
By Claire Martin, 17th June 2021
This hearing, on 6th and 7th May 2021 before HHJ Howells at Wrexham County and Family Court (COP 13575520 Re: B) was the second hearing I’ve observed concerning “David” – a 39-year-old man with a severe learning disability, poorly controlled epilepsy and congenital cerebral palsy with right-sided hemiplegia.
At the previous hearing, on 11th February 2021, I’d learnt that David’s care team, concerned about his night-time seizures, had installed a visual monitoring system almost two years before, without holding a best interests meeting about this, and without consulting David’s family. Counsel for David at the last hearing stated that there had been a ‘wholesale failure by either public body [to recognise that] a video monitoring system required a best interests decision’.
Having blogged about this case previously, I was very pleased to be able to attend what was (again) intended to be the final hearing for David, and a judgment on the issues of:
- whether a visual monitoring system (VMS) is in David’s best interests, and if so, how this will be deployed and monitored, and
- whether the public bodies should be responsible for paying David’s legal costs.
The applicant was David, represented by Emma Sutton and instructed by David’s litigation friend, his Relevant Person’s Representative. The respondents were the local authority (Pembrokeshire County Council, represented by Robert Goodwin), Hywel Dda University Health Board (represented by Anna Tkaczynska) and David’s parent (her choice of descriptor), who was a litigant in person.
When the hearing started, I was asked to confirm to the judge that I had received, read and understood the Transparency Order for the case. I was the only public observer on this occasion and the judge (HHJ Howells) noted that I had previously written a blog about the same case, which I was surprised to hear her comment on to the court!
Delayed Submissions – an ‘unfortunate situation’
The hearing started inauspiciously, with HHJ Howells stating that it looked like there might be a ‘change in position’ from some parties, though noting that the ‘amended bundle … amounting to 435 pages digitally, was only filed yesterday or the day before’. It transpired that the position statement for the Health Board, as well as their updated care plan proposal were only filed on the day of the hearing (due to start at 10.30am). This is despite the fact that – as I noted in my previous blog about this case – “The judge asked for Position Statements forty-eight hours in advance to allow all parties to read and digest the contents.”
Other documents (care home records, MDT meeting minutes, an article from a medical journal, some emails) were said to have been ‘filed very late’ and Emma Sutton (counsel for David) said there was:
“… a plethora of additional information [submitted] an hour before a two day trial. I am making my way through it but there is a significant amount of information. … This is a wholly unacceptable position the Health Board has put people in.[1]”
It became clear that the Health Board had failed to provide the required updated information or position statement by 4pm on 4th May, when the hearing was at 10.30am on 6th May. The judge said that ‘costs will be considered’ and addressed counsel for the Health Board: “Ms Tkaczynska you have a chance to explain”.
In response, and by way of explanation, counsel for the health board ran through a list of documentation, when it was filed, who received what from whom, and there ensued a multi-way conversation between all barristers and the judge about when documents were requested, why they weren’t chased when they were not received and why the Litigation Friend for David (his RPR – Relevant Person’s Representative) had been missed from some communications (it emerged that an incorrect email address for her was used in communications from the Health Board). This was then not rectified, meaning she was not included in a Best Interests meeting. I observed the judge with her head in her hands at one point, looking exasperated.
“One would have thought that if the litigation friend didn’t respond it would have alerted others to the need to chase up, but this doesn’t appear to have happened. …. I have received all these [documents] and I am willing to proceed but it’s not fair on others, especially counsel for [David] and his parent.” (HHJ Howells)
Emma Sutton suggested a half hour break to give people time to read the documentation. The judge thought that ‘optimistic [because] important information needs to be absorbed as well as read’. I was struck, especially, by the judge’s care for David’s parent, who was representing herself, and was abroad, in a different time zone and had not received all of the relevant documentation until the morning of the hearing. The genuine consideration of what this might be like for her was palpable, and it was made clear that she could ask for longer if she needed more time:
HHJ Howells: “This is an unfortunate situation – especially for the litigant in person. [Addressing David’s parent] you have permission to drink caffeine!”
We returned at about 12.20pm. It was still not clear (to anyone) what the Health Board and Local Authority’s positions were – either in relation to David’s care needs, or their proposed options to meet those needs or their proposals to put different options into effect. Emma Sutton noted that this needed further exploration. David’s parent’s view was that the VMS should be removed ‘immediately’.
