By Jennifer O’Neill, 3rd August 2021
On 27th July 2021 I observed a remote hearing (via Microsoft Teams) brought before Mr Justice Hayden in the Court of Protection: COP 1354439T Re: PH.
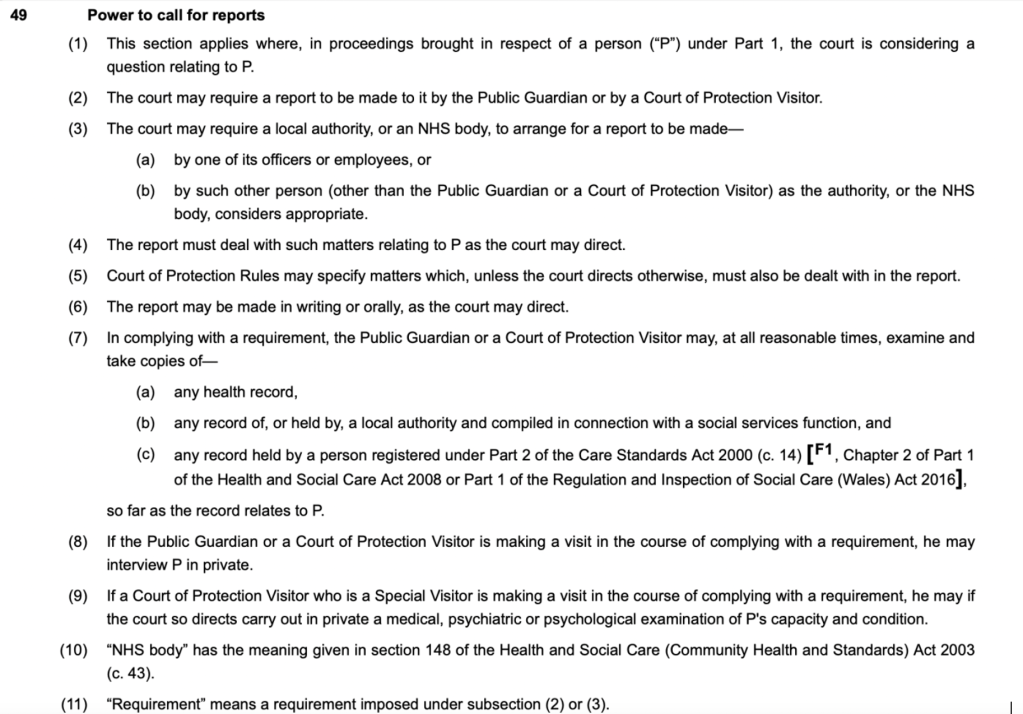
Having observed my first remote hearing in the Court of Protection a few weeks earlier (Re AH COP 13783897), I was aware that when observing such hearings, you never quite know what to expect. On this occasion it quickly became evident that this was a complex case which had already been through several rounds of hearings. Due to the complexity of the case– and the great concern it caused Mr Justice Hayden – there were several interludes during the day as Mr Justice Hayden attended to other pre-existing duties and returned to consult Counsel. During these interludes I sought to familiarise myself with the facts of the case and consulted Gaby Parker’s blog relating to a hearing of the same case on the 29th June 2021.
The hearing of the 27th July was the continuation of a hearing from the previous Friday (23rd July 2021) which I did not attend. Counsel on behalf of the Hospital Board was Roger Hillman and Counsel for PH was Ian Brownhill, via the Official Solicitor.
Background to the case
The case concerned PH, a man in his 40s who was described as having complex physical and mental health needs. The court heard that in 2017, PH had swallowed swimming pool cleaning fluid and, that a specialist team of upper gastrointestinal (GI) surgeons had performed life-saving surgery which included an oesophagectomy, partial gastrectomy, partial colostomy and splenectomy. Although PH had made good progress and was fit for discharge, he had remained in hospital for the past year due to the difficulties in finding a suitable placement in the community. We were told that the case had been adjourned on Friday 23rd July 2021 pending an appointment between PH and the surgical specialist on 5th August 2021.
We heard a short report from the specialist – a consultant upper GI surgeon – who explained that PH’s mental and physical health had been subject to ongoing review to determine whether he had attained the “stage of stability” required to undergo reconstructive surgery of his oesophagus, stomach, and bowel. The court heard that this surgery would remove the need for PH to be fed via a PEG-J tube and would enable PH to live a more normal life. We heard that PH had made good progress thus far and that, in May, his tracheostomy was successfully removed with no need to reinstate it. In her blog, Gaby Parker explained that PH had had “significant communication difficulties as a result of his tracheostomy and [could not] talk” . Since the tracheostomy had been removed “the judge referred to him as ‘blossoming and restored to communication with the world’”. Furthermore, she explained that as a result of hypoxic brain injury – which had been known to further trigger seizures – his cognitive and motor functions had been affected. According to the surgical team, the ‘stability’ required to undergo the surgery required that PH demonstrate abstinence from alcohol and drug use and attain an adequate level of feeding. It was clear that it was crucial PH demonstrated a “good enough presentation” to the surgical team to be considered ready to undergo this “very major” life-changing reconstructive surgery. It appeared that thus far he was moving in the right direction.
