the family wanted to share with him. AH’s children left their seats to show him as many videos as they could locate on their phones. Hayden J at one point commented that they were competing to show them to him. The courtroom at this point felt less formal, as the siblings approached the bench and handed their phones back and forth to allow Mr Justice Hayden to watch family videos.
M was ‘very critical’ of the nursing care that her mother had received. She thought that some nurses did the ‘bare minimum’. She talked about when she was first able to visit her after the restrictions were reduced. She said that she was upset to find her mother ‘unrecognisable’ and that she herself set about tending to her mother’s personal care needs. She described bed sores that AH had developed and was clearly horrified that this had been allowed to happen. She said she looked up how to heal them, got some lotion herself and let the sores air dry, to bring some relief. She said that within two weeks, the sores had healed, and knew that her mother was much more comfortable. She also tended to her mother’s appearance and ensured that she would present herself to the world as she would have wanted to – Hayden J made reference to this in the judgement, when he went to visit AH himself in hospital:
M was forthright and assertive with the judge, and only towards the end of her evidence did she break down. Mr Justice Hayden apologised for making her cry. I recall him offering an explanation of why he was pushing her: to try to help her see that, for her, it was important to be able to take a step towards accepting that her mother was dying, and, that if she were able to do this, she might be better able to assist him to understand what AH’s wishes would be. Mr Justice Hayden expressed heartfelt understanding for M’s own wishes: that she loved her mother and wanted her to live. He voiced the clear message that M must consider whether there might be a difference between what she herself wishes, and what AH would wish for herself, in her current circumstances.
I started to form the idea that an additional function of court cases such as this – and certainly this court case – was to offer the family an opportunity to begin to accept the inevitable death of the person they love and to start to grieve for them. I have witnessed this before from Mr Justice Williams in this very upsetting hearing about a young woman who had tried to take her own life. I am sure something like this must have been in Mr Justice Hayden’s mind as he spoke compassionately to each family member.
His clear judicial task of reaching a best interests decision for AH was primary, and at the same time he regularly made reference to the opportunity for the family to make a consensus decision with him, rather than putting him in the position of making a singular judicial decision.
Son [A]
Mr Justice Hayden’s attempt to reach a consensus decision was clearest in his interaction with A, AH’s son. A conveyed a confident, almost bullish, attitude at the start of his evidence. I thought this covered a fragility that was not far from the surface. Like M, A also desperately wanted his mother to live and found it extremely hard to even begin to think about whether his mother would want anything different from what he wants for her.
Mr Justice Hayden (expertly and kindly, I thought) enabled A to describe his relationship with his mother and guided A to acknowledge that he was the ‘golden boy’ (judge’s words) of the family. It seemed that, over the years, A had come to see his own thoughts and feelings as indistinguishable from his mother’s. He spoke of interactions he had had with his mother in hospital, where he asked her questions, the answers to which he had interpreted as her conveying a wish to stay alive. Hayden J was able to help A think about why he might have received that communication from his mother. I recall Hayden J saying something to A along the lines of: perhaps the last person your mother would tell, if she felt she did not want to carry on, is you. At this moment, you could hear a pin drop in the courtroom. I thought this was a pivotal moment for A: he seemed to start to consider the possibility that he, specifically he, might not be able to ascertain, from asking her, what his mother’s wishes were. She would not want to distress him if her wishes did not accord with his own.
A described a relationship where he would do anything for his mother, and indicated that her needs were always paramount in his mind. Like M, A was sceptical of the medical evidence and, like M, he was critical of some of the care that AH had received (a view with which Mr Justice Hayden vehemently did not agree).
A also began to point out that his sister, S, was in Australia and was not around to see how his mother is progressing. At this point, it was clear that there had been, and probably was ongoing, discord within the family regarding AH’s likely wishes for herself. Mr Justice Hayden intervened – I had the sense that he saw no benefit in airing a family dispute, He noted that he found S’s evidence ‘very impressive’ and that she had attempted to consider what their mother would want for herself.