Evidence from the Expert Witness
The first witness was Dr Dougall McCorry, a Consultant neurologist and epilepsy specialist.
He was a witness for David, the applicant, and so Emma Sutton opened the questioning to elicit the evidence in chief. She took the witness through his expert views on the practice of video-monitoring for epileptic seizures, the types of seizures most associated with SUDEP (Sudden Unexpected Death in Epilepsy), David’s particular risk of SUDEP and Dr McCorry’s view of the best way to mitigate those risks.
Emma Sutton went on to explore movement monitors (e.g. wrist alarms), mattress alarms and anti-suffocation pillows.
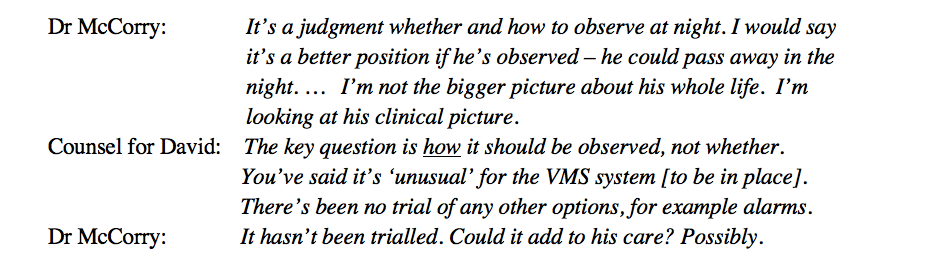
Cross-examination followed. Anna Tkaczynska (counsel for the Health Board) asked questions about proposed additional staffing for observation, the likelihood of picking up and attending all seizures and the balance of risk and privacy for David. Dr McCorry was clear that, from a clinician’s perspective ‘the gold standard is observation at all times’. This led to the following exchange:

Counsel for the Health Board then asked Dr McCorry to clarify the view from his supplementary report regarding the reasonableness and efficacy of trialling other monitoring technology. Dr McCorry replied: “In the current care plan – are we adding to his care? Will we detect more seizures with a mattress or movement alarm? If you really want to know what percentage you’re picking up, you must observe as well, to audit.”
This point – about accurate measuring of the percentage of seizures that can be detected by different monitoring practices, was really the nub of the case.
It later became clear that evaluation of the VMS had never been part of the installation plan in terms of whether it increased the number of seizures it accurately picked up. So how could the team know if that level of intrusion might be justified? This seems like a really important point to me – the VMS was simply installed on the advice of the treating clinician without a plan to collect evidence of its safety benefits over time, to weigh against the intrusion into David’s privacy.
By the end of Dr McCorry’s evidence in chief, I thought he was suggesting that the permanent observation of David (including using the VMS) was a certain way of picking up all of his seizures. However, further questioning of Dr McCorry by David’s parent (as well as later evidence from David’s treating medical consultant) suggested otherwise. It became clear that VMS for people with epilepsy (including David’s kind of epilepsy) is quite unusual – his treating clinician later stated ‘5% of people I see’ have a VMS set up. It also wasn’t entirely clear why this had been implemented for David at the time it was. Furthermore, he hadn’t had any of the types of seizures of concern, at night, for over a year (which I think were the original justification for the use of the VMS).
There was a break for lunch and at 2.25pm the hearing resumed with an expectation that David’s treating clinician would be the next witness for the Health Board. Prior to this, however, it was reported that agreement had not been reached between the public bodies for funding of additional care at night for David. This was important because the treating clinician would be questioned on different potential monitoring methods for David, which would necessitate more staff at night (and thus increased funding).
A discussion ensued between Robert Goodwin, counsel for the Local Authority and the judge regarding the LA position on funding of additional care for David. Robert Goodwin reported a misunderstanding between the Health Board and LA regarding the funding ratio as well as how additional care resourcing would be deployed (solely for David or shared). Frustration rippled through the court:
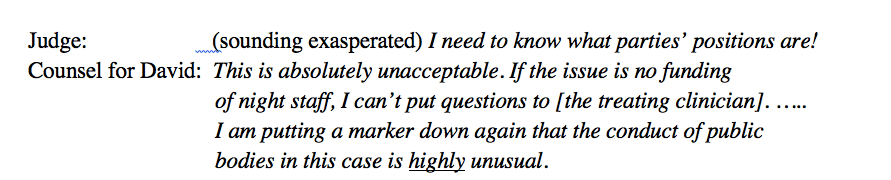
The judge addressed David’s parent: “The Health Board and the Local Authority are at cross-purposes in terms of funding an additional person – whether this is for [David] or to share with others. Are you prepared to continue?“ David’s parent replied ‘Yes’.
