The hearing I observed (COP 13977140, listed for 12 noon on 18 September 2023 before HHJ Spinks sitting in Cambridge County Court) was a “final” hearing to last for two days, with the issue before the court being “Discharge/conduct of deputy or attorney, application by Public Guardian”.
Committing to a two-day hearing was a first for me. My previous observations have usually been no more than a couple of hours, often much shorter, being mainly “directions” hearings. I’m not sure I would want to do it again!
When I saw the details, as listed by the Open Justice Court of Protection Project on Twitter/X, I knew immediately it was probably the case I had been waiting for and I felt I had no option.
There are very few hearings involving the Public Guardian, they are seldom open to observers and, when they are, they are usually in person with no remote access for observers. At the last one I observed, the OPG representative expressed surprise and dismay at my presence because he had thought the hearing was private (I blogged about it here). On this occasion I overheard a conversation – I think between the OPG barrister and the OPG investigator – to the same effect.
With this background, I was agreeably surprised when I asked for a copy of the OPG’s position statement and, after a few days, received it from their very helpful barrister. By that time, I had already drafted this blog post, so it was interesting to see the discrepancies between it and my understanding of the case based only on what I heard in court. Because the respondents were not represented, there was no way that I could ask for their position statements – so I now have a slightly lop-sided perspective, which was not the case during the hearing. I have made a few revisions as a result but tried to keep more or less to what I actually heard. Interestingly, the position statement shows that this was originally intended to be yet another “attended hearing” (i.e. in person). I don’t know what caused the change, but it was possibly to accommodate the OPG investigator, who attended remotely.
My special interest in the OPG is in relation to property and financial affairs and stems from the very poor treatment to which I was subjected when I was acting as COP deputy for my mother’s affairs. In particular, after my first annual report, they insisted that I pay back a gift that I had made and, when I refused, threatened me with a range of consequences, including taking me to court to remove me as deputy. I was very keen to go to court because I doubt the legal grounds on which the OPG makes its decisions and welcomed the opportunity to obtain some transparency. It didn’t happen because my mother died and, anyway, it appears from a Freedom of Information request I made that such threats are seldom carried through.
This case concerned an attorney rather than a deputy and I imagine that there are more cases involving attorneys (compared with deputies) because – unlike the situation with deputies – the initial process of becoming an attorney involves very few checks. I sensed that the situation was similar to mine, however, in that the attorney believed that her actions were in keeping with her legal responsibilities and also that the OPG’s administration was badly flawed. Furthermore, she felt that she was being defamed by their accusations and that their behaviour towards her lacked understanding and humanity. She had clearly put her heart into preparing for the hearing, as demonstrated by the fact that she had produced over 300 pages of evidence and claimed to have spent £900 on photocopying. (The entire “bundle” of evidence before the court totalled over 1000 pages!) She represented herself, possibly influenced by the cost of employing a lawyer but I think also because she was so sure she was in the right and that the truth would prevail. Like most people in her position, she had no idea how the judge would expect the hearing to be conducted.
Joining the hearing
I received the link from the Cambridge court at 9.15 on the Monday morning (impressive!) with the heading ‘URGENT HEARING 18th September 2023 at 10:30AM’. I duly opened the link at 10.20 and waited… An hour later I rang the Reading hub to see what was happening but they still had the start time as 12 noon (as per the listing). Sometime after noon, the hearing did in fact commence. It was, I think, only my second experience of a hearing where most of the participants were present in the courtroom.
Present remotely were myself and the OPG investigator. (For information about OPG investigations, check out “How we do investigations at OPG”.)
Present in the physical courtroom were: His Honour Judge Spinks Mr Alex Cisneros representing the Public Guardian as applicant First respondent, one of P’s two sons and a co-attorney (A) Second respondent, P’s only daughter and a co-attorney (B) Third respondent, P’s other son and a co-attorney (C)
None of the respondents was represented.
The camera was managed extremely well so that the witnesses were in view when giving evidence and the judge was in view at least some of the time when he was addressing the court. For some reason the OPG barrister was almost never in view – possibly due to logistics. I only found out his name when I emailed Celia with what turned out to be a poor attempt at a phonetic version!
The case
The way the hearing was listed was a little vague but it was, in fact, to consider the discharge of all three respondents from their roles as attorneys for both property and financial affairs and health and welfare for their mother, P. The three siblings held their attorney roles both jointly and severally and the OPG sought to replace them with a professional Court of Protection deputy for property and financial affairs, leaving the role of attorney for health and welfare unfilled. This was explained to me by Mr Cisneros at the start of the hearing at the Judge’s request. I had to work out the rest for myself!
It transpired as the hearing progressed that Son A had, in the beginning, been in accord with his sister as to the use of their parents’ assets (they were attorneys for both their father and their mother, but their father had died by the time this investigation began). He had agreed that in reality she would be the only one accessing their accounts because she was the only one looking after them on a day-to-day basis, including eventually moving in with them to give 24-hour a day care. He did have access to P’s bank statements, however, and eventually became concerned by some of the transactions. He had failed to get his sister to engage with his concerns and, as a result, had contacted the OPG.
To avoid paying a professional deputy, Son A had volunteered to be appointed sole attorney; this would be a separate decision once the existing arrangements were revoked, which is why at this stage he was a respondent and not an applicant. (Son C took no significant part in the proceedings except to express his support for his sister.)
I presume that what came next is standard procedure. The OPG started an investigation, putting the powers of attorney into abeyance and appointing an interim professional Court of Protection deputy for property and financial affairs. The investigation included asking for records of all expenditure, which B had provided in what appeared to be meticulous detail, going back some ten years. Since the OPG only ask attorneys to provide records of their activities in exceptional cases I would be very surprised if many attorneys have kept such detailed records, although it is clear that they are expected to do so.
The OPG investigator acknowledged that B had been very open during the investigation but said that some of her explanations had become “confused and changed slightly”. He had had no contact with the other two attorneys.
The evidence
The judge said that it would be impossible to go through all the evidence in the time allotted and that, although the OPG were not currently considering requesting that costs be awarded against the respondents, their position might change if resolution could not be achieved in two days. He suggested that the court concentrate on some of the major items of expenditure. He pointed out that the OPG were not requesting repayment of the money B was accused of spending inappropriately (a total of over £80,000 was later mentioned in this context) so she did not have to justify every item. (I don’t know why the OPG were not asking for repayment because they did in my case; I suppose that could come at a later stage, but the judge didn’t in any way suggest it as a possibility.)
B was not happy with this arrangement and, although the OPG’s barrister started off as instructed, a considerable amount of time was in fact spent talking about minor as well as major items. B was clearly very angry that the work and the care that she had put into looking after her parents had been, as she saw it, completely disregarded and that questions were being asked about such things as who paid the bill if they went into a café together. So, the discussion ranged from bills of less than £10 through to the cost of purchasing a car. There was also some time spent on a sum of £10,000 that the OPG initially said was unaccounted for, but then admitted was a transfer between accounts.
B was particularly exercised by the terminology “issues of concern” on the OPG spreadsheet and did not seem reassured when the OPG investigator said that this was simply his way of signifying things that needed to be looked at further.
The issue of capacity
This was an interesting area. Questions were raised as to when decisions were made; whether they were made by B or by her parents; were they before or after P lost capacity; and what capacity had been lost and what retained on each occasion? The power of attorney had been registered with the parents’ bank well before P lost capacity to manage her money, and B claimed that P’s capacity was, in any case, variable. Even after she had been medically assessed as being unable to make “financial decisions of complexity”, she was still capable of making choices as to how she wanted to spend her money. B said that her father had always managed the couple’s finances and they had never had bank or credit cards.
An underlying issue?
Some of the questions put to B concerned very large amounts of cash that she had taken from her parents’ bank accounts and kept at home. The OPG said she had talked about trying to avoid care costs (P was now in a care home) and she strongly refuted this, given that P was the sole owner of a house of considerable value. She said that her father had always kept large sums of cash and felt more secure being able to see it rather than having it in the bank. This made some sense given his declining faculties, including eyesight. However, it isn’t hard to imagine that B might have preferred to safeguard a certain amount of cash so that it would not be taken into account when, before the house was sold, the Local Authority made its initial financial assessment. The position statement shows that the Local Authority were now paying care home fees due to depletion of assets. B knew that she would have to repay the debt later but, in such circumstances, liquidity can be a real problem.
The judgment: A pragmatic decision
Looking at the government website, it seems to me that the duties of an attorney, as opposed to the duties of a deputy, are not closely defined and certainly there was no attempt at this hearing to come to a decision about whether or not B had contravened them on any particular occasion. In the end, just as the court was set to rise on the second day, the judge managed to pluck agreement out of nowhere, as far as I could see, although I might have lost some concentration! All three attorneys agreed that, whatever the rights or wrongs of B’s actions, because the relationship between them was irretrievably broken, they were incapable of continuing. Son A withdrew his request to act as sole deputy for the same reason. The judge ordered that a professional deputy should be appointed.
All three siblings agreed that they could still continue to act together as P’s attorneys for health and welfare and the OPG accepted that on the grounds that there were no immediate decisions to be made now that P was reliant on the Local Authority for care home provision.
B’s day in court
Despite unhappily agreeing to the decision, B continued to express her disappointment at the way things had turned out. She had wanted to clear her name and felt that that had not been achieved. She asked about making a complaint about the OPG and the judge said he was sure there must be a complaints procedure. I did so want to tell her not to bother; I have been through all that, including trying to take my case to the Ombudsman, and it doesn’t work.
Afterword
According to the blurb for a forthcoming book, Powers of Attorney for Property and Finance: A user’s guide by Ann Stanyer, more than six million powers of attorney are now registered in England and Wales and it does seem to me that it is an area potentially fraught with difficulty, with far too little general knowledge or detailed guidance. I am hoping the book will fill this important gap.
By Celia Kitzinger, with Brian Farmer, 24 September 2023
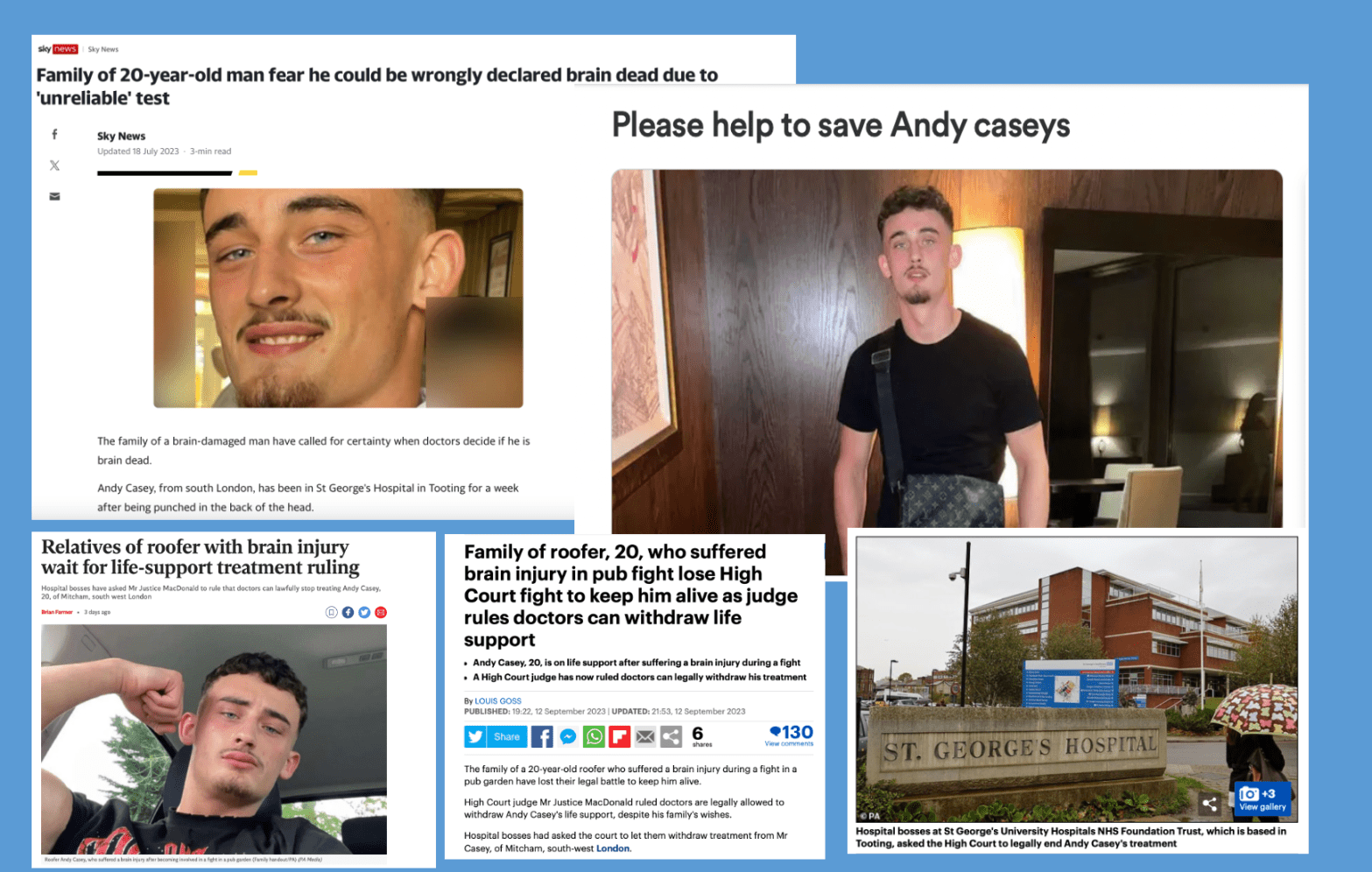
On 9th July 2023, Andy Casey – then a healthy young man – was on a night out when he was assaulted in a pub garden. He was punched on the right side of his head and fell to the ground, with catastrophic injury to his brain. An ambulance took him to St George’s Hospital where, from the point of admission, he was found to be in the deepest form of coma, and four days later his treating clinicians suspected that his brain stem had died. This was subsequently confirmed by formal brain stem testing. This meant he met the legal definition for death in England.