Gaby Parker explained that at the June hearing, P had been assessed by a consultant clinical psychologist in late 2020 who had reported that he had ‘Emotionally Unstable Personality Disorder, Impulsive Type’ and he lacked capacity “in a number of respects, including to litigate and to decide on his residence and care – although …in February 2021…did have the capacity to decide whether or not to accept his PEJ feed and the care associated with this”.
The present hearing brought before the Court of Protection related to interim developments which could affect this crucial surgical appointment. Ultimately the court would consider whether it was lawful to hold PH in deprivation of his liberty by consideration of both section 3 Mental Health Act 1983 and the Mental Capacity Act 2005.
Developments in the case
First, we heard that the format of the planned appointment had changed. The surgical team no longer considered it necessary to transport PH from the hospital to the specialist centre to meet the surgeon face to face and so a remote hearing was proposed instead. PH did not require investigations and his weight could be communicated to the team remotely. Mr Hillman, counsel for the Hospital Board, explained that the COVID-19 situation at the referral hospital was acute and that even cancer surgeries had been postponed due to the lack of intensive care unit (ICU) beds. He stated that even if PH attended his scheduled appointment on 5th August, there is no timescale as to when he could feasibly undergo the surgery.
Mr Hillman then explained to the court that since Friday, PH had been removed from the ward where he had spent the last 9 months. Gaby Parker explained in her blog that PH had been isolated in this ward – “[t]here were…systemic, organisational factors at play…[a]s such [PH] was an ‘outlier’ on the ward.” Counsel for the Hospital Board explained that PH had been moved to a psychiatric ward on the same hospital site following an assessment of his behaviour. Mr Hillman stated that “…on a number of occasions [PH has] been upset and frustrated at the progress of matters and had broken computers on the ward. Due to assessment of the safety of staff and others it was deemed that he should be moved to a psychiatric ward for the safety of himself and other patients”. (1) Mr Hillman acknowledged that the move was met with a “very negative reaction” from PH, that he was unsettled and refusing food via his PEG-J tube and that he was described as being “very unhappy there”.
Mr Justice Hayden responded with an expression of deep concern. He clarified that whilst he was in no way “…defending for any moment [PH’s] behaviour [he was] not convinced the damage to computers was linked to psychiatric [factors]…”. PH, Mr Justice Hayden explained, had faced “barrier after barrier” that would have “driven any one of us to despair”. That PH should now find himself in a psychiatric unit because of this was not “immediately and instinctively” considered by Hayden J to be in his best interests. Gabby Parker described in her blog that PH’s “psychological needs appeared to have been … overwhelmingly ignored by mental health provision [and so she] wondered whether [PH’s] complex psychological needs had led to an over-shadowing of his ‘normal’ distress in the face of unwelcome healthcare interventions and his right to have an opinion about these.” She concluded that it appeared that PH was being “silenced in his care, both literally and metaphorically” . Indeed, Mr Justice Hayden toiled with the situation throughout the hearing explaining that he was “not at all surprised” by PH’s reaction in breaking the computers and that to have moved him to a psychiatric ward was “such a pity” considering the progress he had made. He also considered the legal framework which covered PH’s psychiatric admission, explaining that he was not convinced that PH met the criteria for section 3 of the Mental Health Act 1983 and that he was inclined to discharge it.
Mr Justice Hayden proceeded to engage with counsel for the Hospital Board – “Is PH capacious?”. Mr Hillman responded that PH was not, according to the doctor’s assessments from December 2020 and February 2021. Mr Justice Hayden reminded Mr Hillman that we are now in July/ August of 2021. Mr Hillman clarified that PH did not have capacity to decide on his residence, care or treatment.
On several occasions Mr Justice Hayden expressed his concern at the situation, describing the case as a “litany of failure”. The frustration experienced by PH was, according to Hayden “understandable”. Hayden J explained;
“As a result of the system being unable to meet his needs, he finds himself in a psychiatric ward. I am in no way convinced it is in his best interests and I am inclined to remove the order at the expiry of 12 months of not being able to achieve a great deal. He was doing so well… he is [now] not eating, he is distressed, and he is in a psychiatric unit and he is about to be assessed for a surgery for which he needs to be at his best – and he’s at his worst.”