My reaction at this point was astonishment at how patient the judge and David’s parent were. The care system appeared in a mighty pickle about all sorts of things, and readiness for the hearing with clear and comprehensive options appraisals, care plan proposals and funding had not, seemingly, been their priority.
The hearing nevertheless continued with evidence from David’s treating clinician.
Evidence from Treating Clinician
David’s treating clinician had known him for 15 years. Counsel for the Trust asked minimal questions of her witness and then counsel for the local authority cross-examined him, focusing on evaluation of the VMS and staffing required for this. David’s treating clinician outlined his view of what would need to happen to reduce the use of the VMS: at least a year with no overnight seizures. He said “In my view [David] needs to be observed at all times – how that’s done is for the care team”. Irrespective of the lack of legal process regarding deprivation of liberty, I found it curious that, how it was subsequently deployed (2:8 staff:resident ratio) meant that the VMS could not facilitate ‘observation at all times’.
Litigant in Person cross-examines David’s Treating Clinician
I found this part of the hearing fascinating. It is important to know that David’s parent is a medical doctor herself and had done a lot of research about the nature of David’s epilepsy, risk of SUDEP and how best to mitigate those risks. She asked about population versus individual risk for David and proffered a view that, for people such as David, the longer they live without ‘succumbing to SUDEP’, the less at risk they are as time goes on. The treating clinician disagreed with this view. His estimate of SUDEP risk for David was 1:300 in any one year.
I have not heard a litigant in person question a witness before. I am not sure how common this is in the Court of Protection. It was a particularly affecting exchange because David’s treating clinician had seemingly had a good relationship with his parent over 15 years, and he clearly cared about David’s welfare. At the same time, it was evident that something had gone very awry with the planning and communication around David’s care.
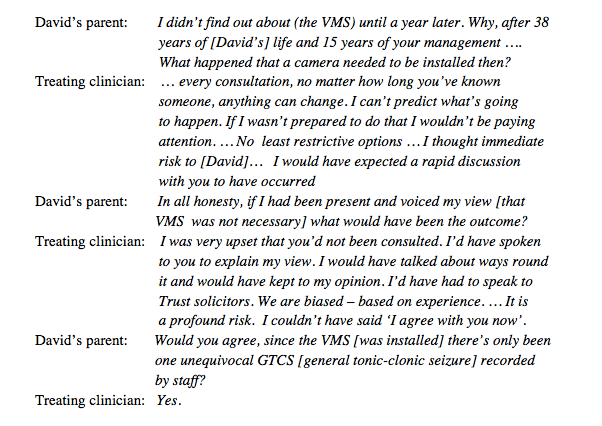
It was my understanding that the night-time GTCS were the reason for the installation of VMS, so this was a pertinent point raised by David’s parent. They then discussed evidence around SUDEP and comorbidities, papers that the treating clinician cited (but did not provide) in his evidence. The treating clinician said that the ‘SUDEP data doesn’t allow such a fine-tuned analysis’.
David’s parent had asked very probing, evidence-based, questions regarding risk and mitigation of risk, and applied them to David’s recorded seizures. The treating clinician seemed somewhat flummoxed by this and I felt unconvinced that he had properly considered whether the VMS would actually offer the protection to David that he proposed it would. David’s parent was of the view that it did not, and therefore the intrusion into his privacy was not justified.
Counsel for David, Emma Sutton, then picked up this line of questioning and argued that the blanket, night-time VMS – which was meant to offer ‘observation at all times’ to mitigate risk – was not, in reality, viewed at all times.