Normally, withdrawal of organ support follows within 24-48 hours of the clinical diagnosis of brain stem death. In this case, though, the family did not accept the results of the tests and reported seeing Andy move in ways that they considered indicated that he was not brain stem dead. An attempt at mediation failed, and the Trust made an application to the Family Court for a declaration that Andy Casey was dead, and that therefore organ support could be lawfully withdrawn.
The judge heard evidence from the family and from clinicians and concluded that “Mr Casey died on 16 July 2023 at 11.51pm” (i.e., when brain stem testing confirmed his death). He further declared that: “in the circumstances, it is lawful for a consultant or other medical professional at the hospital part of the St George’s University Hospitals NHS Foundation Trust to (a) cease to mechanically ventilate and/or to support the respiration of Andrew Casey, (b) to extubate Andrew Casey, (c) cease the administration of medication to Andrew Casey and (d) not attempt any cardio or pulmonary resuscitation upon Andrew Casey when respiration and cardiac output ceases” (§79 and §81(ii) St George’s University Hospitals NHS Foundation Trust v Casey [2023]EWHC 2244 (Fam)).
This sad story has been widely reported in the media as the case has unfolded – and Andy Casey’s name, and those of his family members, as well as the name of the hospital where he was being treated, have been included in these reports from the outset. Here’s an example from Sky News.
The family of a brain-damaged man have called for certainty when doctors decide if he is brain dead.
Andy Casey, from south London, has been in St George’s Hospital in Tooting for a week after being punched in the back of the head.
The 20-year-old’s family say doctors treating him at the hospital want to do a brain stem test to assess whether he is brain dead before removing life support.
The family oppose the test, citing questions over its reliability after two recent cases where the test was used to wrongly declare living people as dead.
Mr Casey’s mother Samantha Johnson told Sky News the test is “not 100% accurate”.
She said: “If they do this test and it comes back zero activity, they can turn off the machine … it’s not a 100% accurate test so there could be a chance that my son could pull through this.
“I believe my son is fighting. He needs this chance and I’m going to fight no matter what.”
The names of the family, and the Trust and the hospital are used throughout reporting of this case and are also used in the final judgment.
This is unusual – both in the Family Court and in the Court of Protection – and this blog post describes how this came about.
It’s an interesting case to consider for families who don’t want reporting restrictions in relation to their own cases in the Family Court or the Court of Protection.
It’s sometimes claimed that the Family Court and the Court of Protection are operating in secret, imposing “draconian” reporting restrictions which prevent families from speaking out about court cases in which they are involved.
Of course, many – perhaps most – families involved in these court hearings do not want their stories in the Daily Mail. But some do, especially when they believe that injustice is being done, or that the life of their relative is at stake. There may be lessons here for families who want to speak out.
Reporting Restrictions Order: 23 August 2023
Initially, there were reporting restrictions in place preventing identification of the Trust, Andy himself and Andy’s mother. Observers were sent the Order approved by Mr Justice Moor on 23rd August 2023.
3. For the purposes of these proceedings:
a. The Claimant shall be referred to as “A Hospital Trust”;
b. The Person the case relates to shall be referred to as “A”;
c. The Defendant (A’s mother) shall be referred to as “B”.
Publishing Restrictions
4. This Order prohibits the publishing or broadcasting in any newspaper, magazine, public computer network, internet site, social network or media including Twitter or Facebook, sound or television broadcast or cable or satellite programme service of any information (including any photograph, name and/or address) that is likely to lead to the identification of any of the following;
a. A, who is the subject of these proceedings; or
b. Any member of A’s family, including B; or
c. The name of the Applicant NHS Trust;
d. Any of A’s treating clinicians (clinical and non-clinical), including those who have taken a part in or been referred to in these proceedings.
IF, BUT ONLY IF, such publication is likely to lead to the identification of A as being the person receiving treatment or as a party to these proceedings, whether such identification be to the public at large or to those who know A, or have encountered A as a fellow patient or being a party to these proceedings.
Reporting Restriction Order, 23 August 2023
The problem with this Order was that by the time it was issued (in August 2023) there had already been media reports (and a fund-raising page) naming Andy, his family members, and the hospital (though not his treating clinicians) in ways that make it easy to connect them with these legal proceedings. They include the Sky News report quoted above, which was published in July 2023.
Varying the Reporting Restriction Order: 8 September 2023
Both the Official Solicitor (Emma Sutton KC, acting as Advocate to the Court) and Brian Farmer – as the journalist covering the hearing – drew the judge’s attention to the fact that the information prohibited by the reporting restriction order (RRO) was already in the public domain.
The Official Solicitor said, that “reconsideration of the terms of the RRO is likely to be needed at the outset of the hearing” – comparing it to an earlier case in the Court of Protection concerning William Verden (Manchester University NHS Foundation Trust v William Verden (by his litigation friend, the Official Solicitor) & Ors [2022] EWCOP4 (see §§9-11 in particular), where there had also been lots of media publicity before the case reached court.
Brian Farmer (journalist with the Press Association) wrote to the judge as follows:
Dear Judge
1: I can see from the Alerts Service explanatory note that this case is a little unusual because Mr Casey’s mother appears to have disengaged.
2: However, the problem from the media’s point of view is a familiar one.
3: There has been publicity about Mr Casey’s case (names have been named) and the publicity has indicated that litigation is likely if not underway.
4: We’d want to be able to report developments and finish the story. Those developments (and probably the end of the story) will be outlined to you in court.
5: This is the jigsaw identification problem with which everyone in the Family Division is so familiar: names have already been named, how do we end the story if we can’t name Mr Casey or the Trust in court reports?
6: Anonymous reporting won’t work: outlining the facts without names will create the simplest identification jigsaw.
7: There are obvious public interest issues:
i)We ought to be able to report court hearings, even private hearings.
ii)We ought to be able tell people about the consequences of violence (and here I’d make the well-known, “what’s in a name… a lot press would say” (1) point).
iii)We ought to be able to report the issues that arise, and the difficulties doctors, families, and judges face, in these kinds of cases.
8: You’ll obviously have to balance [Articles] 10 and 8 but I’m not sure whose 8 rights you are protecting. Realistically, ending the story isn’t going to undermine Mr Casey’s 8 rights; they’ve already been undermined by reporting. I would make a similar argument in relation to Mr Casey’s mother and family.
9: We’d say you shouldn’t impose a blanket ban on reporting. (We’d then ask if we could report the ban and make “secret justice” arguments.)
10: These problems have been solved many times before in a series of treatment cases (Gard, Evans, Battersbee etc). We’d say you should let us name the names which have been already named – just as judges did in Gard, Evans, Battersbee etc.
Email from Brian Farmer sent to Mr Justice MacDonald
The parties’ positions
The position of the Trust – represented by Abid Mahmood – was that the reporting restrictions should continue, despite publication of some of the case details.
“It is not necessarily the position that persons will be able to link the previous reports in the media to this case when it appears on Bailii or the like”, he argued.
The Trust’s motive for retaining the reporting restrictions was clearly to protect staff.
Counsel referred to a message sent by Christine Casey via Facebook on 14 July 2023 inviting the public to attend the hospital to protest: “…if it says 0% then there turning his machines off so now we need as many people as possible to come up after the test to protest to make sure his machine don’t get turned off please share this status”. And since then (he said), a covert recording device was found in P’s room – designed to look like an air freshener with a device for recording at the back.
In their skeleton argument, the Trust acknowledged that “the family deny any connection to it [the covert recording device]” but added “it is obvious that the Hospital staff are employees who need to be able to get on with their work. Hospitals are always stressful and difficult places even without complications with protests and covert recording devices. The Trust owes duty to its staff.”
The Trust quoted the judgment in a Court of Appeal case (which also concerned a case of “brain death”):
“The manner in which social media may now be deployed to name and pillory an individual is well established and the experience of the clinicians treating child patients in cases which achieve publicity, such as those of Charlie Gard and Alfie Evans, demonstrate the highly adverse impact becoming the focus of a media storm may have on treating clinicians. The need for openness and transparency in these difficult, important and, often, controversial cases is critical but can, in the judgment of the court, be more than adequately met through the court’s judgments without the need for identifying those who have cared for Midrar…” (§102, Re M (Declaration of Death of Child)[2020] EWCA Civ)
Judge: I’m sorry to interrupt, but none of those actions would be restricted by a reporting restriction on the name of the Trust. Family already know it. Friends know it. And members of public know it. An Order preventing reporting of the name of the Trust wouldn’t prevent that mischief.
Counsel for Trust: If members of public want to, it would really be only a simple step to put into search engine the name of the Trust and locate the names of the treating clinicians. We propose that the Trust be referred to as “a London Hospital Trust”
Judge: The horse has bolted, Mr Mahmood. The name of the Trust is already out there. […] I really struggle with the idea that in circumstances where the name of Trust is already in the public domain, I should artificially restrict it. Ms Sutton – […] do you have any submission?
Official Solicitor: Yes, it’s straightforward. The family want to speak out. The only issue is that the clinicians are appropriately anonymised….
The judge checked that the family’s legal representatives (James Bogle and Paul Diamond) also supported relaxing the reporting restrictions. They did.
Decision on reporting restrictions
The judge said he was “entirely satisfied” that the Order should be varied to allow “naming of Andy and identification of the Trust”.
The Official Solicitor checked that the intention was that the Order would also permit naming Andy’s mother, the first respondent – albeit that she was not in court today – Samantha Johnson; and his siblings, seeking to join as third and fourth respondents, Christine Casey and Joe Casey. “Yes”, said the judge.
In his judgment, Mr Justice MacDonald names all of these people – and more (Joe Casey’s partner, Macy Jo Phelan, who gave oral evidence in court), as well as naming the Trust and the hospital. He refers briefly to the reporting restrictions in §5 of his judgment:
“… the court determined that it was appropriate to relax the terms of the Reporting Restriction Order (RRO) to permit the naming of Mr Casey and the identification of members of the family and to permit the naming of the Trust and the hospital. Both these steps were taken in circumstances where those details were already in the public domain as the result of coverage in the press. I was not prepared to relax the current restrictions on publishing the names of the treating clinicians involved in this case.”
§5 St George’s University Hospitals NHS Foundation Trust v Casey [2023]EWHC 2244 (Fam)).
Reflections
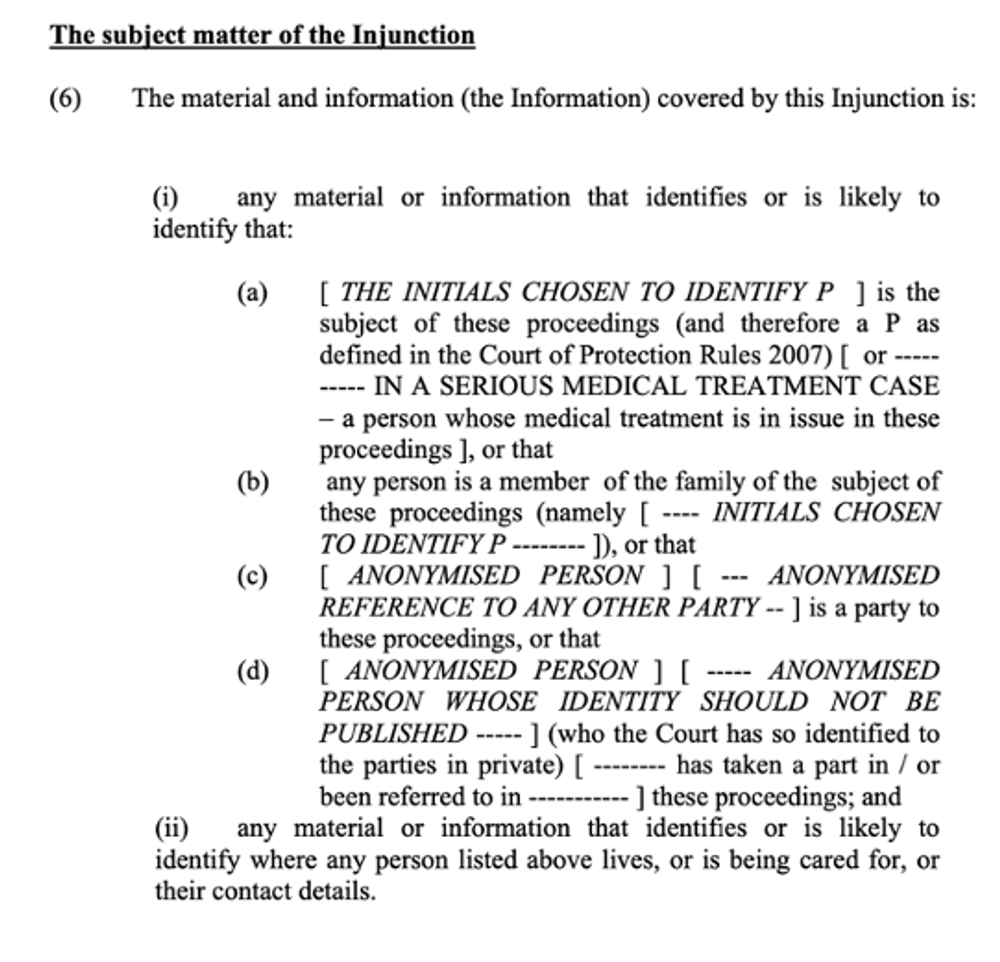
“Reporting Restriction Orders” (RROs, in the Family Court) and “Transparency Orders” (TOs, in the Court of Protection) raise difficulties for family members who want to speak out about their court case. They’re often made without the family really understanding what they mean, or knowing how to ask for them to be changed.