Mr Hillman then responded that there had also been a change of position by the Hospital Board Mr Hillman then responded that there had also been a change of position by the Hospital Board since Friday.The Official Solicitor had recommended an Independent Social Work (ISW) report and an independent nursing report to be carried out and he explained that whilst he had originally been instructed to oppose those reports, he was now instructed to remain neutral. He explained that although the Board had its doubts as to the value of such reports, if the court felt it would be appropriate then the Board would not oppose such a move due to the complicated nature of the case. Mr Justice Hayden responded in exasperation, explaining that he rarely feels that commissioning reports provides answers to such immediate problems.
Mr Brownhill expressed his concern, stating that if PH is in a psychiatric unit, it should be for “the shortest period of time”. Mr Justice Hayden in agreement asserted that “he has waited for 7 months for a place in the community and I am not going to leave him in a psychiatric unit for the next 7 months”. Mr Brownhill then asked Mr Justice Hayden how PH meets the criteria for section 3 of the MHA, to which Hayden J responded that “he does not meet the criteria”. Mr Brownhill proceeded to explain PH’s position – “he is on a psychiatric ward with several elderly people, he says that it “smells like death” and he is becoming upset and agitated”. Mr Justice Hayden, clearly troubled by the developments, responded
“He is not going to stay on that ward. I am prepared to declare it is not in his interests to stay on that ward, but I’d rather work cooperatively and constructively. I do not for a moment seek to justify his loss of temper, but I cannot see but that any of us would be frustrated to have option after option dangled and then withdrawn in the way he has. He has progressed and got better in circumstances that are not capacious to his recovery and all this will be undone by the psychiatric unit.”
Mr Justice Hayden then referred back to Mr Hillman, counsel for the Hospital Board, stating
“I would have thought that the system could do better than that Mr Hillman. I appreciate that people are doing their best, but in the end, one must judge by results and not aspirations. What is the point of him seeing [the reconstructive specialist] at this low ebb which is the result of this placement? It seems to set him up to fail”
In response, Mr Hillman stated that PH has a “complex presentation” which involves an “emotionally unstable personality, of the disruptive type”. However, Hayden J opposed such a defence stating that he does not think such an assessment “correctly characterises the recent past with [PH’s] striking progress…It is [therefore] not satisfactory to say he has an emotionally unstable personality as a banner to march behind to justify the removal to a psychiatric unit. I simply cannot see how that was thought to be necessary or appropriate”. In response, Mr Hillman explained that the move was “as much to do with welfare and safety of PH as welfare and safety of staff and other patients”. Mr Justice Hayden then asked Mr Hillman to point out where, in the court documents, he could find a statement which set out the balance of these issues, quickly clarifying that this was a “polite way of saying I don’t find the balance of welfare and safety” in regard to PH – which served as the basis of the report. Mr Hillman then suggested that the recommendation to move PH to a psychiatric unit would allow his behavioural outbursts to be “better managed”. Explaining that he still remained unconvinced that the criteria for section 3 MHA 1983 were satisfied, Hayden J asked Mr Hillman where, in the context of the law – not medicine – this then left the court.
Deliberation over the relevant legal framework
Mr Hillman explained that PH lacked capacity in relation to treatment and residency and therefore could be deprived of his liberty. The Deprivation of Liberty Safeguards (DoLS) (Schedule A1 is an amendment to the Mental Capacity Act (MCA) 2005 which aims to protect those who cannot consent to their care arrangements whereby those arrangements deprive them of their liberty. Such provision must be necessary and, in the patient’s best interests. However, still unsatisfied, Mr Justice Hayden stated that he considered the detention of PH “for the purposes of treatment is disproportionate and contrary to PH’s best interests”, warning counsel that he has “followed this case all the way through and [is therefore] on top of the evidence”.
Still perturbed, Hayden J turned to Mr Brownhill, “I want to hear PH’s voice”, to which Mr Brownhill responded,
“It is clear PH does not want to continue in the current circumstances. My legal view is that if you came to the conclusion that deprivation of liberty is not authorised, that there would be an ongoing Article 5 [(European Convention on Human Rights – Right to Liberty and Security) breach until resolved in damages. If your Lordship declares that section 3 is unlawful – wearing your administrative court hat…your Lordship may be able to do so in the administrative court on that basis that it is unlawful”
Mr Justice Hayden agreed, “I think it would be difficult for anyone to argue the section 3 criteria are met and so no one could argue it…”. Continuing, Mr Brownhill explained “the Official Solicitor has challenged this for over a month, as to why a case under the MHA 2005 – as opposed to a deprivation of liberty of MCA 2005 – and it appears to be an intention to sidestep your Lordship’s overview”. Hayden J pondered, “the papers are headed under both the COP and MHA – I don’t think they have doubted the jurisdiction of this court. Whilst he has been on the ward, the regime has been somewhat academic but now it is not – it’s very real. I need to hear from Mr Hillman as to whether section 3 MHA can be justified – I think I should hear your submissions after speaking to the psychiatrist”. Mr Justice Hayden then explained “The Supreme Court is looking at the scope of deprivation of liberty with a judgement due to be handed down next Friday regarding children. I am working on the basis that the inherent jurisdiction remains open to the court until the Supreme Court tells me otherwise – if it indeed does – and that I can authorise a placement that is otherwise illegal under the inherent jurisdiction.”