Mr Justice Hayden asked A to try to suspend his own wishes and consider, knowing his mother as he did, what she would want for herself. It was at this point that A became upset. The situation facing A felt impossible for him to countenance: that his mother was dying. I could see the conflict he was going through – it was palpable. How could he consider when and how his mother might die if he did not accept that she was dying?
Mr Justice Hayden allowed time (especially for M and A, who struggled the most to accept what their mother was facing) for what he was proposing to the family to be digested. Each time he made a statement that was hard to hear, to compute, he allowed some silence. I thought this was very therapeutic – it enabled space, to think, to feel, around the message that was being delivered.
At the end of the hearing, the most resounding thought in my mind was that, even if Mr Justice Hayden did not make a judgment concordant with some of the family members’ wishes, they would all have felt valued, honoured and heard.
*****
Although I (Celia) didn’t observe the second day of the hearing on which the family gave evidence about AH, I have watched Mr Justice Hayden question family members many times before and admire the skill with which he persistently maintains a focus on the person at the centre of the case. It is that person’s values, wishes, feelings and beliefs that are key to the best interests decision – and teasing these out from what family members want for the patient, or for themselves, is not always straightforward. These extracts from the judgment indicate some of the difficulties.
“A desperately wants his mother to live. Though he has the intelligence to absorb the impact of the medical evidence, his love for his mother causes him to retreat from the force of it. He devises questions to put to his mother in which he hopes to find evidence to support his own desire that she may continue to be ventilated.” (para 75)
“I formed the impression that [K] struggled to find the right words to express himself, in part because the ethical issues are complex but also because he did not want to offend his siblings, especially A. He struck me as bowed down by the weight of having to take a proactive decision one way or another about his mother.” (para. 87)
“ M had been absolutely clear to Professor Wade, when he interviewed her, that “if she had asked her mother what she would want in this situation before the illness struck, she (her mother) would not wish to continue”. This is no longer M’s explicit position, though her conflict about her mother’s welfare is almost palpable. She states that her mother’s improvement in consciousness causes her to hope that she might continue to improve to a degree which makes her life (i.e. her mother’s life), tolerable. She recognises that this optimism cannot be founded in the medical evidence but contends that doctors do not know everything and that her mother may yet confound them.” (para. 88)
The decision
As Mr Justice Hayden made clear, “An assessment of ‘best interests’ must, ultimately, survey the whole landscape of a patient’s medical, welfare and emotional needs” (para. 66). The goal of the hearing was to elicit the information required and then consider the options available.
The applicant Trust considered that AH had two choices, and Mr Justice Hayden believed that they had correctly identified the options.
“There are two choices for [AH]. One is continued treatment on ITU until she succumbs to a fatal infection, on the ward, at an unpredictable time, when there may be no family in attendance. The other is that she moves to a calm, quiet and private place, where the close of her life in this world can come to pass when she is back where she has always wanted to be – at the heart of her family – surrounded by their love, in an atmosphere of prayerful peace and togetherness.” (para. 102)
The judge rejected an alternative suggestion, from the Official Solicitor, that AH should continue to be ventilated outside the hospital – because this is not medically safe and risks “an avoidable, painful, unexpected death, with no family in attendance” (para. 77).
The judge recognised that “however depleted and compromised her life may have become, AH retains the capacity to feel and receive love”. He saw the comfort she receives from her family (and her faith) as offering “shafts of sunlight” penetrating her overarching misery or “moments of pleasure in the scorched landscape of her present existence” (para. 104). He also recognised that AH would have taken into account the comfort her family gained from seeing her – and this recognition is not (as one of the clinicians implied) about putting the family wishes ahead of the patient’s, but is rather “reflective of the central importance of family in AH’s hierarchy of values and beliefs”.