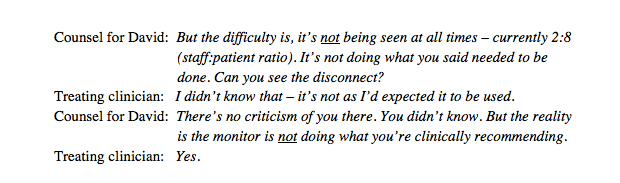
As counsel for David, Emma Sutton’s questioning was concise, incisive and absolutely to the point. She had clearly extracted the key pieces of information regarding the process of David’s care and was able to lead the court along a path that revealed a clearer view of the issues. Here’s an example:
Following Emma Sutton’s questioning, my sense at this point was essentially this: that the medical consultant involved in David’s care took a cautious and conservative approach, without considering a range of options. Everyone (who was included in the process) deferred to the medical consultant’s view. Apparent blanket observation was decided upon, due to his worries about night-time seizures. How this was then operationalised was not specified and did not, in reality, afford the additional protection he desired. The treating consultant did not have a full grasp of how, and how effective, the monitoring of the seizures was.
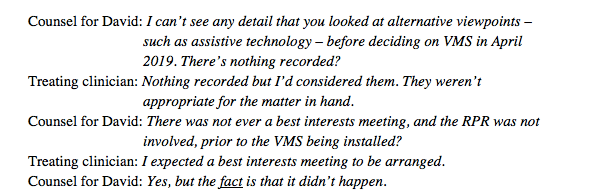
Leaving aside the unlawful installation of the VMS, the use of the monitoring device in practice felt very messy without a plan for evaluation of its effectiveness. I was also struck by the treating clinician’s response of ‘expecting’ a Best Interests meeting to be arranged – if he had expected it, and it hadn’t happened, why didn’t he rectify this situation (especially since it is a legal requirement)?
Further questioning from counsel for the Health Board and the judge further displayed the difficulty of establishing a clear picture of how a trial (of any technology) would be put into operation and then evaluated carefully. I came to the view that this was because alternative, less intrusive, means of monitoring David’s seizures had simply not been considered. An earlier question from Emma Sutton (counsel for David) perhaps sheds light on why this might be:

I would have thought that’s exactly what did need to happen, under the MCA 2005.
The fact that David’s RPR was not part of some meetings, the fact that a BI meeting was not arranged prior to the VMS being installed, and the fact that his parent was left unaware of the presence of the VMS for a year after it was installed, would suggest that privacy hadn’t been on anyone’s radar for David.
That was the end of Day 1. My takeaways were that:
- David’s treating clinician was, understandably, worried about his night-time seizures and recommended a VMS to be installed. This recommendation was actioned by the care system without following the Best Interests process required by the Mental Capacity Act 2005.
- The treating clinician was oblivious to the evidenced fact that he did not know how the VMS was actually used in practice, and to whether and how evidence was gathered to enable evaluation of its effectiveness, so it was not possible to know if it had, actually, improved monitoring of David’s seizures. The situation reminded me of this quote from Noam Chomsky: “Science is a bit like the joke about the drunk who is looking under a lamppost for a key that he has lost on the other side of the street, because that’s where the light is. It has no other choice.”
- The Health Board and Local Authority had not reached an agreement for additional night-time funding, or a plan for different monitoring options.
Day 2: 7th May 2021, 9.30am.
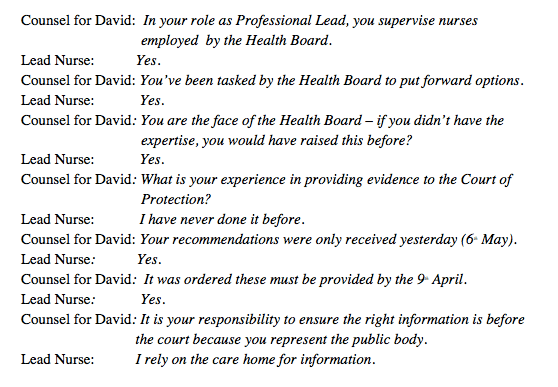
The Lead Professional Learning Disabilities Nurse from the Health Board was questioned. as a witness for the Health Board. (I’ve referred to her as Lead Nurse below.)
Before her testimony could be considered, DJ Howells discussed the unresolved issue of funding between the Local Authority and the Health Board. Robert Goodwin for the Local Authority offered an apology for the ‘confusion’ about funding. He said, “We have had limited evidence from the Health Board and did not understand what they proposed regarding extra night staff.’ The Local Authority was willing to fund 40% of this additional staffing. This was agreed with the Health Board and the hearing was able to continue.
