
By Rebecca Brione, 21st June 2021
Editorial Note: This judgment has now been published: University Hospitals Dorset NHS Foundation Trust & Anor v Miss K [2021] EWCOP 40.
I am a bioethicist and reproductive justice researcher. I am also currently the Research and Partnerships Officer at the charity Birthrights, which works to protect human rights in childbirth. I have been following maternity cases in the Court of Protection in both capacities for some years, but I had never previously observed a hearing.
I particularly wanted to observe a hearing concerning decision-making about childbirth because I have significant concerns about how decisions have been made about obstetric intervention in previous cases – in particular the tendency to conflate maternal and foetal interests, the sense that women’s voices are often lacking, not properly heard, or dismissed, and assumptions about what ‘safety’ in birth means.
My interest in Court of Protection decisions on childbirth was first spiked by the media storm around the Re AA case in 2012, in which the Court authorised a Caesarean on a 39-week pregnant Italian woman, originally in the UK for a work-related visit but subsequently detained under the Mental Health Act 1983 after she stopped taking medication and become unwell. The Court found a Caesarean to be in her best interests, apparently due to the risk of uterine rupture. Her voice was completely absent from the proceedings, and her baby subsequently (and separately) removed into child protection. Inaccurate (and in some cases hyperbolic) media commentary led to the judgment in the case being published in 2013. In fact, the imperative to publish in this case forms part of the push for transparency in the Courts that made it possible for me to observe now.
In the intervening years, there have been a significant number of obstetric intervention cases, including a recent case I blogged about in which the Court authorised planned transfer to hospital for an agoraphobic woman who wanted a home birth. I had been unable to observe that case as remote attendance was not permitted, so my blog – like the others in the series – is based on the published judgment. Whilst these are invaluable resources, I am always aware that they paint only a part of the picture, and that as a reader you don’t always feel confident that you can really understand what went on behind the scenes: how the case came to Court in the first place, what support the person at the centre of the case had received and experienced, and what happened during the hearing.
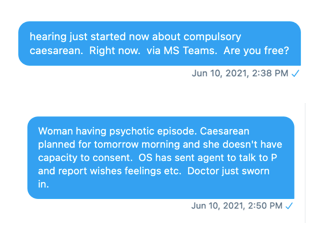
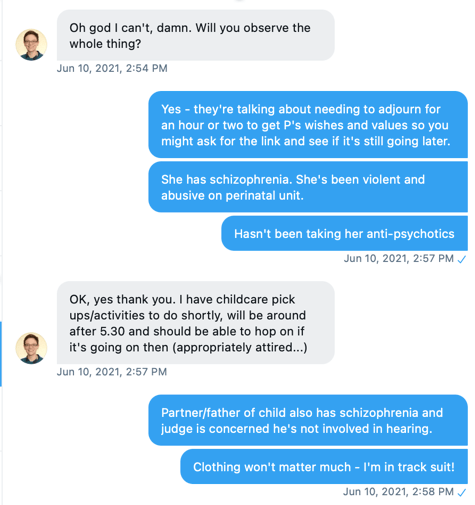
I was therefore really keen to observe a case for myself. When Celia messaged me at about 2.30pm on Thursday 10th June 2021 asking if I was free “now” to observe a hearing, however, I have to confess my first thought was of being utterly unprepared. I wasn’t ready, I had other commitments, I was nervous. Thankfully pragmatism quickly took over – I found a shirt to go over my running clothes and emailed requesting the link, which was promptly sent. I logged on to observe. I am so glad that I did. It will not be the last time!
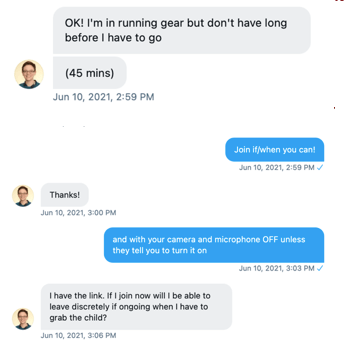
In this blog I will share some of my reflections on the process as well as on the case. I have to be clear that I did not observe the whole hearing and I missed some parts at the start, and another part after an adjournment, that would have been really helpful for me to hear. I must say, though, that being able to observe remotely made the whole experience so much more accessible than it would have been. I could access the hearing immediately, I could and did nip out to collect a child mid-way through. I would not have been able to observe this case had it required in-person attendance.