He concluded:
“I do not consider that AH’s best interests are presently met by ventilatory treatment in the ICU; ventilation is now both burdensome and medically futile; it is protracting avoidable physical and emotional pain. It is not in AH’s best interests that ventilation be continued indefinitely. It is however in her interests that ventilation remains in place until such point as all her four children and family members can be with her. This, I am satisfied, is what she would want and be prepared to endure further pain to achieve. I am also clear that it is in her best interests to be moved to a place which protects her privacy and affords her greater rest. The details of these arrangements can be worked out between the family and the treating team. One of the children is presently outside the United Kingdom and will have to make arrangements to travel. I hope this is possible, but I make it clear that ventilation should be discontinued by the end of October 2021. Though there is an inevitable artificiality to this, it reflects the delicate balance that has been identified. It provides an important opportunity for this close and loving family to be together at the end. The treating clinicians feel able to work with and perfect this plan and recognise that it is consistent with their own professional conclusions and reflective of the central importance of family in AH’s hierarchy of values and beliefs.” (para. 108)
Understanding the process of best interests decision-making
I don’t know whether or not Mr Justice Hayden has made the right decision in this case.
But a decision had to be made one way or another. I am glad the Court of Protection is there to do this, and I’m glad it wasn’t me who had to make the decision.
I don’t know for sure that AH would want ventilation withdrawn, given the tenets of her faith – but as Mr Justice Hayden points out (paras. 93 and 94 of the judgment), “on these difficult end of life issues there are differing views within each of the major faiths, including within Islam”.
I don’t know for sure that AH would want to continue to suffer pain and distress for up to an additional two months (so that all of her family members can be with her), while being given treatment that the judge describes as “burdensome” and “futile”.
I wish she could tell us herself what her views are, and what she wants.
But as the Official Solicitor noted: “There is no direct record of AH’s wishes as to what she would want to happen in this situation; she did not make an advance decision for herself”.
I’m not really sure that her family members know for certain what she would want in this situation either.
Any of us could suddenly lose capacity to make our own decisions about life-sustaining treatment – it might be a stroke or cardiac arrest, illness, or accident. Any of us could be in the position where others are having to make decisions on our behalf.
Family members (and doctors and judges) could really use support in understanding what we would want in this situation.
What Claire and I witnessed in the Court of Protection was a determined, serious, and lengthy attempt on the part of the judge to determine what AH would want, in the absence of any direct record to help him. Mr Justice Hayden tried very hard to find out what her wishes would be, and to respect them – giving effect to her autonomy and self-determination.
It’s common for people to make passing remarks along the lines of “if I’m ever like that, just let me go” or (conversely) “I’d want everything possible done to keep me alive”. But few people engage with possible future scenarios in any detail – preferring not to think about it, hoping it will never happen to them.
Only a tiny minority of us write down guidance for those who might in future need to make life-and-death decisions on our behalf. These ‘advance statements’ can be enormously helpful to decision-makers. They set out our values, feelings, wishes and beliefs (both the things we are certain of and those we are unsure about). We can explain what makes life worth living for us, the role of our religion (if any) in our decision-making, and the extent to which we’d want family views taken into account.
Written statements from the person at the centre of the case carry particular weight in Court of Protection hearings. In part this is because the law says that the judge “must consider… in particular any relevant written statement” (s4(6)(a) MCA) made by the person at a time when they had capacity.
Suppose that AH had written any of the following statements (based loosely on actual statements I’ve seen written by others), then how differently the hearing might have gone.