On Friday 30th July the Supreme Court is to hand down a ruling in the landmark case of In the matter of T (A Child)(Appellant) UKSC 2019/0188 on the use of the inherent jurisdiction to authorise children’s placements in unregistered secure accommodation in cases whereby there is insufficient registered places available. In this case, the appellant – a 15 year old child subject to a care order – wishes to be recognised as capable of consenting in law. The case will consider:
- whether it is lawful for the court to exercise its inherent jurisdiction to authorise a child’s placement in unregistered accommodation;
- if so then what legal test should be applied and;
- whether the child’s consent to such deprivation of liberty relevant in the exercise of this inherent jurisdiction.
At this point Mr Justice Hayden then directed the court to return at 11.40, stating he had other duties to attend to.
Upon resuming, Mr Hillman instructed the court that the consultant Liaising Psychiatrist, Dr B, was called as a witness. Having been sworn in, Dr B then addressed the court. Dr B explained to the court that her role was as a Liaising Psychiatrist, providing mental health input in the general hospital whether that be in the emergency department or on the wards. This, she explained, provides a link between mental health and all primary and secondary care physicians.
Mr Justice Hayden was keen to determine the extent of Dr B’s dealings with PH. Dr B explained she had interacted with PH “since his admission”. Hayden J sought further clarification still, “you said you assessed him within weeks of his admission, but have you been seeing him regularly in the interim?” The doctor replied that she “might not have necessarily seen him [herself] but [that she had] been involved in the overall [oversight of] things as the consultant of the liaison team”. Pressing further, Hayden J asked on “how many occasions have you seen him?”. Dr B responded that she couldn’t say, but that it varied between “two to three times a week or once a fortnight or monthly – depending on how he has been”.
Mr Justice Hayden then asked if Dr B had provided the witness statement dated July 15th, to which Dr B replied she had. Mr Justice Hayden asked how PH presents today. Dr B responded that the day before he had walked, with staff, from the general surgery ward to the psychiatric unit. Hayden J then asked why that move was arranged from the ward where he had been for those previous months. Dr B responded,
“PH has been very stable from a physical point of view with minimal intervention from physicians. The only main issue remains his waiting for a placement. Every now and then he gets very frustrated waiting and there were episodes where he would – unprovoked – become very, very aggressive and start throwing things again. And, on a couple of occasions, he broke computers in the secretaries’ office in the ward and it seems to us that, although physically he is much better and he is waiting for the placement – and, his acute needs for both physical and mental health aren’t there – ….we felt that he has been waiting for his placement for many months and it hasn’t come through and it is the psychiatric behaviour that seems to be a big problem when it comes to managing it on a general ward.”
Dr B was then asked to explain the type of patients on the general surgical ward. She explained that, due to COVID, wards are no longer split in to set specialities and that this ward, in particular, now served a range of patients from specialities such as ear, nose and throat (ENT) to medical patients. She explained “it is a mix of skills on that ward”. Mr Justice Hayden then said, “I was under the impression that PH was in a room of his own?” The doctor replied, “yes, he has been in a cubical on his own, but he is able to walk out of his cubical and is on the main entrance to the ward”. She then went on to explain the proximity of PH’s room to the secretary pool and the junior doctor’s office. The ward, we heard, held between 22-23 patients. Mr Hillman then asked the witness whether, with regards to the aforementioned incidents which had occurred, PH would have been able to remain on the general surgery ward. Dr B responded,
“Well, mental health and physical health nurses have different training, and the mental health nurses are far more trained in dealing with behavioural problems with patients and, although those nurses tried their best, they called security and you then have security deal with a patient rather than nursing staff – although our colleagues helped. So, we feel that the psychiatric team is more trained in dealing with the circumstances and we feel this behaviour won’t stop and, from time to time, we will see it”.
Mr Justice Hayden appeared sceptical of this response and asked Dr B – “why, a day before he came to court, was it deemed [necessary] to move him to a psychiatric ward?”. Dr B responded that previously PH was not physically well enough to go to a psychiatric ward, explaining that when he had the tracheostomy this required suction which was not available on mental health wards. Mr Justice Hayden asked Dr B how did she think PH would react to this move, to which Dr B replied
“He was very happy – he said “[he was] mad – take me to psychiatric hospital!”. When we discussed that there was an opportunity and there would be more activities he could participate in, during the day, he was quite inquisitive about the move. It was discussed previously. From 15th July it was discussed with him a couple of times, the move.”