As I’ve said previously, these reporting restrictions, “[impact] upon their [families’] freedom of expression more severely than it does observers , because in speaking about (for example) “my son” or “my mother”, under their own name, in connection with a COP hearing, they are “likely to identify” that person as a P in the Court of Protection”.
32. Many of the families I’ve supported through serious medical treatment cases find themselves angry about being “silenced” or “gagged”. They have come to believe that the TO protects clinicians, not P. Some of the family members who’ve contacted me through the Open Justice Court of Protection Project say similarly that the court is attempting to silence them because of their criticisms of the healthcare or legal systems. Reporting restrictions are viewed as damaging P, not protecting them. Most have not, in fact, been willing to challenge reporting restrictions – believing it will be another expensive court battle, or that they are bound to lose anyway, or simply because they are too stressed and exhausted by the situation that has led to the court hearing in the first place. Some fear ‘reprisals’ against P if they are seen as ‘difficult’ family members.
33. I am currently supporting two members of the public seeking variations of the TO – neither of whom recalls any discussion at all, at the outset of their relative’s COP case, about the restrictions it would impose upon their Art.10 rights. What they remember is being “reassured” by lawyers that their names (and that of their relative) would not be made public, and that the family’s privacy would be protected – but not that they would lose the right to speak out.
34. It seems that there is no proper explanation or ‘anxious scrutiny’ of reporting restriction orders with family members. When supporting family members with cases that have not yet reached court, I explain the TO to them, and help them to engage in a balancing exercise, both in relation to their own rights to privacy and freedom of expression, and in relation to P’s. In a couple of cases, I have recommended publicising as much as possible in advance of the application to the court, such that “the cat is already out of the bag”, in terms of what is publicly available and a TO restrictive of their Art 10 rights is then less likely. For
For families like the Caseys, ensuring that “the horse has already bolted,” or “the cat is out of the bag” can be a very effective strategy for preventing the “draconian” reporting restrictions which sometimes earn the courts a reputation for “gagging” families and for conducting proceedings in “secrecy”. Letting a journalist or public observer know about the hearing in advance is also likely to be of assistance in that they, too, might have arguments to present in court for varying or discharging reporting restrictions.
Celia Kitzinger is co-director of the Open Justice Court of Protection Project. She has observed more than 470 hearings since May 2020 and written more than 100 blog posts.She is on LinkedIn (here), and tweets @KitzingerCelia
(1) This is a reference to the well-known observation by Lord Rodger at §63 In re Guardian News and Media Ltd and others[2010] UKSC 1:“What’s in a name? ‘A lot’, the press would answer. This is because stories about particular individuals are simply much more attractive to readers than stories about unidentified people. It is just human nature. […] A requirement to report it in some austere, abstract form, devoid of much of its human interest, could well mean that the report would not be read and the information would not be passed on. Ultimately, such an approach could threaten the viability of newspapers and magazines, which can only inform the public if they attract enough readers and make enough money to survive.”
Indi Gregory is a six-month-old baby girl who has mitochondrial disease, a rare and incurable genetic condition that drains energy from the body’s cells. She also has a hole in her heart, and soon after her birth underwent operations on her bowel, and her brain to drain fluid.
Despite doctors advising that it may be kinder to let Indi die, her parents Claire Staniforth and Dean Gregory want her treatment to continue. As there is disagreement between the hospital and the parents, Nottingham University Hospitals NHS Trust has made a court application asking the judge for a declaration that it would be in Indi’s best interests not to receive additional life-sustaining treatment or painful interventions, and that it’s lawful for her clinicians to withhold those treatments. The parents oppose this application. There was a hearing on 15 September 2023 in the Family Court.
I am a PhD student researching media representations of end-of-life decisions. I have observed several hearings in the Court of Protection (COP), all of which have provided me with invaluable insights into the court process, and the complex nature of end-of-life decision-making. My experience of COP hearings has enhanced my understanding of these issues and enabled a more informed analysis of media coverage and portrayals of these cases. I’ve written (or contributed to) five blog posts about COP hearings:
So, when I heard that there was going to be a hearing about Indi Gregory, I was keen to observe it. The previous cases I’ve watched have all concerned adults (mostly in prolonged disorders of consciousness) – this would be an interesting counterpoint, and it was also attracting considerable media attention. I want to understand how the media portrays the complex medical and ethical dilemmas that arise in court hearings of this kind, and how media framing – including the language, narratives, sources, and imagery used in reporting – can impact and shape public understanding of end-of-life decisions. Researching and analysing how cases such as these are discussed and portrayed in the media can provide an insight into how public discourse and understandings are influenced, how societal attitudes are constructed and how the media navigates legal rulings about sensitive topics.
Access to the Family Court
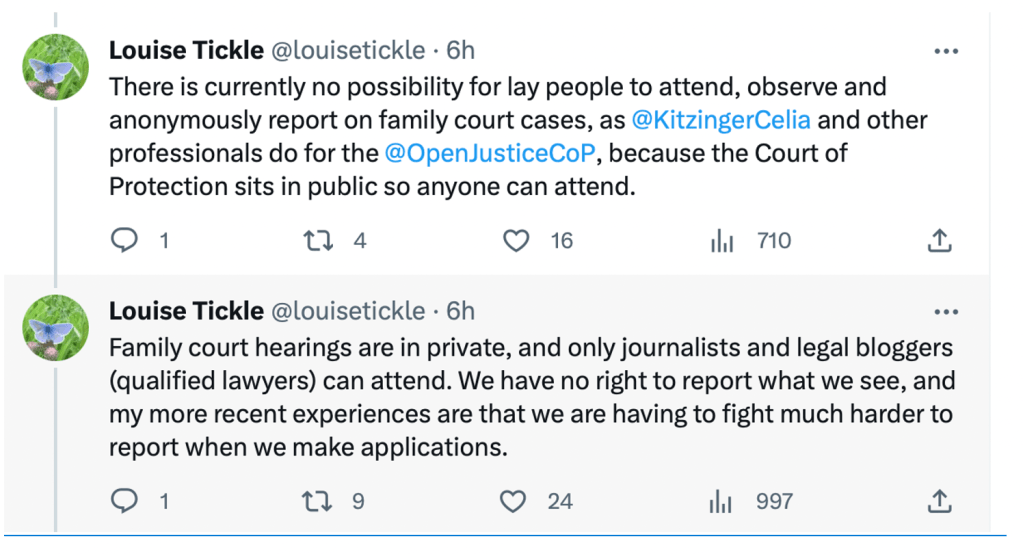
Alas, this hearing was not in the Court of Protection – which hears cases about adults – but in the Family Court – although the judge hearing the case, Mr Justice Peel, also often sits in the Court of Protection. I submitted a request for the link, but I was told (via email) that the hearing would be private. According to Family Court rules, this this means that I’m not permitted to attend because only accredited journalists and “legal bloggers” (who have to be qualified lawyers) are allowed to do so.
The Court of Protection generally conducts hearings in public, allowing members of the public to attend and to report on the proceedings subject to certain restrictions outlined in the Transparency Orders. By contrast, the Family Court primarily conducts hearings in private which means that attendance is limited to journalists and lawyers – and there is no automatic right for them even to report on what they observe.
A journalist who has worked indefatigably for transparency in the Family Court, Louise Tickle, has recently tweeted about this.
The Family Court implemented a ‘Transparency Pilot’ at the end of January 2023 (expected to last for one year) which allows ‘pilot reporters’ (consisting of journalists and legal bloggers) to attend and report on cases, subject to compliance with restrictions noted in the Transparency Orders. (More information about the Transparency Pilot is available on the Judiciary Website (here) and on the Transparency Project website. )The pilot limited to three locations – Cardiff, Carlisle and Leeds – and, unlike the Transparency Pilot in the Court of Protection (launched in 2016 and now incorporated into daily practice), which allows ordinary members of the public to observe, the Family Court’s transparency pilot does not.
Following the email informing me that I would not be able to attend, Celia Kitzinger let me know that she had been granted access to the hearing. Although she is neither an accredited journalist nor a “legal blogger” (according to the definition of the Family Court), the judge had said she could observe. In an attempt to enable me, too, to have access, Celia informed court staff that I was a PhD student studying media representations of end-of-life court decisions and that she was supervising my observations of court hearings, all of which had been Court of Protection hearings so far. We were then told that it should be okay for me to observe, and Celia forwarded me the link.
It was a ‘hybrid’ hearing, and most people attended in the physical courtroom at the Royal Courts of Justice. After joining the link, I spent some time in the waiting room before being admitted. On admission, I was asked to explain – in front of all the assembled lawyers – who I was and “which party I was for”. Following my explanation, I was told that it was a private hearing that I was not allowed access to, and I was publicly removed. For me, the whole situation was highly stressful especially having to speak in court and then be removed, despite having previously been told that I would be allowed to observe. I left feeling frustrated and disappointed.
I would have been very interested in observing this case. I believe allowing both journalists and public observers to be present has a range of benefits – as is apparent from reports arising from both the Court of Protection and from the criminal courts. As Celia Kitzinger has said, in her “Evidence for Ministry of Justice Consultation on ‘Open justice: The way forward‘”
Despite the claim that journalists are “the eyes and ears of the public”, there are, as evidenced below, significant differences between what journalists ‘see’, ‘hear’ and report about court hearings, and what members of the public ‘see’, ‘hear’ and report. Open justice requires that we have direct access to the court and are able to observe for ourselves the process whereby judges and lawyers are “doing justice” with our own eyes and our own ears.
Access to the Family Courts for members of the public, as well as journalists, would supports a diverse range of perspectives, improve transparency, and enhance public understanding and engagement. As I have addressed in a previous blog (here), the benefits of having both media coverage and a blog written by a public observer about the case are substantial. Each piece offers a unique perspective of the case, oftentimes with public observers offering knowledge and expertise from a range of backgrounds.
As Celia Kitzinger says:
…. one case that attracted a lot of media attention concerned whether it was in the best interests of William Verden, a teenager with a learning disability, autism and ADHD, to have a kidney transplant. Media reports (e.g. here) were short, pithy, factual, and aimed at a general readership. But members of the public who observed the hearing and blogged about it did so from specific professional and personal viewpoints and presented sustained and in-depth examination of the issues involved: from the perspective of a medical ethicist and mother of an autistic child (Imogen Gould); as an academic researcher on kidney donation (Bonnie Venter); and as a trainee barrister focusing on advocacy in the court (Jordan Briggs).
What journalists ‘see’, and report is organised with reference to whether it’s (in their terms) ‘a story’ or not. Members of the public observe court hearings through a multiplicity of very different lenses. Compare for example media reportsof the case of the woman with agoraphobia ordered by the court to give birth in hospital with the blogs from our contributors, who include a woman with agoraphobia, a medical ethicist, and some midwives. Each of them brings her or his own unique personal and professional experience to bear, and each of them speaks authoritatively to a specialist constituency in relation to whom they are able to engage with acknowledged expertise.
A fundamental difference between press accounts and the blogs authored by members of the public is that while journalists, by and large, focus on communicating “the facts” and the story behind them, members of the public regularly provide commentary on the case they’ve observed, reflections on their experience of observing it, and make connections with their own personal and professional experience.
The newly-formed “Courts and Tribunals Observers’ Network” is a UK-based initiative focused on how the public can be supported to observe courts and access court information in digital and physical environments. The Network has raised concerns about the “two-tier’ system whereby some categories of observers (journalists and lawyers) get privileged access to the courts.
This case is back in court on 27 September 2023, and I plan to make a written application to observe it in advance of the hearing. Given what I’m reading about the Family Court, I don’t hold out much hope of success, but it seems worth trying – given the huge media impact of the case, and its importance for my own research project in understanding how the media reports on cases such as these.
Rhiannon Snaith is an ESRC-funded PhD student at the School of Journalism, Media and Culture at Cardiff University. Her research focuses on media representations of decisions about life-sustaining treatment, specifically for those without the capacity to make such decisions for themselves. She has previously blogged for the Project here and here. You can learn more about her work by checking out her academic profile and her Twitter profile.
In my first observation of a Court of Protection (CoP) hearing – and first blog – I will take you through who I am and my interest in the Court of Protection, the background of the case my experience of the hearing, and my analysis/reflections of the outcome of the hearing. Professor Celia Kitzinger also observed this hearing and shared some of her notes with me (referenced accordingly). My experience of the hearing, and my thoughts about it (as opposed to my observations of it) are italicised and in blue.
Introduction to the author
I am Hartej Singh Saund-Matharu (he/him), a recent first-class law (LLB hons.) graduate from Cardiff University. I am currently studying the Bar Course at the Inns of Court College of Advocacy with the help of an Exhibition and Frank & Burris Gahan Scholarships from Inner Temple.