The hearing
The hearing (COP 13766836) was about whether or not it was in the best interests of a pregnant woman (Miss K) in her late 30s with a diagnosis of schizophrenia to undergo a planned Caesarean section. It was a complex and challenging situation.
At the point at which I joined the hearing (about 3.00pm), the Court was hearing evidence from the treating consultant psychiatrist, Dr B, who had been overseeing Miss K’s care for the previous fortnight or so. The judge was Mrs Justice Lieven and the two barristers in Court were Emma Sutton (for the Trust) and Katie Gollop QC representing Miss K (via the Official Solicitor).
Miss K had discontinued medication when she realised she was pregnant and was now “acutely distressed and unwell”.
Dr B described Miss K’s behaviour as variable but as having recently deteriorated, and she was at times being restrained, sedated and isolated in the Psychiatric Intensive Care Unit (PICU) where she was detained under s. 2 of the Mental Health Act 1983. Dr B said this was an unusual case: “I do locked wards: only the most seriously ill patients come to me and we hardly ever have pregnant ladies on our unit”. Miss K was refusing oral medication and being given intramuscular injections.
Dr B said that Miss K had been “compliant” with antenatal services and had recently gone “willingly” for an ultrasound. He said the difference in engagement was difficult to explain, although he did comment that obstetric care helped assuage some of her “paranoid delusions about the foetus”.
He was asked about waiting for labour to commence naturally:
“If we wait for spontaneous delivery we’d need to wait another few weeks and the patient is not easy to manage. We have to go lightly with doses of anti-psychotic because of the pregnancy. There are risks associated with physical restraint. We don’t have adequate access to monitor the baby…. It’s difficult to listen to the foetal heartbeat because we don’t want to put our heads too close to her tummy, because we might get thumped – it’s as simple as that”
He also noted that the psychiatric and obstetric units are about two miles apart, meaning that transport and staffing to support (or manage?) Miss K played into the decision.
Care Plan
After hearing this evidence, the Court turned to look – with the witness – explicitly at the care plan. I did not have a copy of this, but was significantly aided in my understanding by the thoughtful questioning from both Counsel for the OS (Katie Gollop QC) and the Judge who asked lots of questions herself and seemed very focussed on keeping Miss K at the centre of case.
In particular they raised concerns about the plan for her psychiatric care and support post-Caesarean (if ordered). A meeting on 20th May 2021 had led to a plan for the baby to be removed at birth by the Police using their powers of protection pending the Local Authority applying for an emergency protection order. Miss K was not told of that plan until two days before this hearing.
The Judge asked: “At some point she’s been told they are removing the baby. Has she experienced that as distressing?”. “Yes”, said Dr B, “I think she has”.
Little thought seemed to have been given to Miss K’s care needs on coming round from a general anaesthetic to find her – much wanted – baby to have been removed. The care plan seemed to assume that she would be relatively sedated for a lengthy period as a result of the general anaesthetic; something the Judge questioned (“not speaking from personal experience”) as being ‘not normally the case’ for a Caesarean, “where the dose is often quite a light dose and wears off quickly”.
In this context the care plan post-birth was described as a “recipe for severe problems”.
“You’ve potentially got a very, very distressed patient here. She comes round from a major operation with no baby. She’s highly distressed, and she in the obstetric unit not the psychiatric unit. I’ve seen videos of physical restraint. It’s not a pretty sight however well trained you are. The care plan has about a page and a half about physical restraint at this point – physical restraint on a woman who only hours before has had a caesarean. The plan needs to say more about the alternatives to restraint after the birth”
The care plan also needed to say “more about before the birth” added Emma Sutton. “Yes”, said the Judge, “let’s call a spade a spade. She’s being forced into an ambulance to have a Caesarean to have her baby removed.”
The care plan seemed to be focussed much more on the use physical restraint than supporting Miss K with her distress in the immediate term and after discharge – and whilst this was disturbing to hear, I was also really heartened by the way the Judge and Katie Gollop QC for the Official Solicitor kept returning to this point. They raised what seemed to me to be highly practical concerns about ensuring safe wound care as well as asking questions about why there wasn’t more consideration of use of family support or medication, given the “page and a half” in the care plan on physical restraint. Whilst the Judge said that she knew that “none of the medication is going to resolve the fundamentals of the situation”, it was important to recognise that Miss K was already showing extreme distress and would be “highly distressed” to emerge from a major operation without her baby. She said outright that “I don’t feel that the discharge planning and care planning is sufficiently detailed to give me comfort”.