This, it appeared, was in contradiction to the submission of PH’s counsel Mr Brownhill and, as it transpired, the subsequent testimony of PH’s partner – both of whom explained that PH was extremely distressed by the move. Mr Hillman then asked Dr B whether there were any issues, other than dealing with PH’s behaviour, which prompted the move to the psychiatric ward. Dr B explained,
“He has injured staff at times, and he would put other patients at risk – although obviously staff and security try to ensure this will not happen. When he becomes threatening… I have felt threatened and I would have to leave as I knew I would be injured if I didn’t. It wasn’t just about him, it was about the safety of other patients and when he pushed computers on the floor, the secretaries were there and terrified.”
Apparently unconvinced by the necessity for the move, Mr Justice Hayden then asked whether the bed was still available on the General Surgical ward, to which the doctor responded that she didn’t think it was given the acute need for beds. The doctor was then asked how PH was today. She replied,
“Although I haven’t seen him, I am seeing him this afternoon and I have discussed with the team leader that he hasn’t settled well. He refused PEG feeds and has been agitated….I have asked my speciality doctor – who has engaged well with him – [about how he is today]. She reviewed him and he was in the garden of the ward, and they sat and had a chat. He complained there is a smell in the room and in the garden. He also said he didn’t want to take the feed but he was accepting of the medication.”
The doctor was then asked whether PH’s condition was likely to change and whether he would get used to where he had been moved to. Dr B responded,
“This is not unexpected with a condition like PH, to behave this way. It will take some adjustment. I am optimistic that things will move on. The fact the doctor could engage him, and he sat and spoke is good news to me. It is easy for him to access the garden, it is contained, he can’t go outside the ward, but from his room he can go out into the garden, so that is another positive thing for him. Whilst I accept that there are some adjustments to be made…”
Mr Justice Hayden then interjected,
“You know that PH is being assessed by surgeons to evaluate the prospect of major reconstructive upper GI surgery to improve his quality of life – potentially very much – on the 5th of August?”
Dr B replied,
“Yes, I am aware. It was planned a year after 2016. Unfortunately, due to alcoholism and alcoholic hepatitis however, thereafter he has a number of appointments…”
Mr Justice Hayden again interrupted,
“What [the specialist] insisted upon, was that PH be in optimal condition for the assessment. It seems inevitable that to move him before the assessment…it seems incredibly predictable that this would happen. How does that fit with your liaison role?”
In response, Dr B said
“Yes, [the specialist] needs him to be mentally and physically stable. They thought he would be settled in a placement and take it from there. So that’s why it was arranged. At the moment, [the specialist] said there is no point in having the face-to-face appointment. We will probably have it remotely as they will not do any investigations and it is highly unlikely that he will be able to list him for surgery. So, to me, it is much more important that we try and settle PH in a placement to see how he will cope outside, where he will have access to alcohol which he has used in the past and, whether he will be able to continue with the progress so far.”
Mr Justice Hayden then said, “we have spent 12 months trying to find a placement and now he’s ended up in a psychiatric unit. Do you think this is the right place for him?” Dr B said “no, a placement would be right – but when you can’t find it, you choose the least evil”. Clearly perturbed, Mr Justice Hayden hastily responded,
“I don’t think you do, when you are restricting someone’s liberty. That is a long way from meeting their basic human rights. I understand the challenges, but it does not mean I will sanction what you term ‘the least evil’ option. I don’t think that that’s right, that people should have to endure that. I am not prepared to sanction something that is the ‘least evil’ and I don’t think the public would expect me to.”
In regrouping, Hayden J then returned to whether the criteria for section 3 of the MHA 1983 had been met, surmising that “if we get to the bottom of that, then it cuts out a swathe of options”. He asked Mr Hillman, “can you look at, and consider, the recommendation that you made about PH continuing on the section 3 MHA 1983 order, as it has been raised before the court as to whether that is ‘appropriate’ or ‘necessary’ and I would like you to explain [this]?” emphasising that he would like to know whether the criteria are met, today.
Dr B responded that he did meet the criteria as the doctor determined that PH suffers from a mental disorder and, as the result of an acquired brain injury that disorder is more difficult to manage. In considering whether the order is of a degree that is appropriate, Dr B explained that, when one considers the “chronicity” of the disorder, it is evident that he has a long history of behavioural problems that involve self-harm. In describing PH as a “vulnerable adult who will always need care” the doctor explained that he has been “known to surface in mental health [since the age of] 27 when he had a history of multiple drug and alcohol abuse.”