Counsel for the health board asked the witness to describe her role. The Lead Nurse explained that she oversees the nurses from the Health Board who look after David’s care. Her role in the CoP hearing was to bring together a full options appraisal (for the monitoring of David’s epilepsy) for the court to consider. A curious exchange occurred at the start:
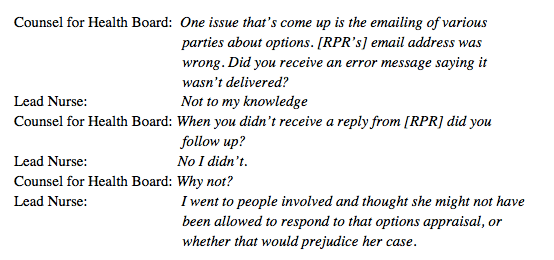
I was very surprised to hear the lead nurse’s reason for not ensuring that David’s RPR was part of the options appraisal for his care. What she would have needed to support that reasoning was an email back from the RPR stating that she was not allowed to respond to an options appraisal. This was not what happened.
Robert Goodwin for the Local Authority then cross-examined the Lead Nurse:

She then referred to minutes from a Best Interests meeting of 9 July 2020, chaired by a Mental Capacity Act practitioner from the Health Board. The judge asked if the minutes were in the bundle – they weren’t. Counsel for the Health Board stated that she did not know why they weren’t shared; they were an 8-page document. It was agreed that the court needed a twenty-minute break to read this document and the judge (addressing David’s parent) said: “Please say if you need more time to read these. Someone acting for themselves should have plenty of time. My tone says what I think about this.”
And addressing counsel for the Health Board, the judge said: “This is not the way it should be done – piecemeal disclosure. It is not fair for [David’s parent] to not have all the information which is under consideration. I suggest everyone goes for a cup of tea. I’m leaving this hearing yet again.” (Judge)
When we returned the judge addressed David’s mother once again:
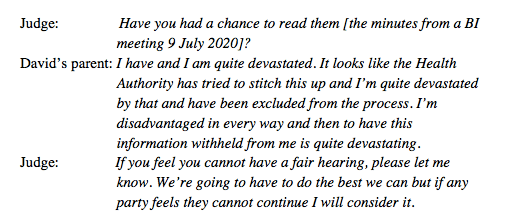
All agreed to continue. I felt angry on David’s parent’s behalf at this point. She had not been informed about a video-monitoring system for him, had not been included in a subsequent Best Interests meeting when it did, eventually, take place, and her right to have a voice in these processes had been entirely over-ridden. It felt as if, because the care team knew she might hold a different view to theirs, they simply wrote her out of the story.
Counsel for the Local Authority, Robert Goodwin, continued his cross-questioning and asked the lead nurse about assistive technology being considered at the Best Interests meeting on 9 July. She said she had not been in that meeting and couldn’t comment on ‘how the discussions went’.

It was beginning to look as though no one whose responsibility it was to oversee David’s care (his treating clinician and the lead nurse who was tasked with drawing up an options appraisal) had entered into a deliberative process about methods to care for David, balanced with his human rights. I kept wondering: ‘what if a video-monitoring system IS, in the end, in David’s best interests and they just hadn’t done the working out’.
It reminded me of another case I observed, and contributed to a blog about, called ‘When Expert Evidence Fails’. In that case, the expert witness expressed a clear view about P’s capacity to consent to sexual relations, but had not followed a clear, deliberative process to reach his decision. This seems to me so important in our work with vulnerable people who might lack capacity for certain decisions. Without this demonstrable process, it can look like, and I would suggest often is, our own view of what is best for P, rather than a holistic, person-centred consideration.