My interest in the CoP first arose from studying the law of capacity and consent in my Healthcare, Ethics & the Law module. Having done previous work experience in care homes and hospices, I had observed the outcomes of the decisions made in the CoP from a clinical level and was intrigued to understand the legal perspective on CoP matters. Further to this work experience, I accrued over five years of NHS work as an administrator in GP practices. A primary care perspective on CoP matters gave me better insight into the relationships between public bodies such as Trusts, Integrated Care Boards (ICBs) (albeit they were only CCGs [Clinical Commissioning Groups] when I was last in this job) and local authorities (LAs). This job also helped me understand medical terminology, which oftentimes can be lost to lay persons. Consequently, after an invite to the National CoPPA conference in Cardiff last year, I was enlightened about many of the recent developments and issues in the CoP by speakers such as Senior Judge Hilder, Mr Justice Hayden, Mr Ian Brownhill, Ms Emma Sutton KC and Mr Thomas Jones, just to name a few. In particular, I was introduced to Professor Kitzinger of the Open Justice Court of Protection Project who gave us lots of insight into the transparency issues that face public observers wanting to attend CoP hearings. (This will be discussed further at the end of this blog.)
As a barrister, I am looking to practice in family (specifically child protection) and CoP law. It is those parties who are vulnerable and who may not have the capacity to consent that I wish to aid via participation in decision making on their behalf (of course, even as opposing counsel). The majority of my mini-pupillages have been in child protection law in South Wales, although I am open to (and looking for) any experience working with vulnerable/disabled clients, particularly in the CoP.
Background/experience of the case
This case, Re HJ (COP 14131686), was listed for 10:30am on 13 September 2023 before Poole J in the Royal Courts of Justice (RCJ).
I emailed the RCJ for the link to this hearing at 8am and received a timely response by 9:20am. Both Professor Kitzinger and I joined the MS Teams link at 10:30, to be greeted by a clerk, who informed us that Poole J had several other hearings that morning and Re HJ would be heard at 11:30am. We were informed that the hearing would now be via Cloud Video Platform (CVP) link due to the ICB solicitor, Mr Ed Pollard of Browne Jacobson not being able to attend in person. We were informed that a Transparency Order [TO] was in place and that we would subsequently be sent it by the clerk.
In the meantime, both Professor Kitzinger and I emailed counsel for their Position Statements (PSs) and the Transparency Order (TO). Personally, I only received a reply from Ms Ellie Ward from Capsticks, who represented the Applicant. This was at 11:15am. However Ms Ward advised me that I would only be able to view her client’s PS once the TO had been signed. In particular, she requested a reply to confirm that I had ‘read, understood and agree to abide by the [TO]’. This was promptly done and subsequently the Applicant’s redacted PS was sent at 11:25am. I, of course, agree that PSs should be redacted prior to sending to public observers. On discussion, and only on discussion, with Professor Kitzinger, I learnt that signing of a TO was contrary to standard practice – I would not have known otherwise. Contrary to Ms Ward’s exact phraseology, no signing, whether digitally or on paper, is normally required – just an agreement in writing as previously quoted. Professor Kitzinger informed me that it was a ‘standard TO’. It was at this point that I learnt that the applicant’s counsel was Ms Eloise Power from Serjeant’s Inn Chambers, and that the applicant was the University Hospitals Sussex NHS Foundation Trust. The First Respondent (R1) was HJ (the vulnerable person at the centre of the case) who was being represented by their litigation friend, the Official Solicitor (OS), a paralegal from Biscoes, and Second Respondent (R2) was the West Sussex County Council (CC) (i.e., the LA). On scanning this PS before the hearing was to start 5 minutes later, I read that: “The applicant sought that the protected party (P) was to be temporarily moved from the paediatric ward to the relatives’ suite (normally reserved for EOL patients) due to safeguarding reasons. P has only just turned 18 in the past week and suffers from autism and obsessive-compulsive disorder. Security measures had been put in place for P’s and hospital staff/other patients’ safety too.” The counsel for R2 sent Professor Kitzinger their PS at 11:30, but I didn’t receive a reply.
Professor Kitzinger, at 11:20, informed me that the LA opposed the application to determine ‘which public body or bodies bears responsibility for commissioning of HJ’s social care and whether it is lawful for the Council to cease to commission HJ’s social care’ on the grounds that “[t]he Administrative Court is the appropriate forum for the Trust to challenge the Council public law decision”.
In all honesty, at this point, I was feeling very overwhelmed and beginning to become more anxious. Whilst I did not assume that every party whom I emailed would send me their PS as a public observer, and they are under no legal duty to do so, having to jump over hurdles at such short notice before the hearing or to be ignored completely does not benefit open justice and transparency at all. Bear in mind that at this point, I had still not received the CVP link or the TO from the Court themselves and was very anxious as to whether they were going to send it. Alas, the clerk (as I can see from the email thread) asked other clerks or court staff to send the link, and they passed it between each another until finally, at 11:47 we received the link. I joined immediately, only to have to wait until 12:00 for the hearing to start. This is quite a stark difference in timing from the original listing of 10:30. With all the emailing to counsel and the Court, being advised that the new start time was 11:30 and having to wait anxiously for emails which inevitably are sent last minute, is not a constructive way to interact with public observers. All I could do was try and read the PSs, research the areas of law that may be mentioned in the hearing or do other work. That being said, I, of course, acknowledge how busy the judge and lawyers are and that this is not at the fault of anybody – it is just how the court operates. So, if this happens to you, just know it isn’t intentional and everyone is working as hard as they can!
Thankfully, the audio and video worked well at this point and Poole J, before the hearing, confirmed that all the public observers had received the TO. In fact, he stated (as I paraphrase), that ‘I have been informed that the public observers have received the TO but if there are any public observers that haven’t, please inform the court now’, to which there was silence.
On reflection, after discussion with Professor Kitzinger, this seems to be a more facilitative and expedient approach to confirming receipt and compliance with the TO compared to if a judge individually asks the observers to say ‘yes’. There were some issues with the way the video was being cast – the actual courtroom was not pinned, and the Court made little effort to mute any other public observers. The Court also forgot to unmute the hearing for a short period after we had joined.
Ms Power helpfully provided an introductory summary to the hearing (as recommended by the now former Vice President of the CoP), specifically mentioning that it was mostly for the benefit of the public observers. Ms Power introduced the counsel present who comprised of herself for the applicant NHS Trust and her instructing solicitor as Ms Ellie Ward, Ms Susan Wright of Garden Court Chambers for P (with the instructing OS being Ms Tasha Bibby, a paralegal from Biscoes – P wasn’t present himself; Ms Chiara Cordone of 39 Essex Chambers representing the ICB (who are not a party to the proceedings) and Mr Pollard as the instructing solicitor (who was, as I mentioned, the reason for the CVP link), and finally Mr Michael Paget of Cornerstone Barristers representing the LA. Representatives from the LA, ICB, and NHS Trust were also present. P’s mother (who normally attends the hearings) was not present. Nor was P’s father (who doesn’t normally attend).
In particular, the key issues which were highlighted by Ms Power orally from the applicant’s PS were:
In circumstances where P has no medical reason to be in hospital, which body (or bodies) bears responsibility for commissioning P’s social care package while he is awaiting his discharge from hospital.
Whether it is lawful for the second respondent to cease commissioning P’s existing social care.
It is reiterated that the parties should not allow the commissioning issue to distract attention from the main challenge of finding a suitable placement for H. Finding a suitable placement for P is an absolute priority. P has exhibited very challenging behaviours in hospital such as assaulting a member of the nursing team. Dr H, Consultant Psychiatrist, recommends a specialist placement in order to reduce the anxiety and challenging behaviour and explains that remaining in hospital is unlikely to be helpful to P.
The applicant Trust looks forward to receiving an update on potential providers and hopes that some meaningful progress has been made since the last hearing.
A Deprivation of Liberty Order and a best interests decision are needed.
The latest development is that a possible placement has been identified and is going through the commissioning process (and will need adaptations – boarding up windows and changes to door handles).
In sum, the underlying issue is discharge to an appropriate placement – since as Poole J later said, “if there were an alternative placement we wouldn’t be here at all, because he’d be moving into it”.
In the submissions by Ms Power, which were often counterpointed by Mr Paget, it became clear that Poole J focussed on speeding up the arrangements for transfer as much as possible, and encouraging the parties to sort out between themselves who would commission the care, thereby avoiding having to make a declaration himself. This focus seemed to be as a result of developments with possible placements now in hand.
This approach is pursuant to the notable case of N (Appellant) v ACCG and others (Respondents)[2017] UKSC 22. The important principle that stems from this case is that a Judge cannot order any public body to exercise a discretion.
Professor Kitzinger, helpfully provides paraphrased transcripts of interactions between Poole J, Ms Power and Mr Paget. (As usual for these blog posts, these are based on her contemporaneous touch-typed notes and are as accurate as possible, given that we are not allowed to audio-record hearings, but cannot be taken to be verbatim).
Power hopes that P can be moved on Friday – in which case it would be ‘disproportionate to move him to the family suite’, so he’d stay on the ward until then.
Poole J: If he’s to remain on the ward until Friday, at least, then the court is asked, is it, to authorise the deprivation of his liberty there, for that period with the restrictions previously authorised to remain?
Ms Power: Yes, and should say that for the duration of P’s stay on the paediatric ward, the status quo can continue. However, that does not extend to provision of care if P is moved to the relatives’ suite. So, we have a lacuna if P is moved to the relatives’ suite. And if he’s not to be moved to relatives’ suite, we’ll have to close the paediatric ward.
Poole J: He can’t go to the relatives’ suite until something is sorted out about the care package. He can’t go to a placement because there isn’t one. He can’t go home. So, you are asking me to decide that it’s in his best interests to stay where he is. The Supreme Court has said in previous cases involving children that the scarcity of placements is “a national scandal”. This is a very similar situation isn’t it.
Ms Power: I respectfully agree. It is a national scandal and there’s a limited amount any of us in this courtroom can do to address that.
In circumstances where insufficient places are available in registered secure children’s homes, is the exercise of the inherent jurisdiction to authorise a child’s placement in unregistered secure accommodation lawful?
If it is, what legal test should the courts apply when determining whether to exercise the inherent jurisdiction?
Is a child’s consent to the confinement of any relevance when determining whether to exercise the inherent jurisdiction?
The facts were:
The appellant, T, was a 15-year-old child who was subject to a care order. The local authority, CBC, wished to place T in secure accommodation. Since there were no places available in registered secure children’s homes, CBC applied to the High Court for orders under its inherent jurisdiction authorising T’s placement in non-statutory accommodation. T had consented to the restrictions on her liberty in the placements sought and submitted that the orders restricting her liberty were, therefore, unnecessary.
The High Court did not consider that consent to be valid, and duly made the orders sought by CBC. T seeks to challenge those orders. She does not object to the placements or the restrictions on her liberty but wishes to be recognised as capable of consenting in law.
Case summary In the Matter of T
The Court of Appeal dismissed her appeal. T now appeals to the Supreme Court.
And it was held:
The Supreme Court unanimously dismisses the appeal. It holds in particular that the use of the inherent jurisdiction to authorise the deprivation of liberty in cases like the present is permissible but expresses grave concern about its use to fill a gap in the child care system caused by inadequate resources.
Press summary: In the matter of T (A Child) (Appellant) [2021] UKSC 35 On appeal from: [2018] EWCA Civ 2136
Judge asks whether Friday is realistic – it sounds as though it isn’t.
Poole J: Mr Paget, Friday has been mentioned as a suggested date for P to move. I think the court is invited to authorise his deprivation of liberty in his present circumstances, then it is hoped that arrangements can be made for transfer into the community. How realistic is that?
Mr Paget: I am not able to say that to the court. [The Care Provider] has not provided us with a care plan to be able to commission. I hope just as much as Ms Power, or her clients do that this happens by Friday.
Judge tries to speed things along by adjourning and putting pressure on Care Provider
Poole J: Is it possible to contact [the Care Provider] now and ask them when the care plan will be sent? You could say that the High Court is mid-sitting and wants to know. The court is looking for some levers it can pull to get what everyone wants as the right outcome.
(Whispered conversation between Paget and person behind him – possibly the instructing solicitor or CC representative?)
Mr Paget: We have been using soft powers to encourage [Care Provider] to produce these documents, but it won’t result in him being able to move by Friday we don’t think.
Poole J: (to Ms Power) What’s the end date by which the Trust will accept his continued stay in the paediatric ward before it says “no longer” because the twenty-bed ward would be shut.
Ms Power: Friday. I have asked my client to reflect on what the position would be if a firm move were confirmed for Monday. If the court were to rise while enquiries are made of [Care Provider], should it not merely be asked about the care plan, but also about the timeline for adaptations. Which do seem relatively minor.
Poole J: Yes, if just boarding up the windows. This is a case of pressing urgency. The issue then is if P is to remain at hospital for want of any alternative …. I don’t want to address that. But I will need to. I shall I do that at 2pm.
Ms Power: If P’s stay is to be prolonged or open-ended, I fear I must submit it would become necessary to look substantively at the application for moving him to the relatives’ suite […] to avoid the catastrophic outcome of closing a 20-bed ward. And we are seeking declaratory relief in relation to who bears the cost.
Mr Paget begins his submissions:
(Mr Paget explained the process – details of P are given to the providers. The providers decide whether they have capacity and whether they are suitable given P’s needs. If so, providers work up 3 documents (i) costings; (ii) risk assessment; (iii) fully worked up care plan. Those documents are then considered by a panel, and if the panel agree it’s the right placement, then they draw up a commissioning agreement. In this case, the provider has submitted provisional costings and a risk assessment, but not, as yet, their care plan. They want to see P again tomorrow before providing it. It had been hoped that would happen yesterday – but it didn’t; and the risk assessment only came through at 5.30pm.)