She continued, describing
“the intensity of [PH’s] symptoms – [that he has] a shallow understanding of his care needs, [that] from time to time he finds it difficult to tolerate his frustrations and experiences very negative thoughts. He finds it difficult not to act out, and to dissipate his frustrations in a more mature way. When he ‘comes down’, he is either oblivious or apologies. Is it [therefore] necessary for the health and safety [and] protection of others. Yes, he needs to remain on section 3 of the MHA, as treatment cannot be provided unless under the section. We could say that PH is incapacitated, compliant something – but sometimes he isn’t compliant. He has a degree of restrain that is needed to be used. It is not permissible to use this degree of restrain when he is behaving in certain ways that require restraint. He might not be able to receive treatment if he is under the MCA alone. It takes us back to the original reason why he was put on section 3 in late December. He was originally put on section 2 and then section 3 as he was trying to abscond from the ward, and it was very difficult to control him on the doors alone. To my knowledge, when there is an element of restraint required, we are not justified by keeping them just on the MCA. Whilst I have considered the least restrictive option, I have to use section 3. And, because we have not appealed in the first 6 months and he has a manager’s meeting, where I will meet to defend it again.”
Mr Justice Hayden then inquired, “if the manager maintains the section 3, will it go to tribunal?” to which Dr B responded, “yes, it will go on 9th September and if the managers discharge him from section 3 then we will have to consider an emergency order to keep him on the unit”. Hayden then enquired as to whether PH has tried to abscond, to which Dr B responded that he had tried to abscond from the General Surgical ward, describing how PH had, during a walk around the hospital with staff two weeks ago, tried to “divert towards the shops” and that it had been “difficult to get him back”.
At this point, Mr Justice Hayden had to leave again, and the hearing was set to resume again at 2pm.
Upon his return Mr Justice Hayden expressed frustration at “going round in circles” and conceding that he had “the profound feeling that nothing is going to be achieved at all today and [that he was] very uncomfortable with PH’s situation”. After being advised the PH will go before the mental health tribunal in September, Hayden J concluded,
“I think that PH’s circumstances are very disturbing. He has been waiting for appropriate placement for 12 months. He has been in circumstances that are not meeting his needs. Notwithstanding the lack of neurorehabilitation that he’s been receiving since (as it’s not in the remit of those giving him care), he has made remarkable progress. He has to be evaluated for some very important reconstructive treatment in [such circumstances] when he is – at very best – in the first wave of shock as the result of a dramatic change of circumstances. If you had planned to make it difficult to make progress for PH, then it could not have been more effective”.
Mr Justice Hayden then reminded the court that PH is “a long way off having access to a service his is in need of” and that it makes him “very concerned for those who do not have the degree of scrutiny this case has [and all the protection afforded by the Court of Protection]”. Hayden J then explained that he had met with PH’s partner, whom he noticed was in attendance at this hearing, as she had been at every prior hearing. He explained that whilst he was not prepared to allow this situation to continue, he was unsure of what he could do today. He contemplated that he could make a public order, and “name names” but that that was the “weapon of last resort”. Whilst acknowledging that in the current pandemic, we are “all under pressure”, he cautioned that “that does not mean people like PH can get lost in it”.
Concerning the Lack of Suitable Placement
Mr Justice Hayden then turned to address Mr Hillman, Counsel for the Hospital Board – “last time you had told me there are places in the community that PH might be able to go to because he’s made sufficient progress…because he’d made [that] progress under his own steam. Is that still an option?”
Mr Hillman explained that those were mental health nursing homes and that those applications have not been progressed because there have been COVID outbreaks which means they had not been able to assess him. He sought to assure Hayden J that PH would be assessed “as soon as the COVID situation allows”. Mr Justice Hayden was wholly unsatisfied with this response replying,
“I am not prepared to accept that is sufficiently proactive or creative enough. About 12 months ago we moved to assess people in care homes remotely and that has proved quite effective. I know it’s a preliminary assessment [by the specialist surgeons] that will take place remotely – why can’t the assessment for the nursing home be done remotely since there is a [body] of evidence available [from this case]?”
Hayden J was not prepared to accept Mr Hillman’s explanation that this was the nursing homes’ position, stating that nursing home representatives can “come and tell me why they are taking this stance in person”. Mr Justice Hayden continued to emphasise the urgency in this case, stating “we cannot have this drift. He has been in these parlous circumstances for too long now and I want to know what can be done and quickly. I want to know what we can actually do and not what we can’t do. Dr B – what can we do, because this can’t be right?”. Dr B asked, “if I took this right [you are stating that] we are depriving him of something that would benefit his physical health?”. Hayden J replied,
“No, he’s recently been moved. He’s been distressed at the move. The distress is predictable and it’s at the time when he’s being assessed for major surgery and he’s not going to give off his best – that to me does not seem like the most coordinated approach. PH should not be where he is now and he’s been there long enough.”