Further, when one professional’s view dictates the outcome, this seems even more likely to be the case – privileging only what we consider to be in the best interests of the person, based on our expertise in that one very specific aspect of that person’s care. As Dougall McCorry said earlier: “I’m not the bigger picture about his whole life – I’m looking at his clinical picture”David’s parent then cross-questioned the witness. She picked up Robert Goodwin’s questioning of the lack of consideration of all options for monitoring David’s epilepsy, noting especially that there had been a Best Interests meeting on 9th July 2020 and the options appraisal had not been available until 7th April 2021, nine months later. Her questioning illuminates potential issues with a best interests process sitting with one ‘dominant voice’:
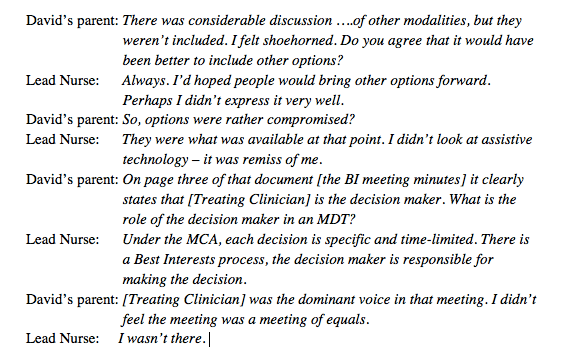
Further questioning from Emma Sutton showed that the balance of safety and privacy for David really had not been considered. There were several quite terse and revealing exchanges:
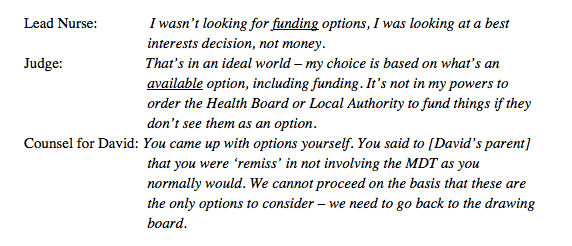
There was then discussion again between Emma Sutton, the lead nurse and the judge about the fact that the Health Board’s recommendations were based on increased funding, yet, at the start of the hearing, funding for those recommendations had not been secured with the Local Authority:
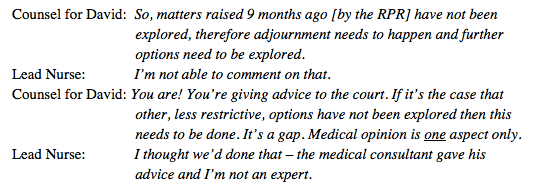
And later in relation to the RPR asking for ‘less restrictive options’ to be considered:
I wondered whether the lead nurse had been placed by the Health Board in an invidious position. She did not seem to feel confident in guiding all the people involved in David’s care and welfare through a thinking, questioning and balancing process to compile a balanced options appraisal – something for which you do not need medical expertise.
Counsel for the Health Board intimated that there would be no point adjourning) since “What else needs to come to the table? Would anything else trump [treating clinician’s] view?” Although the Lead Nurse thought nothing would, the judge pointed out:
But [treating clinician] is not the decision maker in the Court of Protection. He might be in the Health Board, but not here. It might not change the Health Board’s decision but it might provide more information to the court, so we can weigh in the balance for [David]. At the moment [lead nurse] evidence is that she accepts that these should be looked into. (Judge)
With that, it was agreed to break for a joint parties’ meeting to confer about ways forward. This was 12.19pm.
My thoughts at this point were, first, this seems like an almighty mess! Two days of court time (plus previous hearings over the past year) and there was still no comprehensive options appraisal, care plan proposals for different options that were proposed or funding agreed. I might be being unfair – we have been living through a pandemic during this time – however, the VMS was installed prior to the pandemic and I couldn’t help thinking that, had due process been followed then, the case might not have needed to come to court.
Second, I thought that there was a lot of buck passing: submissions for the court and bundle documents were not ready for the hearing, varying reasons for which were proffered; the Local Authority implied the Health Board had not apprised them of their proposals to enable the LA to form a view of their position on funding; the lead nurse appeared to blame the care home (which, at other times in the hearing, was described as ‘exemplary’ in their care practice) for not providing timely information to inform the options appraisal; the treating clinician seemed to ‘expect a best interests meeting to be arranged’ but took no responsibility for this himself, despite being designated the decision maker by his employing organisation. All in all not very edifying.
At 12.47 the judge returned to the hearing (I had stayed logged in throughout, as I was never sure when breaks were going to end and parties return to court). At this point it was just me, the judge and her clerk in the courtroom. DJ Howells said ‘I hope Dr Martin is enjoying observing all of this’, which made me laugh (though I had my microphone off of course). It was certainly a spectacle – and the fact that David himself was not in any distress helped me, at least, to feel more astonished than angry at the situation.
Parties returned to the courtroom and it was agreed that there would be a round table meeting over lunch, including all lawyers, to consider all options.
At 2pm we resumed. My notes read: “Robert Goodwin looks thoroughly fed up. Judge asks Emma Sutton ‘where are we?’”