Miss K’s wishes
Nobody suggested that Miss K had capacity to make her own decisions about the birth. The judge said there was “very clear evidence” that she could not process information given to her or weigh it up to come to a decision. In accordance with the Mental Capacity Act 2005, therefore the hearing was focussed on making a decision in her best interests, giving weight to her own wishes.
Discerning Miss K’s wishes and feelings turned out to be impossible. This was not for lack of trying in the short time available. The Official Solicitor had sent an agent to the hospital to try to speak to Miss K during the hearing, but she declined to speak to him. Counsel for the OS (Katie Gollop QC) reported back: “She won’t answer questions or engage with him. She was earlier preoccupied with wanting to make a phone call to her father. I think this conversation isn’t going to happen”.
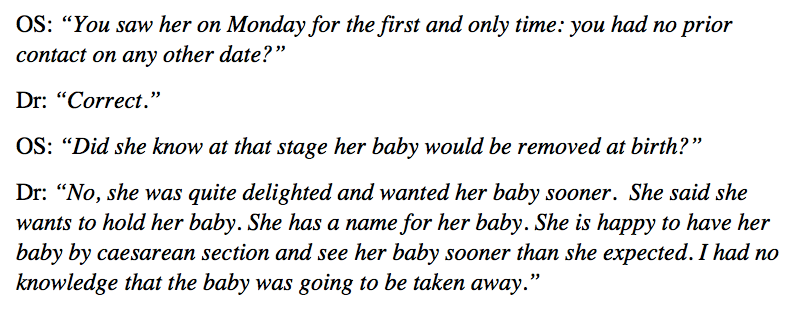
The Court heard from the treating obstetrician, Dr A, that Miss K had said she wanted a Caesarean – and indeed the obstetrician thought she had taken capacitous informed consent for a Caesarean earlier in the week. However, it emerged that the obstetrician either did not know, or did not recall that the baby was to be removed after the birth and had therefore not factored this into her discussions at all:
At this point it became apparent that someone else was in the room with the obstetrician who was giving evidence and he began speaking to her. The Judge immediately intervened asking who he was. He turned out to be from the Hospital’s Litigation and Claims Department. “I can hardly emphasise too strongly,” said the Judge sternly, “how inappropriate it is to speak to a witness who is giving evidence in court”.
The published judgment records the Court’s reaction to Dr A’s evidence:
“… the Official Solicitor was “appalled” at parts of Dr A’s evidence. In particular, the Official Solicitor’s concern, which I share, is that Dr A gave evidence that her view was that Miss K had given capacitous informed consent on Monday to a planned caesarean section, but did so stating that she wanted to hold her baby and keep the baby safe and that she was delighted to give birth sooner rather than later (by having a caesarean section) so that she could hold her baby earlier. This evidence was deeply moving because it had already been decided on 20 May 2021 that the Local Authority would take the baby away at birth. So the true position is that when Miss K comes round from the general anaesthetic, there will be no baby. However, Dr A appears not to have understood this or known it. The Official Solicitor, as I am, is staggered by this as Dr A did not seem to have any understanding of what would happen to the baby following the caesarean section taking place”. (para. 17, University Hospitals Dorset NHS Foundation Trust & Anor v Miss K [2021] EWCOP 40)
Unfortunately, I had to leave before the end of Dr A’s evidence, but what I heard really worried me on many levels. It seemed to reflect a complete failure in multidisciplinary care and planning and also left me uneasy about how the Trusts had approached the need to go to Court for an order.
I gather that, shortly after I left, the Court adjourned for amendments to be made to the care plan. These were discussed before I was able to return – I understand they concerned the use of medication around the period of birth and postnatally. When I re-joined, closing statements were underway.
Closing statements and judgment
At the point at which I re-joined, the Court was reflecting that Miss K had been invited to make a decision about mode of birth on the “wholly false premise” that she would be able to hold her baby – they could not know what she would want had she been informed of the plan at the time she ‘consented’ to a Caesarean. (The Judge did reflect, helpfully for me, that the fact that removal at birth was planned did not mean that Miss K may not be later reunited and able to care for the child.) The Trust had reiterated their position that they wished the court to authorise the Caesarean.
Katie Gollop QC, acting for Miss K via the OS set out what I think is a fairly unusual position of taking no view on what the best interests of Miss K would be. This was because, she said, she had no sense of what Miss K’s wishes and feelings were. The Judge commented that she had looked at the attendance note from the OS’s agent and that there was some evidence that Miss K wanted to protect the baby, and that, therefore presumably wanted the baby birthed safely.