Poole J: So, from here, what’s the expedited timetable?
Mr Paget: As soon as the care plan is provided, we will convene the panel.
Poole J: But when will that be? They haven’t said?
Mr Paget: No. We hope we can do that this week.
[…]
Poole J: I would benefit from knowing when [the care provider] can do that, because then dominoes will fall rapidly into place.
Mr Paget: Procedurally yes, but the adaptations- they hadn’t told us how long those will take.
Poole J: Are they bespoke?
Mr Paget: Yes.
Poole J: In children’s cases of a not dissimilar nature, these have been done within 24-48 hours – the whole process.
Mr Paget: We are alive to the urgency of process. We don’t want to discharge to placement that will fail.
Poole J: No, but the current situation is a failure. […] Well, there we are. It’s not clear when the placement will be available – if it will be available.
The Court then adjourned for lunch. I think there may have been a problem with sound for me on return, as I missed some of the early part of what follows (and rely on Professor Kitzinger’s notes).
Conversation in court after lunch and before the judge returned.
Ms Power: (to Mr Paget) “Go first if you have an update” (can’t hear what Paget says)
Ms Power: “End of next week?! That would not come as welcome news to my client.
That’s too long. Why don’t you say that to the judge and then I’ll probably need a moment to take instructions.”
Poole J returns.
Mr Paget: reports that the panel will have the care plan and will meet on Monday (remotely) and will make the commissioning decision “immediately thereafter” and “the care provider will adapt in that week, ready for transfer, and assembling the care team, ready for transfer on 25th September.”
Poole J: That’s a week on Monday.
Ms Power: We invite the further use of soft power to speed it up a bit. Perhaps if the care plan could be provided by 2pm on Friday rather than at close of play, the panel could convene on Friday afternoon rather than hold it up until Monday. It may seem a small thing but then adaptations could be made over weekend….
Poole J: I am not here to make directions about how soon adaptations can take place. That is not my role. I have my answer as to what the projected timetable is. Mr Paget can tell me whether it’s worth pressing further, but this should be done outside court.
[…]
Poole J: Care plan, yes on Friday and panel on Monday morning. Well, Mr Paget, the court would be gratified to know if the care plan can be provided by 2pm instead.
Mr Paget: (sounding slightly irritable) They are abundantly clear on the situation. Asking them again won’t get a different decision.
Judge rose to enable parties to discuss it at around 14:45.
I was getting rather anxious at this point, having potentially missed a significant development and having to wait further to hear this case that was meant to start at 10:30 and last for an hour. On reflection, the lunchtime adjournment seemed beneficial to P given this development. I was shocked to see and hear how firm Mr Paget was with Poole J, but on reflection, I understand that counsel must be firm and advocate ‘fearlessly’ as described in the Code of Conduct. My anxiety persisted as Poole J had asked to restart at 15:00 but this had not happened until 15:14 – of course, the public observers could only wait patiently whilst we could not hear what was happening in the court and if they had started and it left us looking at the Court coat of arms. It had been my thinking that the court staff had caused some technical issues for us by forgetting us, but thankfully this was not the case. I began to understand that hearings can be multiple successive dynamic interactions in real time. Poole J’s role in this case was very important due to the developments and changes in position over the course of the hearing, as he had to allow adjournments for any necessary actions to take place. Poole J is evidently a judge who is committed to creating space for parties to sort out the problems themselves, whilst giving them a steer as to what is needed. In this way, I thought Poole J was very strategic in court, and that he used the court powers very well to facilitate and enable progress – rather than simply wielding power or lamenting the limits of his power.
On return at 15:14:
Ms Power: A certain amount of harmony has broken out. The ICB is prepared to commission care for P on the Relatives’ Suite, so the subject matter of my application falls away.
This is significant. Again, it seems that this adjournment was particularly beneficial to P and the court – my thoughts on adjournments in general have become more positive as a result. The ICB does not generally have the power to commission care in cases such as these and therefore could be viewed as acting ‘ultra vires’ but in the best interests of P (of course with caveats). This pragmatism and harmony between the parties is duly noted in Poole J’s summing up, which I reproduce as accurately as possible below:
Summary Ruling from Poole J
I’m concerned with [P] [and with regards to the TO]. He turned 18 only last week, so he is an adult. He has relatively recently been diagnosed with autistic spectrum disorder and obsessive-compulsive disorder. He did live with his mother, but a significant deterioration in his condition and his behaviour led her to be unable to care for him at home. She has not attended today by choice. She has attended previous hearings in this case. The protected party’s father is aware of the proceedings, he has so far chosen not to participate in them. He [P] was admitted earlier this year to hospital in July and briefly detained under s2 of the Mental Health Act 1983 and he was discharged from that detention on the 24th of August 2023. His behaviour has put himself and others at risk. He was involved, as I’ve heard today, in an assault on a member of staff at the hospital and whilst at home he ran in front of vehicles on a public road. I’ve read the assessment of him by Dr H, who I believe took the decision to discharge him from detention under s2 in August.
The paediatric unit, where he is currently accommodated, is a 20-bed ward. I am told that six beds are out of commission due to P’s presence. I was told at the opening of this hearing, that the Trust is considering moving patients out and indeed even closing the ward due to his continued presence there and the risks that that presents both to him and the others. That would be an extraordinary consequence of the unavailability of suitable adult care for him in the community.
He does have complex needs and the case has been before the court on six occasions, since the 25th of August – as many as 5 times last week when this case was before the court. And I’m afraid that it appears to me there was during that period no concrete progress. Today at the hearing after further enquiries, the LA, told me through Mr Paget counsel, that a care provider who has already been identified by them and who had indicated that it was willing to provide care for P at a placement in the community, needed until close of play, which I took to be 4pm on Friday 15th September, to produce a detailed care plan. That and other necessary documentation, if provided to a commissioning panel, that could meet on Monday and make a decision on Monday. Adaptations would be required for the planned accommodation for the placement. And I have been told that they can be completed by the end of next week, such that the placement could in principle be available if commissioned for P to transfer to it on Monday 25th September. That is the planned timetable. It isn’t in any way a guaranteed timetable, for example, the commissioning panel has still to make a decision about commissioning the community placement.
I’ve encouraged the LA through Mr Paget to have a Plan B and he assures me that they have as much in mind and actively consider alternatives. The Trust position at the opening of the hearing, was that it was highly reluctant, to say the least, to continue to accommodate P. The Trust could simply just discharge P into the community because he has no medical and that includes physical or mental condition. There is no medical reason for him to remain in hospital. It is purely because of the lack of anywhere else for him to be accommodated that he continues to reside there. The Trust then would be extremely reluctant for the reasons I have already articulated for him to continue residing in the manner in which he does at the paediatric ward at the Trust hospital. However, it would continue to accommodate him, notwithstanding the cost to other patients and their families and to him, but not indefinitely, and the Trust is very concerned about the timetable that I have already referred to. It has accommodated him for nearly 3 weeks already, with the costs – I don’t mean just financial costs – but the consequences for him and others that I’ve referred to. So, it is unappealing for the Trust to face another 12 days of that.
An alternative which had already been noted was to move P to a family suite within the hospital. That is a suite where families of terminally ill patients can stay close to them at the hospital or in the hospital grounds. Mrs Justice Morgan said that she was ‘dismayed’ by that prospect, as would anyone given the consequences for the families of those other patients. However, this is a case where there are many disagreeable consequences of various decisions that could be made. I have to be concerned at present with P’s best interests. He lacks capacity, there are grounds/reasons to believe he lacks capacity, as previous judges have foun,d and I do again, to conduct this litigation and make decisions about his residence and care. Therefore, the court has to consider and put itself in his shoes and consider what decision should be made about residence and care in his best interests.
After standing the matter down for some time, the court has been told that the ICB, which I think I am in right in saying is not a party to these proceedings, but appears and I’m very grateful to it, that the ICB is willing on a pragmatic basis, itself to commission care for P upon him moving to the family suite within the hospital. They have thereby unlocked the possible provision of that care because previously, if I can be excused for putting it this way, there has been something of a standoff between the parties in relation to the commissioning of care within that particular setting. The condition is that it is done without prejudice to the ICB’s position, that it is in fact the LA’s responsibility to commission such care. It is also and without prejudice to any other cases. The ICB is anxious to report that this is not a precedent to other cases but a pragmatic decision taken in the individual circumstances of this case. The third qualification is that the ICB is not in a position to monitor and deploy the package. It is willing to commission and will rely upon the other parties, but with the LA feeding into it to monitor and deploy the package of care. I repeat that I am extremely grateful to the ICB for unlocking that part of this difficult case. In those circumstances, the Trust is willing to continue to accommodate P in the hospital, but with a view to him transferring to the family suite once preparatory work has been done. This will allow an opportunity also for the OS to make contact with P and for P’s own wishes and feelings about the move to the family suite to be ascertained. I am told, and have no reason not to accept, that P himself is keen to make that move, but the OS has not had an opportunity to make contact with him to discuss that particular issue. In these circumstances, I’d argue that general liberty to reply in relation to this order on short notice and so, if necessary, if for example there was an extreme adverse reaction from P to the proposed move to the family suite, depending on the circumstances, the matter could be brought back before me if available for further application and review.
In any event, I should review this case again reserved to me on the 20th of September because by that time, firstly any move to the family suite should have taken place and I could be updated on that,. Secondly, the commissioning decision should have been made in relation to the community placement and I can be updated on that. And thirdly, it should be clear by then that the adaptations necessary to the community accommodation were on track and that the placement should be available for P to move into on the 25th of September. In the alternative, if that is not on track, I can review the case and make the appropriate orders if necessary. In order to accommodate that hearing, which will be a remote hearing at 10 o’clock on the 20th of September before me, which I will list for 1 hour, updating evidence will be required from the LA and the Trust and I give permission for the OS to adduce any further evidence by way of attendance notes for example, which should be provided by 4pm on the 19th of September.
I have to consider the position in the interim in relation to P’s deprivation of liberty. Previously, at the court hearings I’ve alluded to, authorisation has been given for the deprivation of P’s liberty with a number of restrictions that are set out most recently in the annex to Mrs Justice Morgan’s order of the 8th of September 2023. They include, as I’ve already referred to, supervision by staff and a 2:1 ratio at all times in his room and other security measures. They also include monitoring during toilet visits, windows of his room are boarded up – that is not for any reason other than at his own request because he becomes distressed when the room is not at the ground floor, at the view he can see through the window and so prefers to have the windows boarded up. The doors closest to his room on the ward are also locked. He is not free to leave the ward unaccompanied. There is no permitted restriction in relation to physical restraint, so the annex reads ‘no physical restraint to be used at present with P verbal de-escalation to be instead used’. Items that he could use to harm himself are removed from his possession. In terms of those restrictions, there is no doubt that they amount to deprivations of his liberty to which he is unable to consent and they are is imputable to the state. I am satisfied that the continuation of those restrictions within the hospital, whether on the paediatric ward or on the family suite are necessary, proportionate and in his best interests. In particular, I have in mind that there is nowhere else for him to go and that he has become in fact more calm and settled of late with these provisions in place, that they are permissive, that in some ways he welcomes the feeling of security and that physical restraint is not amongst the restrictions which are permitted.
I therefore do give the authorisation of the deprivation of his liberty within the hospital, either on the paediatric ward or the family suite and I do so until 23:59 on the 20th of September where I’m due to hear and review this case earlier that day. It is unedifying for public authorities to dispute with each other in litigation, the responsibility of the care of a highly vulnerable young adult and for resources to be taken up in litigation when what is needed is a collaborative pragmatic approach. What I’m pleased to report, is that that is the approach that has been taken today and the pragmatic agreement as to how to move forward has been reached after discussions today.
I acknowledge that that has not always been easy for the parties involved, who are mindful of more general principles, but I am grateful to them for the work that has been done today. I would also like to record my thanks for all the staff that have been involved in the care of P – not an easy job and it appears that they are doing an excellent job and that he has become more settled as a result of that. I am grateful to the Trust and to the staff for all they have done to care for P and continue to do so.
This summing up is a testament to the skill of Poole J – it could easily have become much more confrontational and a rather oppositional hearing with a frustrated judge feeling powerless to do anything about it. This pragmatic harmony seems to be the best-case scenario for P on the facts, especially considering P has just turned 18 and is still on the paediatric ward where he has been a risk to others. It is important to note that P’s wishes were also to move to a room on the ground floor (i.e. the relatives’ suite) as he gets triggered by looking out of the window, hence why they were boarded up. So, the ICB’s intervention has facilitated P’s wishes being included in the best interests decision.
Following the summing up, a question was raised about the TO and whether where P lives or might be cared for might become apparent if specific security measures were described, and an amendment was made.
It is important to note that this amendment was prompted by an intervention from a journalist, Mr Brian Farmer. Open justice in the CoP relies not just on journalists making demands for their Art. 10 ECHR right to freedom of information, but also on journalists recognising the risks when putting certain information into the public domain and raising this with the judge.
At the end of the hearing, I received another email from Ms Ellie Ward, who wanted to confirm that I was present for the amendments to the TO and understood its terms. She informed me that, cnce the amendments were formalised, she would send the amended TO to again. I am yet to receive this new TO.
The next hearing is listed at 10am for 1 hour on Wednesday 20 September 2023 before Poole J.
Post-Hearing Reflections
It is evident that this was a difficult hearing for the parties. I have learnt that even despite the parties coming to the court because they have not been able to resolve the dispute out of court, Poole J guided them into finding this resolution, even if this is because of N v ACCG and the court’s inability to create new options for P, meaning the court can only choose between the available ones. This extends to the court not being able to order any party to create new options.