Dr B then responded “PH is where he is because of what he did to himself”, to which Hayden J crossly replied “I do not take that view. The Court of Protection does not take a punitive view. I am talking about the overwhelming gamut of his needs which are, on your view, the least evil”. The doctor then responded that if there was a placement available which was appropriate then that is where she would have liked PH to go. Hayden then turned to Counsel for PH, Mr Brownhill to ask his perspective. Mr Brownhill explained his frustrations, reminding his Lordship that he had set out a roadmap at the last hearing which represented a “comprehensive assessment of need” and which had recommended that a “commissioning specification” be set up. Mr Brownhill explained that this required a search of England and Wales be conducted to find potential placements and that, once complete doctors would be invited to put forward their views according to section 4(7). This, according to Mr Brownhill, did not happen and he held the Health Board responsible for this failing. He explained “…there is no explanation as to why that is not done. With some regret, the independent social worker and nursing expert are [now] instructed to do the work that should have been done today”. Hayden J requested a list of options be drawn up which could assess PH remotely, but Mr Brownhill reminded his Lordship that this was requested at a previous hearing but had remained unfulfilled. Mr Justice Hayden then turned to Mr Hillman and asked “am I being ignored?”. Mr Hillman advised Hayden J that “the problems have come about [because] we have been given the ‘run around’…for COVID reasons things have been put on hold temporarily”. This was not considered to be an acceptable excuse before the court according to Hayden J,
“Unless you have been living in a parallel universe you will know that the entire world has managed to make assessments remotely …to say we can’t do things because of covid is invariably a ruse for those who don’t want to do things. You only need to look to the law reports and see what has been achieved in care homes and hospitals and ICUs. This man has, on the preponderant medical evidence, some potential to recover – even without focused treatment, and in a state of limbo, has managed to do well. Dr B feels she is being criticised but, the reality is that he has been moved when he didn’t need to be removed”.
In reference to an earlier argument by Dr B that PH would also be exposed to nosocomial infections if he were to remain on the general ward, Mr Justice Hayden continued –“to say there are viruses fails to recognise he has been on the ward for 12 months running the gauntlet of avoiding these viruses.” Counsel for the Health Board, Mr Hillman then replied by stating that “maters are not going to resolve suddenly” when PH meets the surgical specialists. Hayden J responded, “I don’t like that – trivialising the meeting with the experts – I suspect to him it is very important.” Whilst Mr Hillman clarified that he did not intend to trivialise matters, and that it was unlikely surgery soon take place due to COVID, Hayden J explained “I am extremely uncomfortable at what has happened, and I am, by no means persuaded that he should be under a MHA order, but since it will be reviewed by tribunal soon, I am not going to quash it by way of judicial review now. [Nonetheless], I want this to be proactive and I don’t want PH to be side-lined”.
Mr Brownhill then addressed the court, citing his concern that key members of the Health Board failed to attend any of the hearings. He described the whole process like trying to “get blood from a stone”. He commended his Learned Friend as “valiant in defending the Health Board” but explained that the reality was his client was “sat on a bench outside a psychiatric unit” just now and that “if it gets worse, he will end up in a psychiatric intensive care unit”. Appealing to Hayden J, Mr Brownhill explained “someone of rank needs to listen to your Lordship. I would prefer the Chief Executive had been here to listen to what you say”. Hayden J agreed that Mr Hillman had “not [been] given what he needed [and so] ends up in a defensive position for the Health Board and [that] that is not what this court is about”. Hayden J then stated that he would sit in open court at the end of August, that he will review the need for a transparency order if need be and will give a judgement at that time. He requested that he be informed of who to call at that time, and explained that he has “tried all other routes” and that he “does not take this [stance] lightly”. He explained that he hoped this approach would “generate a more proactive, not aggressive, resolve to do something for this still young man who is only [in his 40s]”. Hayden J then turned to Dr B,
“This is not about criticising the individual doctors. It is about getting the system to work effectively to translate the care into the result. I think you are right to use the least evil option. We have hung on for 7 months for a placement that “gave the Board the run around”, but it shouldn’t have been permitted to do so as there is a patient at the middle of it. Either they are going to do so, or you should have abandoned ship”
Mr Brownhill then restated that PH was currently sat in the gardens of the psychiatric unit over lunchtime, indicating that he should not be there. Mr Justice Hayden then considered that “one of the few consolations [of holding remote hearings], is that P – the protected person – has been more involved than they would have before [the COVID pandemic]”. This, in reference to the newfound ability to interact with protected persons via remote video link. He continued,
“I visited P and you will recall that he found that a beneficial experience. Not because I was able to convey anything constructive, but because he was not made to feel a bystander. So, I want a careful note of what he has to say about his circumstances. I do hope that when we meet in August, finally, there will be some good news about this man. My own assessment of him – and I don’t doubt that he is in this position due to his own actions, but he does have a personality disorder which contributed to that – [is that] he has made considerable effort in recent times. I hope that we can do something for him.”