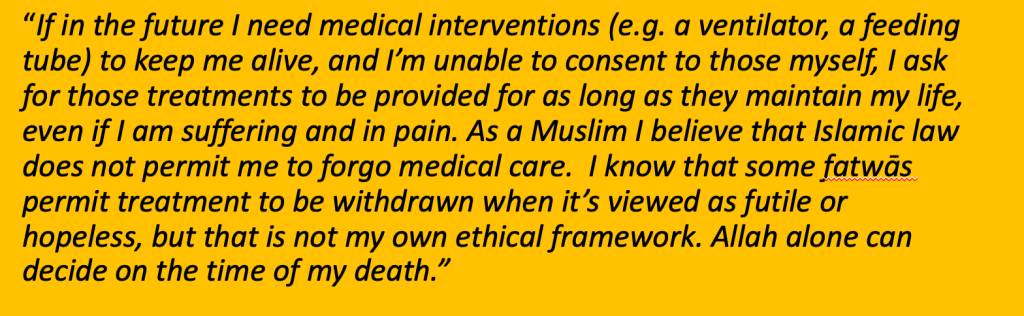
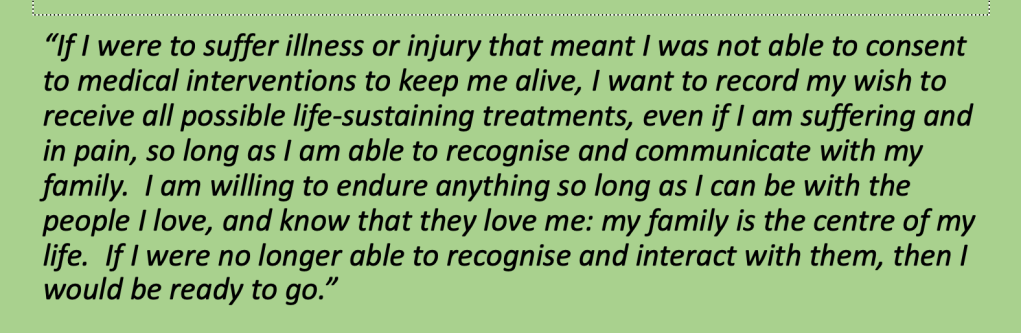
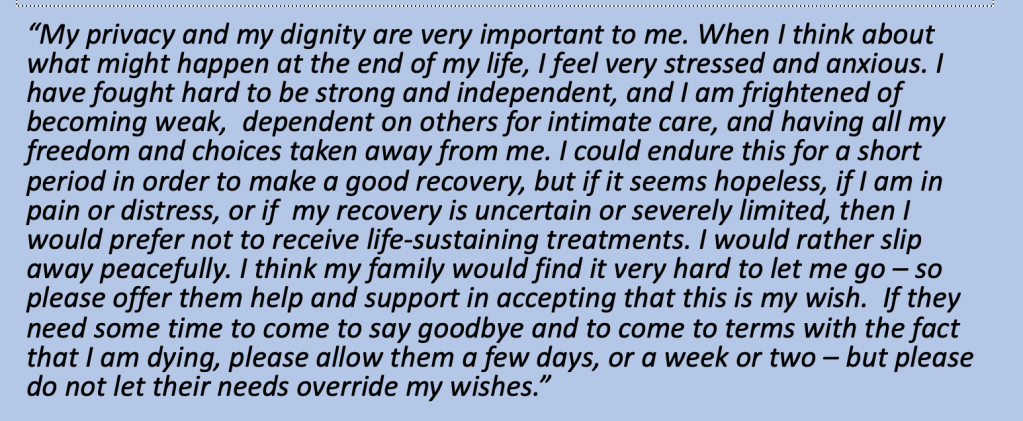
These sorts of ‘advance statements’ carry great weight in best interests decision-making.
We can also avoid ‘best interests’ decision-making altogether by making a legally-binding refusal of treatment. With a formal ‘advance decision’ (signed, witnessed and with some specified wording, see ss. 24-26, MCA), we can make our refusals known (e.g. “I refuse a feeding tube if I have advanced dementia”, “I refuse a ventilator if I’ll never be able to live independently again”). These are legally binding – doctors cannot lawfully administer the treatments refused in a valid and applicable advance decision.
Many people believe that ‘next of kin’ are decision-makers in situations like this but in fact, although family and others close to the patient must be consulted, it is the doctor providing treatment who must be satisfied that it is in the patient’s best interests – or where (as here) there is disagreement, a judge. Even if doctors believe a treatment is in the patient’s best interests, they cannot lawfully administer it if it’s been refused in advance.