It is also apparent that there is a problem with the availability of accommodation for young people. I agree that it is a “national scandal” and am hopeful that this is a consideration that every CoP judge and lawyer has at the forefront of their minds when considering the best interests of P in cases such as this one.
I discovered that CoP hearings are never as they are listed. This is the sixth hearing I have attempted to observe online as a public observer. At the other five, either the matter was dealt with on paper, or in person without a remote link (contrary to the listing), or was listed incorrectly or the link to join was not sent and my email request was not even acknowledged. This hearing was a bigger time commitment, much more than the hour or two that I was expecting. If you plan to observe any CoP hearings, expect the unexpected and make sure you: 1) have a relatively flexible day and 2) have work that you can stop and start easily whilst waiting. I expected there to be some delays between 30-60 minutes, given my experiences within the family court. However, I did not expect there to be more delays given the revised start time. I cannot fathom the costs that this must involve given there were four barristers and four instructing solicitors.
My question to practitioners is: How do you respond and negotiate these delays if you have another hearing scheduled for later on in the day? Is it anticipated that hearings such as these will be lengthy and so your schedule is blocked off or is your duty in this situation to inform the court of the next hearing? How do you deal with such a degree of uncertainty (and stress/anxiety) on a daily basis?
I feel that despite all my previous experience within the NHS and with vulnerable patients, I was thrown into the deep end with this hearing. It was an invaluable experience that showed me the difficulties of the parties working together for the best interests of P but without compromising their duty towards their client. It’s a fine balance to be struck depending on the instructions given to counsel by their client and that was evident with the inflexibility of the LA. However, this hearing has also showed that the overriding objective to act in P’s best interests is the reason why the ICB used their discretion to extend their powers. This “pragmatic harmony” (the judge’s phrase) is not at all what I was expecting when I first joined the hearing, but it has brought me some solace that P’s wishes can be enacted and hopefully, depending on the outcome of the next hearing, can be facilitated up to the point he is under the care of the community care provider.
If I can, I will aim to observe the hearing at 10am on 20 September 2023 and any subsequent hearings, although I appreciate that five hearings were held last week for P and the court hopefully should not need many more hearings as P is soon to go to the community care provider. In any case, I will aim to observe more hearings in future, and I would strongly advise other aspiring barristers – and anyone else interested in the Mental Capacity Act 2005 and best interests decision-making – to do so too.
It is definitely worth noting that despite my anxieties throughout the hearing, observing was highly interesting, productive, and informative. My anxieties can probably be put down to my relative inexperience observing CoP hearings and being thrown into the middle of a case with only a basic understanding of CoP law. So please don’t be put off if you want to observe! I have gained a deeper respect for the court staff and CoP lawyers/judges, especially their patience and pragmatism.
I am extremely grateful to Professor Kitzinger for all the advice and assistance she has given me throughout this process.
Hartej Singh Saund-Matharu (he/him) is a Bar Course student at the Inns of Court College of Advocacy, first-class Law (LLB Hons.) graduate, and recipient of two Inner Temple scholarships. He is an aspiring Court of Protection and Family Law barrister. He has accepted an offer for pupillage at 30 Park Place commencing in September 2025. His LinkedIn is https://www.linkedin.com/in/hartejsinghsaundmatharu/
This case concerns a young man who has recently turned 18. He is currently present on a paediatric ward despite having been ready for discharge back in August (about three weeks ago). This situation has arisen due to the lack of suitable placement options. Furthermore, he cannot live with his mother, as he did previously, because there was a serious deterioration in his behaviour and condition (autism and obsessive-compulsive disorder).
In desperation to get him off the children’s ward (where he assaulted a staff member and threw an object which hit a child), the hospital Trust has applied to the court for an order that he be moved to the Relative’s Suite within the same hospital. This is usually used for families whose child is dying. It will be unavailable to such families whilst the young man is living there.
The hearing
As a law student at King’s College London, much of my time is spent reading about the law in books and articles. Observing a Court of Protection hearing has ‘brought the law to life’ because I am effectively following people’s legal issues ‘in real time’ as they are decided before the court. I was also keen to watch practising barristers deliver their oral submissions in court as I could employ some of the techniques they use in my own advocacy, both in moots and in my future professional practice.
The hearing I observed was scheduled for 10:30am on 13 September 2023. However, the official start time was pushed back to 11:30am and the actual start time was well after mid-day. When the hearing did start, it was held in a hybrid format with the judge, Mr Justice Poole and counsel for the parties being present in London whereas I was observing remotely via a CVP (cloud video platform) link. This set-up worked well as I was able to clearly hear and see the court proceedings throughout.
Eloise Power for the applicant, University Hospitals Sussex NHS Foundation Trust began with an introductory summary of the case. The person at the centre of the hearing (P), the 1st respondent, was represented by Susan Wright. via his litigation friend the Official Solicitor. The second respondent was West Sussex County Council, represented by Michael Paget. In addition to counsel for the parties, there were other people present at the hearing. There was a barrister representing the Integrated Care Board (ICB), instructing solicitors for the applicant and respondent, the Divisional Director of Nursing, and the Assistant Director of Adult Operations. Most observers joined via video link; however, Brian Farmer from the Press Association was present in the press bench (see this media report: “Man staying in hospital’s children’s ward in West Sussex”).
The applicant was seeking a deprivation of liberty order so that P could be kept in the hospital now and moved to the Relative’s Suite. Mrs Justice Morgan in the previous hearing had expressed great concern about this move because it would mean families couldn’t use it, but Eloise Power for the applicant highlighted that the situation would be much worse if P continued to stay in the children’s ward. This is because six beds are currently out of commission to accommodate P and the Trust is considering closing the entire ward due to his presence.
The applicant was also seeking a two-part declaration. The first question to be addressed was who is responsible for commissioning P’s social care package when there was no medical reason for him to be in hospital and while he is waiting for discharge from hospital. The second question was whether it is lawful for the second respondent to cease commissioning P’s existing social care. The main area of contention between the applicant and the respondents was the issue of who should pay for P’s care if or when he is moved to the hospital suite. The problem was that he could not be moved until this was agreed and if he was not moved by Friday, the Trust was considering closing the whole paediatric ward.
To resolve the ‘stand-off’ which had occurred regarding the provision of care, the ICB who were not a party to the proceedings but were represented by Chiara Cordone said that they would be willing to commission care for P upon him moving to the Relatives Suite. They said (and the judge accepted) that they were making this offer without prejudice to their position, and it should not establish a precedent because, in their view, care should really be provided by the local authority.
Michael Padget, for the second respondent said that they had sourced a potential care provider who would be willing to provide both care and a suitable placement for P. They have given a provisional costing and risk assessment, but they have not created a fully worked-out care plan; they want to see P again before providing that.
At the end of the hearing, Mr Justice Poole delivered an oral judgment. He gave authorisation to deprive P of his liberty with the same restrictions that were in place before. These include supervision by staff at all times on a 2:1 basis, plus additional security arrangements, supervised toilet visits, the requirement that his windows be boarded up (which he asks for) and that the doors closest to the room are locked and he is not free to leave the room on his own. The judge said that care staff are limited to the use of de-escalation techniques rather than physical restraint to manage P’s behaviour. These restrictions were justified on the basis that they are necessary, proportionate and in P’s best interest. This deprivation of P’s liberty in the hospital will last until 11:59pm on 20 September 2023. This will be reviewed by the court on the morning of 20 September 2023 at a 10:00am hearing before Poole J.
It is expected that by this time, any move to the Relative’s Suite should have been made and the commissioning decision should have been made, and the adaptations to the community accommodation such as the windows being boarded up and door handles being secured, should be on track. If this has not happened, then the case can be reviewed.
Reflections
After the hearing had ended and the judgment was delivered, I reflected on what I had learnt. I am still a very new Court of Protection observer – this is only the second hearing I’ve observed – so I was able to consolidate my understanding of the Court and the various terms and roles associated with it. For example, I gained a greater awareness about the office of the Official Solicitor which acted as P’s litigation friend due to his lack of capacity to instruct a legal team. This means that the Official Solicitor can decide the instructions given to the barrister who represents P in court; in accordance with the Mental Capacity Act 2005, these instructions should be in P’s ‘best interests’.
One of my main observations during this hearing was that the style of advocacy adopted by the barristers was very inquisitorial due to the focus on working collaboratively for what is in P’s best interests. This contrasts with the much more adversarial style I have observed in criminal cases or when I have watched and taken part in moots at university.
I also learnt about the dire situation in social care in relation to secure placements. Unfortunately, the demand for a secure placement is far greater than the supply. This means that people who need this type of accommodation find themselves in wholly inappropriate settings. In May 2022 the Daily Mail reported that 62 children needed a secure placement, but there were only two available. These secure placements are incredibly important for children because they help to “keep children safe, restore stability to their lives and assess their needs and identify the supports needed in the future.” The hearing I observed was just the tip of the iceberg of a much bigger problem.
I am incredibly grateful for the opportunity to attend this hearing; I hope to attend even more in the future. I would also encourage others to attend a hearing because the work done in the Court of Protection, which is based on the Mental Capacity Act 2005, overlaps with a range of legal practice areas such as human rights, family law and medical law so there is bound to be something of interest for everyone.
Ahmed Hussain is a final year Law student at King’s College London. His LinkedIn profile is here: linkedin.com/in/ahmed-hussain-987b791b3 He tweets @ahmedhussainlaw
Introduction: On 21st October 2022, I submitted (at the request of counsel and with the permission of the court) a witness statement to Mrs Justice Lieven, concerning Case no. COP 13180943). I was asked to supply evidence as to how, according to my observations, Transparency Orders are actually working in practice. This came in the wake of Mr Justice Mostyn’s expressed concerns about Transparency Orders in Re EM [2022] EWCOP 31. I’ve reproduced the bulk of that evidence below because I want it be publicly accessible now that I’ve also recently (a) sent it to the ad hoc working group of the Court of Protection Rules Committee working on on Transparency Orders and (b) referred to it in my evidence to the Ministry of Justice on “Open Justice – the Way Forward”. It starts with §6 because I’ve left the numbering as per the witness statement as submitted (and omitted the first 5 paragraphs about me, setting out my personal academic background and experience). The statement is substantially based on an analysis of Transparency Orders at what were then the most recent 50 hearings I’d observed. I have no evidence of any significant change since then. I look forward to developments following the Rules Committee work on how to do transparency better. [Celia Kitzinger]
*****
IN THE COURT OF PROTECTION CASE NO: 13180943
AND IN THE MATTER OF THE MENTAL CAPACITY ACT 2005
AND IN THE MATTER OF COP Rule 4.2
B E T W E E N:
PM
Applicant
-and-
(1) B CITY COUNCIL
-and-
(2) B INTEGRATED CARE BOARD
-and-
(3) HM
(by his litigation friend, the Official Solicitor)
Respondents
FIRST WITNESS STATEMENT OF CELIA KITZINGER
[Paragraphs 1-5 omitted – they outline my academic qualifications and publications, and the history of the Open Justice Court of Protection Project]
6. I have been asked to provide a statement drawing on my experience, in practice, about:
(i) the extent to which reporting restrictions in the Court of Protection are the outcome of a balancing exercise weighing the protected party’s Article 8 right to privacy against the public’s Article 10 right to freedom of information; and
(ii) the extent to which those against whom injunctions are made have the opportunity to ask for reporting restrictions to be varied, making a case for the exercise of our Convention right to freedom of expression.
In summary (each of these points is subsequently evidenced)….
(i) There is rarely evidence of any balancing exercise
7. In the vast majority of hearings I observe, I do not see any evidence that the court has engaged in anxious scrutiny of competing convention rights in drawing up a Transparency Order (TO) or Reporting Restriction Order (RRO).
8. I often see evidence that TOs are treated as taken-for-granted, standardised “boilerplate” documents that do not require any balancing exercise from the court. They are sometimes authorised without the judge appearing to know what reporting restrictions they are thereby imposing, since they ask counsel if there is a TO and then re-use (without amendment) one they’re told is in the bundle (often made by a different judge) without appearing to have read it. Judicial summaries of reporting restrictions in the TO are frequently inaccurate (I would say, more often than not).
(ii) There is rarely any opportunity for assertion of Article 10 rights from the public (or journalists)
9. Members of the public are very rarely in a position to engage with the reporting restrictions imposed upon us. Reporting restrictions are usually (with rare and significant exceptions) presented as a fait accompli which we are expected to accept unquestioningly as a condition of entry into the court. I have noticed that there is a little more latitude for intervention from journalists – but even for journalists there is rarely much opportunity provided for them to question the reporting restrictions.
10. I do not take a position here on whether such a balancing exercise is required by law, or whether it would be a necessary and proportionate use of court time in every case. I am certain however that the current system for determining and implementing reporting restrictions is not working and needs to be thoroughly overhauled.
Two additional points:
(iii) Injunctions with reporting restrictions are very often not served on observers, so cannot serve their intended function
11. Members of the public very often do not receive any written version of the reporting restrictions: around half of the blog posts published by the Open Justice Court of Protection Project are published without sight of a TO or RRO. Since it is rarely suggested that we have breached reporting restrictions, one implication could be that an injunction against us is not needed. However, the absence of TOs (after their existence has been raised in court) has a chilling effect on transparency because we have no written record of what we are and are not allowed to report, and under those circumstances many members of the public are frightened to say anything at all, and it may be the case that we are over-cautious about what we publish in the blogs – for example there is often anxiety about naming public bodies and expert witnesses.