It has to be said that I heard no specific evidence that vaginal birth would not be safe; rather some brief evidence that monitoring labour would be challenging and that waiting for birth would involve further stressful interactions (for staff – whose best interests should not be considered – as well as for Miss K herself). I would have liked to have heard more about the potential to consider whether supporting a vaginal birth may have allowed Miss K more opportunity to be engaged with the “much wanted” pregnancy and baby, and avoid the extreme scenario of being cut open and having her baby removed before she awoke. I would also have liked to have heard evidence from any midwifery support she had received during her maternity care: their experiences of her engagement and interactions over time could play an important part in understanding if and why she was engaging differently with different aspects of her healthcare, and how her views on the pregnancy and wishes about birth had developed over a longer period.
Given the urgency of the case, Mrs Justice Lieven gave an oral ex tempore judgment. The published judgment is now available and closely reflects the oral judgment as I heard it in Court.
She first raised gave concerns about the timing of application – which are worth reading in the judgment if only to sense the extent of the judge’s unhappiness about how this case had come to court. The need for a court hearing in this case could have been foreseen, she said and “it was incumbent upon the Trusts to have made this application significantly earlier”.
“It is wholly unacceptable that NHS Trusts routinely put the Official Solicitor in such a position where she cannot do the job she is instructed to do, and where her role effectively becomes a tick box exercise. This is a waste of resources and wholly unhelpful to P’s best interests.” (para. 4, University Hospitals Dorset NHS Foundation Trust & Anor v Miss K [2021] EWCOP 40)
As an observer, I would have to agree.
The Judge went on to make the observations about Dr A’s evidence earlier in this blog.
In terms of the best interests decision itself, the reasoning was familiar to those of us who follow maternity cases. Mrs Justice Lieven noted that Miss K was “plainly concerned about the safety and best interests of her baby. I have no reason to believe her wishes would be anything other than to have the safest birth possible”. The ruling reflects on the risk of further deterioration in Miss K’s mental health, “continuing with the pregnancy plainly poses some risks to the baby” and that she would be unlikely to cooperate with intrapartum care. “Therefore, allowing her to go through a vaginal birth would be highly risky to her and her baby.” [at para. 19]
Risks could be “minimised” with a Caesarean, and with the care plan now available. “In those circumstances it seems to me to be absolutely clear that a planned caesarean section is a better option”. [at para 22]
Reflections and postscript
Since the hearing, I have thought long and hard about that decision.
I did not envy Mrs Justice Lieven, who herself commented that she did not have the luxury of declining to take a position on best interests. Although I didn’t have the advantage of hearing all the evidence, I am far from convinced that I would have felt better placed to make a best interests decision myself if I had.
I can see why planned care for someone in a highly distressed and deteriorating state is attractive on many fronts. However, like the Court, I really struggle with the sense that there seems to have been no attempt to engage openly and honestly with Miss K, at a time when she may have been better placed to consider her wishes and feelings in an inevitably harrowing situation.
I remain really concerned that it apparently took a Court application to put Miss K’s wellbeing at the centre of the care planning and I wish very much that I had heard what other support – if any – was added to the care plan in the light of the concerns raised. I wondered whether the option of vaginal birth could have been given more consideration in comparison to a surgical birth under general anaesthetic. I worry that the description of a Caesarean as “safest” in the abstract seems to turn on a very narrow – and arguably foetus-focussed view – of what safety means.
We now know from a postscript to the published judgment that Miss K transferred without restraint to the hospital the following day, “met with the clinicians and engaged with them fully and walked into theatre”. When they’re available, the postscripts to such cases often report that the woman in question acquiesced to treatment or complied with clinicians, often contrary to the staff’s prior expectations.
Pre-operative monitoring identified concerns about the foetus at that point, but the baby was born by Caesarean and is now doing well. The postscript does not say how Miss K is doing. I wish I knew.
In the light of this later clinical information – not of course available at the time of the hearing – it seems clearer that Caesarean may have been the better option.
Nonetheless, my disquiet about how Miss K was seen and heard throughout her care remain.
And, as they did last week, my thoughts keep returning to a woman who may have walked into theatre, but who awoke from the operation to find her “much-wanted” baby gone.
Rebecca Brione researches bioethics in relation to pregnancy and birth and tweets @RebeccaBrione. She is also the Research and Partnerships Officer at Birthrights @birthrightsorg. She has written this blog post in a personal capacity.

Thank you for this. It is deeply sad and worrying.
LikeLike