Second-guessing what someone would want in a complicated medical scenario can be hard. Even if you are sure, convincing a doctor and/or a judge that you know the person’s wishes and that those wishes should prevail can be challenging. As I know from my own family experience, it can fail – even when the whole family is in agreement about what the person would want.
For myself, I have an advance statement laying out my values and beliefs to assist anyone charged with best interests decision-making on my behalf in the future. And I have also completed an Advance Decision to Refuse Treatment, since I know that I would never want to receive any life-sustaining treatment if I were in AH’s situation or anything like it. (Information about how to complete these documents is available from the charity, Compassion in Dying.). If I were ever the person that Mr Justice Hayden had to make a decision about, he’d have a lot more information to go on, and I’m confident that he’d find it a lot easier to make a decision in line with my own wishes.
It’s important for members of the public to understand the process of best interests decision making, as mandated by the Mental Capacity Act 2005, and as exemplified in Mr Justice Hayden’s judgment. Understanding the process enables us to decide for ourselves whether and how to contribute to it by making our own values and beliefs clear in advance, and stating that we would want, or that we refuse, certain treatments.
Understanding best interests decision-making also means we are better able to evaluate – and, if necessary, to challenge – decisions in the courts.
Browsing the comments on social media concerning this case (all of which draw on media reports, and not on the published judgment), I am saddened but not surprised by demonising references to Mr Justice Hayden as “condemning a patient to death” when only God should do so, and protesting against his judgment as authorising “euthanasia”.
In a democratic society, it’s important to be able to criticise the best interests decisions of individual judges, and to feel able to challenge the statutory basis (the Mental Capacity Act 2005) in relation to which their decisions must be reached. But without understanding the process of best interests decision making – and how to intervene effectively into that process – these protests are often wide of the mark.
Through the Open Justice Court of Protection Project we hope more people will be exposed to the realities of best interests decision-making in practice. We hope they will use what they learn to improve their own lives (and deaths) and those of their family, as well as to campaign for the medico-legal and social changes they believe are needed.
Celia Kitzinger is co-director (with Gillian Loomes Quinn) of the Open Justice Court of Protection Project, and co-director (with Jenny Kitzinger) of the Coma and Disorders of Consciousness Research Centre. She tweets @KitzingerCelia
Claire Martin is Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a member of the core group of the Open Justice Court of Protection Project and has published several blog posts for the Project about hearings she’s observed (e.g. here and here). She tweets @DocCMartin
Footnote
[1] BBC news (Covid: Judge rules patient paralysed by virus should be allowed to die)
ITV news (Judge rules Addenbrooke’s patient paralysed by Covid should be allowed to die)
the national press (e.g. Woman left brain-damaged and paralysed by Covid should be allowed to die, judge rules)
the Cambridge local press (Addenbrooke’s Hospital: ‘Most complex Covid patient’ will be allowed to die, judge rules)
and various international news outlets (e.g. Australia, UK woman paralysed by COVID allowed to die, Armenia (UK woman paralyzed by COVID was allowed to die) and in various non-English speaking countries (e.g. Mulher com lesão cerebral esquerda e paralisada por Covid deveria ter permissão para morrer, julga regras; Richter entscheidet, dass Frau, die von Covid gelähmt wurde, sterben darf).
Photo by Felix Mittermeier on Unsplash

This is another very interesting case. It is valuable to discuss these issues widely.
If it’s looked at @academically and rather hard nosed in a utilitarian context what would happen if every patient at the end of life was put onto intensive care for ventilation and organ support. I would suggest we run out of beds very quickly. International guidance is that intensive care is only provided to patients who will benefit. The clinical decision rests with specialists in intensive care, who have wide experience. If we accept that a patient on ICU will no longer benefit, should we not withdraw. Withdrawal is a medical decision based on lack of continued clinical benefit. Relatives are not asked to make the decision. Ethically there is no difference between withholding or withdrawing care, as the courts have confirmed previously.
ICU is a scarce resource, costs about £1500 a day and if beds are not utilised effectively other patients will be denied the opportunity.
What do others think?
LikeLike