(iv) The language of the ‘standard’ Transparency Order is incomprehensible to most members of the public
12. Very few observers (except those with legal qualifications) are able to understand the TO and what it does and does not permit them to say. For example, there is a recurrent problem with the standard wording that prevents publication likely to identify that “AB is the subject of these proceedings (and therefore a P as defined in the Court of Protection Rules 2007)” – where AB are the initials a judge has assigned as those to be used in publishing information about P. A typical response: “If I have to refer to him as AB, and then I can’t say he was in this Court of Protection case, because it says I’m not allowed to say AB is the subject of the proceedings, that means I can’t say anything.” (I could give many more examples of the confusion and resultant chilling effect on transparency occasioned by the ‘standard’ wording).
EVIDENCE BASE
13. I write this statement as a member of the public and as co-director of the Open Justice Court of Protection Project and editor of its blogs[1]. I am not a lawyer or a journalist. I am not a “legal blogger”[2].
14. In preparing this statement, I draw upon:
my experience over the course of the last decade with supporting family members involved in serious medical treatment cases – voluntary work carried out as an offshoot of my work with the Coma and Disorders of Consciousness Research Centre at Cardiff University;
my experience over the last two and a half years, with the Open Justice Court of Protection Project, supporting other members of the public to observe hearings and myself observing more than 360 Court of Protection hearings;
a systematic analysis (prepared specifically for this statement) of reporting restrictions issues as they arose in the 50 most recent hearings I’ve observed (as of 10th October 2022, listed in Appendix 1), held between 29th April 2022 and 10th October 2022.
THE ‘STANDARD ORDER’
15. The ‘Standard Order’ template for making reporting restrictions in the Court of Protection (the “Transparency Order”) has been used since 29 January 2016 with the introduction of the Transparency Pilot. It was cemented into the practice of the court in 2017 via Practice Direction 4C, which states:
§ 2.1 The court will ordinarily (and so without any application being made)—
(a) make an order under rule 4.3(1)(a) that any attended hearing shall be in public; and
(b) in the same order, impose restrictions under rule 4.3(2) in relation to the publication of information about the proceedings
16. The most salient paragraph of the ‘Standard Order’ for public observers is the list of “material and information (the Information)” covered by the Injunction. As observers, we understand that we are “persons bound by the injunction” (#5) and what it prevents us from doing (#7), and the matter of duration (§8) is rarely at issue. It is to #6 (or its equivalent in any actual TO) that we turn to check what we are or are not allowed to report.
Remote hearings
17. Until the public health restrictions imposed by the government due to the coronavirus pandemic in March 2020, it was usual for the Court of Protection to sit in public for most “attended hearings” (i.e. those “where one or more of the parties have been invited to attend the court for the determination of the application” §2.2 Practice Direction 4C). The Vice President notes that “Attended hearings can be remote hearings for these purposes.” (§55 Remote Access to the Court of Protection Guidance, 31 March 2020[5]).
18. The situation was reversed in the Vice President’s 31st March 2020 Guidance. It states that PD 4C should be disapplied for remote hearings, and any TOs already in place for established proceedings discharged (§57). In view of the court’s commitment to transparency, however: “In each case active consideration must be given as to whether any part of any remote hearing can facilitate the attendance of the public, if so Practice Direction 4C may be applied and the transparency order reissued.” (§59). This is now the usual practice in the Court of Protection for remote hearings (other than hearings in the Royal Court of Justice, which are usually listed as “in open court” whether they are in person, remote or hybrid)[6].
19. An alternative practice for remote hearings has been adopted by some judges whereby PD 4C is disapplied and the hearing remains a private one, to which an observer is admitted, subject to a Reporting Restrictions Order (RRO). In my experience this is a minority practice.
EMPIRICAL FINDINGS
Boilerplate or “anxious scrutiny”?
20. There is a small minority of hearings partly, or wholly, devoted to the reporting restrictions themselves in which it is absolutely clear that there is anxious scrutiny of reporting restrictions. These include (successful) applications from the press to name P (as Laura Wareham [351][7] and Robert Bourn [360]) and a case where the judge invited submissions about an interim RRO he’d imposed at the beginning of the hearing preventing reporting that P was being covertly medicated [362]. These are exceptional cases.
21. In the majority of hearings, the language used by the judiciary and by advocates in court conveys the impression that reporting restrictions are effectively boilerplate text used from a template and deployed over and over again without making significant changes – that they are routinised and predictable, rather than the outcome of anxious scrutiny of competing convention rights in the individual case in question.
22. Drawing on contemporaneous notes from the last 50 hearings I’ve observed, there are references to: “the usual Transparency Order” (DJ Glassbrook [240]); “the Transparency Order is in the usual terms” (Arbuthnot, J [345]); “in the usual terms” (HHJ Hildyard KC [327]). Advocates also talk this way: “it’s the standard order in the standard terms” [357]; “the Transparency Order is inthe standard terms” [320]; “Usual transparency orders apply as you know (do not identify family, P, clinicians etc)” [330].
23. Judges and advocates who know that I regularly observe court hearings sometimes display the assumption that I will know – without being told – what is in these “standard” orders: “Professor Kitzinger probably knows the terms of the injunction better than most practitioners” [342]; “Professor Kitzinger is here and understands the reporting restrictions”[338]; “I make the usual order that publication is permitted except that you can publish nothing to disclose P’s name, or the names of P’s family members, or of P’s current placement. I have been over that many times with Professor Kitzinger” [356].
24. Most of the TOs I am sent are virtually identical except for the initials used for P.
For example:
25. It’s quite common to receive (sealed) TOs that bear clear evidence of a ‘cut and paste’ approach and are insufficiently ‘personalised’ for the particular case (e.g. no initials for P, or the wrong initials, or a template that hasn’t been completed). I don’t see this level of inattention to detail in other documents before the court: position statements and substantive orders are usually impressively free of typos etc. and the latter are subject to careful attention by judges. This contrast between the quality of TOs and other court documents suggests a degree of inattention to the details of TOs
26. The TO from which the first of the extracts above is taken [328] was sent by court staff in advance of the hearing, attached to an email in which the judge was quoted as having said, “requestor is welcome to attend subject ONLY to confirmation that she has received copy of TPO”. I confirmed receipt at the beginning of the hearing – but that didn’t seem the right time to raise the deficiencies of the order I’d been sent. It seems unlikely that the judge can actually have read it. (Another member of the public, Bridget Penhale, Co-editor Journal of Adult Protection, and an elder abuse and adult safeguarding specialist, tells me she also has received a blank template TO for a different hearing.)
27. The same inattention to detail in TOs extends beyond the paragraph concerned with “The subject matter of the Injunction” and is sometimes apparent across the whole document. For example, one TO gives P’s initials as MH and those initials [MH] are used sometimes in the TO, including in the “subject matter of the Injunction” section, but there are also places where they should have been entered and have not and it instead reads “[the initials chosen to identify P]” [355]. Another TO uses “P” rather than “LD” (the nominated initials) for the person at the centre of this case and there are omissions throughout, e.g. “1) This application be set down for an attended hearing on [missing date] at [missing time] with a time estimate of [missing time estimate] at which the Court will consider the following issues:…”. (3) The attended hearing is to be listed as follows: [but nothing follows) [357]
28. Transparency orders are not supposed to have a Confidential Annex – but both [314] and [322] have these, with full postal addresses for P and P’s family in [332]. They do this despite also including a paragraph that instructs them not to add this confidential information and to keep the list of names “separately from other parts of the Information”.
29. Another member of the public, Ruby Reed-Berendt (academic lawyer) tells me she was also sent a TO with a Confidential Annex. This concerns me because it means that confidential information (often beyond the information revealed in the hearing) is sent in written form to members of the public and hence renders people’s identities vulnerable to exposure (e.g. via a lost laptop, an overseen printed version).
OPPORTUNITIES TO ASSERT RIGHTS TO FREEDOM OF EXPRESSION + ASK FOR THE TRANSPARENCY ORDER TO BE VARIED
Family members of P
30. Family members and other lay persons involved in COP proceedings as parties, witnesses, observers, or in other roles (e.g. attorneys, deputies) are also bound by the TO – and it impacts upon their freedom of expression more severely than it does observers , because in speaking about (for example) “my son” or “my mother”, under their own name, in connection with a COP hearing, they are “likely to identify” that person as a P in the Court of Protection.
31. In many cases, family members seem content with these restrictions. In a significant proportion of cases, they are not. In hearings I’ve observed, the TO has led to restrictions on family members that they hadn’t understood in advance and do not want. These restrictions have included: use of fundraising platforms; talking to friends and relatives in search of evidence about P’s former values, wishes, feelings and beliefs; sharing updates about what’s happening with P on closed Facebook pages or their own publicly accessible blog posts; seeking out expert opinions of their own for P; and media, public education and campaigning activities. Often – even when they are parties to the case – family members do not realise that they are bound by the TO, and that it restricts their freedom of speech. It seems there is rarely any attempt to explain this to them (until after a breach is seen to have occurred).
32. Many of the families I’ve supported through serious medical treatment cases find themselves angry about being “silenced” or “gagged”. They have come to believe that the TO protects clinicians, not P. Some of the family members who’ve contacted me through the Open Justice Court of Protection Project say similarly that the court is attempting to silence them because of their criticisms of the healthcare or legal systems. Reporting restrictions are viewed as damaging P, not protecting them. Most have not, in fact, been willing to challenge reporting restrictions – believing it will be another expensive court battle, or that they are bound to lose anyway, or simply because they are too stressed and exhausted by the situation that has led to the court hearing in the first place. Some fear ‘reprisals’ against P if they are seen as ‘difficult’ family members.
33. I am currently supporting two members of the public seeking variations of the TO – neither of whom recalls any discussion at all, at the outset of their relative’s COP case, about the restrictions it would impose upon their Art.10 rights. What they remember is being “reassured” by lawyers that their names (and that of their relative) would not be made public, and that the family’s privacy would be protected – but not that they would lose the right to speak out.
34. It seems that there is no proper explanation or ‘anxious scrutiny’ of reporting restriction orders with family members. When supporting family members with cases that have not yet reached court, I explain the TO to them, and help them to engage in a balancing exercise, both in relation to their own rights to privacy and freedom of expression, and in relation to P’s. In a couple of cases, I have recommended publicising as much as possible in advance of the application to the court, such that “the cat is already out of the bag”, in terms of what is publicly available and a TO restrictive of their Art 10 rights is then less likely.
Public Observers
35. Most public observers (who are not journalists) have no idea that they can ask for a variation in the TO (or feel confident to do so, given that they have a very hazy idea of what the TO actually means anyway). I’m not aware of anyone except me who has done so.
36. It is exceptionally rare for me to be treated by judges, in the course of a hearing, as someone with Article 10 rights who might wish to vary the TO. This is not provided for in the Transparency Pilot rules (I’m not sure whether it was even considered?). I am regularly asked whether I have received the TO and sometimes whether I have understood it, but not whether I have concerns about it. Since I only receive the TO around 50% of the time (often after the hearing), it’s difficult for me to make any sensible interventions on behalf of my Article 10 rights anyway. The only journalist who regularly attends COP hearings (albeit almost exclusively those in the Royal Courts of Justice and not in the county courts) is Brian Farmer of the Press Association and I’ve noticed that he also finds it very difficult to intervene: I often observe him switching on his camera, or standing up in court towards the end of a hearing to say: “I’m sorry to interrupt the proceedings but…” Some judges are more open to inviting a contribution from journalists than others (Hayden J, Theis, J, Francis J, Poole J and Keehan J in particular, Brian Farmer tells me) – and Hayden J, Poole J, Roberts J and a handful of other judges (including District Judges and Circuit Judges in the county courts) have supported contributions from me about transparency matters when I have been able to indicate that I wish to make them.
37. I do sometimes have Article 10 concerns which I’ve been unable to address. For example, I’ve sometimes been told that a “standard” TO is in place, only subsequently to receive something like [316] below, which prevents me from identifying a public body (the Local Authority). But by then the hearing was over and there was no opportunity to ask why, or to ask for it to be varied.
I was told in court that the TO was “the standard order in the standard terms” but when I received it, it prevented identification of the Local Authority. Since the hearing was over by then, I was not able to clarify this. [357]
38. When I have Article 10 concerns about a TO and have received it before the end of the hearing, I have usually found it most efficient (in remote hearings) to write an email to the judge and send it via whoever I have an address for who can pass it on (the judge’s clerk; counsel; whoever sent me the video link). In person, I have simply raised my hand and asked for permission to address the court. I have written blogs about some of these concerns: they have all been carefully considered by judges and resulted in variations to the TO in every case. This suggests that a member of the public (who is not a journalist) can play a part in ensuring the transparency of the court when given the opportunity to do so.
TRANSPARENCY ORDERS ARE OFTEN NOT SENT TO MEMBERS OF THE PUBLIC – RENDERING ‘ANXIOUS SCRUTINY’ OTIOSE
39. I only ever receive TOs (or written RROs) for about 50% of hearings. Of the last 50, I have no record of having received a written reporting restrictions order for the following (public) hearings: [317] [318] [319] [320] [322] [323] [325][329] [330] 336] [337] [340] [342] [344] [346] [349] [353] [354] [355] [358][8]
40. In one of these hearings [319], my contemporaneous notes record that the judge asked about TO at the beginning of the hearing, saying there was “added complexity because of concurrent care proceedings and other young people whose confidentiality needs to be respected.” But I have no record of having received the TO.