Mr Hillman then asked what “physical steps are expected to be progressed…?” to which Hayden J clarified,
“Let me help and this is not to circumscribe you to my views. I want to know:
- who is responsible for looking for a place – their name and who they are accountable to
- A list of every place the approach
- What the response is
- The reason for their response.
- Whether it is possible for remote assessment
- I want the emails
- I want the whole telephone and paper trail, so I can get a grip of the reality.
This is what I would do for a child, when children need secure placements and can’t get it. I get a named individual to go around units. It can create a degree of urgency that doesn’t seem to arise under the burden of people’s day to day routine, which I know for all of us is heavy at the moment.”
Finally, Hayden J turned to PH’s partner, who explained that PH had, even prior to the hearing commencing at 10.30am had contacted her 30 times. This was, in her opinion, illustrative of his distress at this psychiatric placement. In closing, Mr Justice Hayden sought to reassure her, “I am hovering over this case for as long as I have to…[and] until we are able to galvanise the system into [doing] something”.
A provisional date for the hearing in late August will be set by Mr Justice Hayden’s clerk.
Reflections
This was a sad and uncomfortable case concerning a relatively young man who, in the midst of legal wrangling and the inability to secure accommodation during the COVID pandemic, found himself referred to the care of a psychiatric unit.
Of upmost concern was that a crucial chance to demonstrate his progress, and be deemed eligible for life-changing surgery, could be undermined by this move – a move which the judge considered to be the result of frustrations borne of the barriers continually placed in PH’s road to full recovery and discharge.
Mr Justice Hayden demonstrated compassion and the upmost concern throughout the hearing.
Whilst it is disheartening that action was not taken on this day, given Mr Justice Hayden’s comments, it appears unlikely that the situation will be allowed to continue as is, following the subsequent hearing at the end of August.
During the hearing, Mr Justice Hayden commented that this was a rare occasion when the distinction between two similar legal provisions – often considered to be purely academic in nature – represented materially different outcomes for P.
For the past four years I have been a lecturer and coordinator of the Legal Medicine and Clinical Bioethics programme at European University Cyprus Medical School. In holding this position, I have sought to bridge the gap between medical practice and legal theory so that our fifth year MD medical students are equipped for their future medical practice. Whilst I was already familiar with the relevant legislative provisions held under the MHA 1983 and the MCA 2005, this was the first time I had considered, in depth, the potential implications which could arise from either provision. It therefore demonstrated the importance of clarifying which provision was necessary in the given circumstances.
Following this hearing, I intend to engage my students on this matter in the coming academic year, so that consideration is given as to when it may be appropriate and necessary to hold P in deprivation of liberty and, where this is established to be the case, that careful consideration then be given to whether the provisions of MHA 1983 or MCA 2005 are most suitable. This, I hope, will allow greater appreciation as to the impact that such “academic” distinctions may have upon the outcome for P – who is, after all, at the centre of it all.
I appreciate that facilitating public access to these hearings creates an additional workload on Court staff during an already very difficult time – they must reply to emails seeking access, provide access links, note the names, and email addresses of public observers, send out transparency orders and may even assist on fact checking for blogs such as this. I am truly grateful for the opportunity to observe, and I consider such access to be an invaluable part of professional development.
I hope that as restrictions end, remote access will continue to some extent. At both hearings I have attended, Mr Justice Hayden has commented favourably on how remote access has placed P more centrally at the heart of such proceedings, enabling the judge to interact with P via remote links and ensure their voice is heard. Remote access also has great academic value, enabling access for those – such as myself – who would not normally be able to visit the High Court in person. In observing these hearings, legal theory itself transcends from the ‘academic’ into ‘reality’ in a way which inevitably stimulates greater academic curiosity, promotes research, and influences teaching. In this way, remote access, arguably benefits future legal and medical practitioners by proxy and so, will hopefully, improve outcomes for future protected parties.
Jennifer O’Neill is a Lecturer in Anatomy at the University of Glasgow and visiting collaborator at European University Cyprus. She tweets @j_o_neill_
(1) Audio- and video-recording of COP hearings is strictly forbidden, so the quotations presented in this blog are the result of type-written notes which aim to reflect as far as possible what was said, but are unlikely to be word-perfect.
Photo by Kyre Song on Unsplash