Emma Sutton, as counsel for David, said:
We have agreed a way forward. There is a gap that needs to be filled. There will be a meeting including [treating clinician] and Local Authority and it’s agreed that an occupational therapist needs to be involved for an assistive technology assessment. We’ll consult Epilepsy Excellence Centres regarding alternatives for care. A possible expert witness – it depends. Then the procurement team needs to be involved regarding devices to see what they can provide. The Lead Nurse is then to provide a pros and cons document including safety, accuracy etc. Then a round table meeting and further court hearing to be built around that. There is a pot of money for additional care now in place [the 60:40 Health:LA agreement from earlier]. Timescales have not yet been decided.
The judge responded (very charitably I thought!) by thanking everyone for “the collaborative approach to proceedings.” She said: :”It seems to me there is a measure of agreement that this should have been done, but there are pressures on people’s time, it’s not deliberate and people ran out of time.”
A further break between 2.15 and 3.15pm allowed the drawing up of the terms of the order from this hearing, including extending the standard authorisation for the VMS, and dates for different people for various tasks to be completed. A round table meeting is planned.
Of particular importance, I thought, was the agreement for the lead nurse to provide, as part of the Health Board’s proposal, details for how the VMS would be used, were it to remain in place. It was evident from this two-day hearing that this had never been planned – it was not specified exactly when to use it (though the lead nurse clarified ‘when asleep’ there was confusion whether it was used ‘at night’ and when David was ‘in his room’ even during the day if asleep); or how to record when a seizure was detected by the VMS as opposed to other means, such as staff being in the room with him (though some records did state ‘observed on video’ it wasn’t known whether this was consistently, and therefore reliably, recorded). The lead nurse had earlier confirmed her view that she would be ‘mortified’ herself, if she was being ‘watched all the time’. She clearly empathised with the intrusiveness of being watched on video in your bedroom. Even more important then, to ensure that any future, court-authorised observation is proportionate and deployed in a carefully monitored and reviewed manner.
Final Thoughts
I have observed around 15 remote hearings now across the pandemic period. None has been as chaotic as this – with respondents not being organised in their communications with each other in preparation for court and court orders simply not being followed. A crib sheet of preparation tips for Trust employees appearing at the Court of Protection would be a good idea! Certainly, for this hearing the following would have been helpful:
- Ensuring that – and being able to demonstrate – that you have meticulously endeavoured to include all relevant people in Best Interests meetings and decisions for P, checking the MCA 2005 for guidance if you are unsure about who this should be (e.g. s4(7) Best Interests decisions and who should be included). In this case David’s family and his RPR were not consulted at appropriate times throughout.
- The person making the subsequent Best Interests determination (in this case we were told that David’s treating clinician was the ‘decision maker’ and the Lead Nurse was producing the options appraisal) should have considered all relevant people’s voices to produce an options appraisal document in readiness for the court hearing – and be able to demonstrate that this consultation process had been followed.
- Referring back to any previous judicial orders in earlier hearings – well before time – and ensuring they are adhered to. This could be facilitated by liaison between parties to chase up required information for documents and to establish agreement or highlighting of areas of ongoing disagreement in readiness for the court hearing. I wonder whether, sometimes, a reminder phone call would be better than an email!
- Circulate all documents to be included in the court bundle by deadlines ordered to enable all parties to ‘read and digest’ (as noted by DJ Howells) prior to the court hearing.
- A willingness to see the ‘wider-picture’ (or ‘holistic’ picture as David’s parent put it) about a person’s needs and care: that our lives are a balance of risks, including for people who do not retain capacity for certain decisions in their lives.
For David, it felt as if an appearance of belt and braces was wanted in his care (i.e. being watched at all time), without the evidence to demonstrate that this reduced risk of harm. So, we could be looking at an invasion of David’s privacy without the added safety that was it was designed to guarantee: an absence of due process and an outcome that did not do what it said on the tin.
I hope to be able to attend the – hopefully – final hearing which is planned for the 15th or 16th July 2021.
Claire Martin is Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is part of the core group of the Open Justice Court of Protection Project and has published many blog posts about hearings she’s observed (e.g. here and here). She tweets @DocCMartin
[1] As usual, I have attempted to render what people said as accurately as possible, but it’s unlikely to be entirely verbatim since I have to rely on my note-taking skills during the hearing, being forbidden to audio-record.
Photo by Steve Johnson on Unsplash

One thought on “Chaos in court and incompetent decision-making: Visual monitoring Part 2”