41. At some of these hearings (e.g. [320] [349]) the judge made explicit requests for TOs to be sent to observers, but we have no record of receiving them. For example, neither I, nor another observer (Paige Taylor, a Bar course student) who blogged about this hearing, ever received a TO for [320]. She describes what happened in her blog post:
I hadn’t received a TO for [318] and checked with another observer, Mollie Heywood who observed a subsequent hearing in the same case She says: “I’ve never had a TO for anything I’ve observed sent to me! They read out instructions but that’s it…. I’ve seen about five [hearings] or so” (Mollie Hayward, social worker + law student).
One observer has watched 9 hearings and received only 3 TOs (and one of those came via me) – see Upeka de Silva, Policy Officer or Compassion in Dying, Appendix 2A.
Another observer, Georgina Baidoun, former lay COP Deputy, tells me she has observed 10 hearings but received only 4 TOs.
A member of the core Open Justice Court of Protection Project group has gone systematically through the 38 hearings (across 32 cases) that she’s observed. She has 14 TOs (=38%) – see Claire Martin Appendix 2B.
43. It does not seem to be anyone’s (agreed) job to send TOs to observers. When I’ve asked about this, I’ve generally been told that court staff should send them (e.g. ““It is not Counsel’s role to provide orders. This is an HMCTS role.”, HHJ Hilder, Item 8 Minutes of COP User Group meeting, 20 April 2022), but when I’ve asked court staff, I rarely get them (either there’s no response, or I’m advised to ask the judge). In practice, I mostly receive TOs from counsel.
44. Judges sometimes seem content to provide simply verbal summaries of reporting restrictions, followed by the request to “contact the court if you need a copy of the order” (Theis, J [337]) or “if you want a copy you can ask” [Theis, J [347]). One judge ran through the TO – she said it was “in the usual terms, nothing to identify [P], her family or where she lives – that would be contempt of court” and seemed surprised – when she offered me the opportunity to address her – by my request for a TO (‘You are keeping me on my toes’) [327]. Mostly I don’t get an opportunity to address the judge, so cannot make this request.
45. The problem with relying on oral summaries from the judge about what the TO says is that these summaries are often incorrect. For example:
On discovering that no TO had been prepared, the judge said: “you’re welcome to observe but the identity of the parties to the proceedings must remain confidential”. She checked with the advocates whether they were content to go ahead on that basis. Francis Hoar (counsel) provided a slightly different version of the TO: “You cannot report anything that may risk identifying any of their parties, or where they live, or who they associate with”. (The addition of “who they associate with” was new to me.) The judge asked the observers if we understood, so I was at that point able to ask whether we could identify public bodies, since they were also ‘parties’ to the proceedings. The judge said: “Yes, I meant the family. Not the public bodies. I think I need a pro-forma I can read out in these situations”. When I eventually received the TO, it prohibited identification of the CCG. I am unclear whether or not what the judge said in court means that she varied the pre-existing TO (made by HHJ Owens on 23rd April 2021). I’m not sure she meant to. [364]
46. Most members of the public who receive only oral summaries relating to reporting restrictions (whether these are framed as TOs or RROs, the latter of which are overwhelmingly oral only) do not feel confident to write blog posts about the hearing because they are not sure what the judge said they could and couldn’t report (or – wrongly – believe that there is nothing at all they are allowed to report). Not sending out TOs has a chilling effect on transparency.
47. In my experience, written versions of TOs (and RROs) are not sent to observers for the following reasons:
there is still some confusion between TOs and “Remote Hearings Order” (even though more recently they are sometimes combined). I was sent RHOs for [317] and [353]. These did not include anything equivalent to “the subject matter of the injunction”.
nobody knows how to separate out the TO from the rest of the electronic bundle
counsel have the TO, but not the observers’ email addresses
court staff have the observers’ email addresses, but not the TO
it’s not clear whose job it is (if anyone’s) to send out TOs – sometimes I’m asked to circulate to other observers
48. Repeated requests for TOs are sometimes unsuccessful. For example:
“What sounded like a standard ‘warning’ was read out at the beginning of the hearing, informing me that publishing “the Information” prohibited by the TO could lead to me being sent to prison or having my assets seized etc. Nothing at all was said at any point during this hearing about what “the Information” was. Nor had I been sent a TO nor was there any attempt to send me a TO during the course of the hearing. I pursued the TO after the hearing, including via the court staff (on 21/8/22) and then via one of the barristers in the hearing (on 27/8/22) and finally by emailing the court address with an email for the attention of HHJ Howells herself. On 8/9/22, I receive an email from a Court of Protection Clerk at Cardiff COP saying “Please see attached 2x transparency orders for the hearings that you observed on 19th August”. Two documents were attached. One was a TO for the 9am hearing (which I had already received). The other was a Remote Hearings Order (not a TO) for the 11am hearing (COP 13802410). It contains NO REFERENCE to “the Information” I am not allowed to publish (i.e. it is not a combined RRO and TO). I still do not have a Transparency Order for this hearing.” [353]
49. My impression is that I am less likely to receive a TO if the judge requires amendments to the draft order (or to the order approved by the previous judge).
50. For example:
I never received a TO for the case before Lieven J on 27 January 2021 (COP 13703893). My contemporaneous notes from that hearing record that the judge referred at the beginning of the hearing to the draft TO and said she could see no reason for anonymising the hospital or the treating clinicians – and in fact she then referred to the clinicians by name in the published judgment. It subsequently transpired that the amendments had never been made – leading to considerable confusion for the BBC (and the court) in their application to name P a year and a half later, since there was a discrepancy between the still-extant TO (which said the treating clinicians could not be named) and the published judgment, which named them. The judge (Francis J) hearing the case brought by the BBC ruled that they could not now be named and ordered that Lieven J’s judgment should be taken down and redacted to remove the names of the treating clinicians (see BAILII (The Newcastle Upon Tyne Hospitals NHS Foundation Trust v Bourn (Rev1) [2021] EWCOP 11). For reasons not discussed in court, the name of the independent expert was also redacted. A temporary restriction on publishing anything about the case was imposed until the redacted judgment was in place. This whole process of seeking a variation to the TO was messier and more complicated than it need have been had the judicially approved version of the TO been available in the first place. (I blogged about the hearing: Medical treatment for people with learning disabilities: Telling Robert Bourn’s story and the challenges of ‘transparency’.)
51. I have emails from counsel in other cases saying that they will send me the revised TO once they have made the revisions and the judge has approved them – but then there is no record that I’ve ever received these revised TOs.
REPORTING RESTRICTION PROCEDURES ARE NOT WORKING WELL
52. In sum, there is strong evidence that the current procedures in place with the aim of protecting P’s privacy while at the same time protecting the public’s right to freedom of information and freedom of expression are not working well. I understand that, following the concerns expressed by Mostyn in Re EM [2022] EWCOP 31, aspects of TOs are being reviewed by the Rules Committee. Pragmatically, requiring a full-scale Re S analysis and notification of the press before any Transparency Order is made would cause a level of delay and complexity that would be impossible to manage – but it would be worth exploring how to address the current problems created by reporting restrictions and to build in mechanisms to allow the court more effectively to address the concerns participants (including family members) and observers often have about the way things are working (and failing to work) at present.
STATEMENT OF TRUTH
I believe that the facts stated in this witness statement are true. I understand that proceedings for contempt of Court may be brought against anyone who makes, or causes to be made a false statement in a document verified by a statement of truth without an honest belief in its truth
Celia Kitzinger
Dated 21st October 2022
Appendix 1. List of hearings 50 most recently observed hearings (on 10 October 2022)
by Celia Kitzinger in date order.
Ref. CASE NO. DATE JUDGE TO?
[314] COP 13755775 (29.04.22) Cobb J RCJ Y
[315] COP 13744224 (03.05.22) DJ Beckley FAH N (Private)
[316] COP 13801482 (04.05.22) DJ Woodburn Bristol Y
[317] COP 13053463 (17.05.22) DJ Porter-Bryant Cardiff N
[318] COP 13861341 (08.05.22) Francis J RCJ N
[319] COP 13630800 (20.05.22) HHJ Edwards Cardiff N
[320] COP 13585739 (23.05.22) Lieven, J N
[321] COP 1388671T (23.05.22) DJ Birk Y
[322] COP 1378613T (24.05.22) Moor J RCJ N
[323] COP 13930317 (25.05.22) MacDonald J RCJ N
[324] COP 1393210T (07.05.22) DJ Charnock-Neal Newcastle Y
[325] COP 13776756 (13.05.22) DJ Keller Cardiff N
[326] COP 13744224 (30.05.22) DJ Beckley FAH N (Private)
[327] COP 13899903 (07.06.22) HHJ Hildyard Reading Y
[328] COP 13719647 (09.06.22) DJ Searl Newcastle Y
Reference made to TO, but not sent to me (not sure I requested). Mungo Wenban-Smith mentioned the ‘previous draft order on 9 March included a TO regarding anonymity. Said the aim was to ‘preserve the anonymity of CD’. The judge (Williams J) reinforced that P would be referred to by name during the hearing and that ‘others’ must adhere to the TO, and added that in the TO it also says family members’ names also not to be disclosed.
[2] Lieven J said ‘TO will be sent. Nobody is to publish information that could lead to the identification of the claimant or P’. Did not receive TO.
[3] From my notes: HHJ Hilder – I had to confirm that I understood the hearing was in private and I could not identify anything about P etc.
[4] From my notes: Judge mentioned observers – “welcome of course, but may I say … the court office is only open from 9-5 and communications received outside of those hours … a lot for staff to do… so Dr M if you wd be kind enough the earlier you can give notice the easier it will be.” Asked if I had received the TO [No] – asked for ‘someone’ to send it to me. Never rec’d. No summary. Don’t know who respondents are …..
[2] The Family Procedure Rule 27.11 (which applies only to private proceedings in the Family courts, and not to the Court of Protection) permits observation and blogging from “legal bloggers”, defined as “duly authorised lawyers” who meet the criteria specified in Practice Direction 27B.
[7] Numbers in square brackets refer to the number I’ve given the 50 court hearings I’ve observed, listed in Appendix 1.
[8] In preparing this witness statement, I have searched through my emails for the TOs missing from my files using (a) the case number; (b) the date of the hearing; (c) the names of counsel. It is just possible that I have in fact been sent TOs for one or more of these hearings but, if so, I have been unable to locate them.
John (not his real name) is 17 and will be 18 in three months’ time. He used to live with his adoptive mother but (since 2021) has been living in a Gateshead Local Authority placement where he is supervised 2:1 by carers.
I didn’t find out anything about John’s difficulties or diagnoses during the hearing (but filled in some gaps in my understanding when I read the Position Statement from the OS) other than that he can present with ‘challenging behaviour’, but he is said to be very happy at his home. He has to move out though, because the home is for children and he will become an adult soon.
This case (COP 14067800) has been before the Court of Protection since 12th May 2023, but the first hearing I observed (remotely) was before HHJ Burrows on 17th August 2023. This is how it was listed.
It was a case management hearing, which means current issues are reviewed, parties’ positions are submitted to the judge, orders are made and plans for future or final hearings are decided.
A Note on Accessing the Court
This was one of the best organised hearings I have observed. HHJ Burrows was sitting at First Avenue House, the home of the Court of Protection, in London. The hearing was remote, via MS Teams at 10am. I received the link, and the Transparency Order, at 9.40am.
Both counsel (Sophie Hurst for John, via his Litigation Friend the Official Solicitor; and Stephen Williams for Gateshead Council) were on the link when I was admitted. The court clerk checked with counsel whether any other people were expected (John’s Social Worker joined by telephone some time later) and then checked that I could hear and that I had received the Transparency Order. He said the judge had asked whether I wished to stay on for his 11am hearing. I couldn’t stay on as I had a prior commitment, though I was pleased to have been asked.
John
When HHJ Burrows joined the video-platform, he checked with counsel whether others would be joining and then said: “Dr Martin is very welcome to join us. I haven’t received a Position Statement from the Local Authority. I have one from Ms Hurst. …. For my benefit and also for Dr Martin please outline what this case is about”.
Counsel for the local authority explained:
“This case concerns [John] a 17-year-old, 18 on [X December 2023]. He was previously living with his adoptive parents and then due to […] rising aggression and behaviours […] he was detained under Section 2 of the Mental Health Act and then in March 2021 detained under Section 3. Care proceedings in 2021 resulted in [John] residing in his current placement – he is the sole resident at the placement since 2021, [which is] a registered children’s home. The Local Authority has blocked out the other vacancies – it can cater for 3 or 4 [children] – but he’s the sole resident presently. He turns 18 in December. He will need to leave then or shortly thereafter. I have been informed that he can remain for a very short period of time, but the Local Authority is taking steps to identify a placement for him before he turns 18. He is supervised 2:1 in the current placement and to and from school. He attends year 13 [and] he’ll be there until 2024, July. [He has] reduced supervision of 1:1 […] staff have had to restrain him on occasion […] they are trained in NAPPI training […] have had to administer PRN [‘as needed’] Methazine medications. He is restricted in using computer equipment, to aid good sleep and a good routine. There are restrictions in place, the doors and windows are locked.”
Counsel for John via the Official Solicitor helpfully sought permission to share her client’s Position Statement with me, which has enhanced my understanding of John’s needs. Counsel for the local authority likewise sought permission to share their Position Statement, but I have not received it to date.
John has a condition called Fragile X of a type that is associated with learning disability, ADHD and global developmental delay. He has been deprived of his liberty since December 2021, when he first moved from living with his adoptive mother, and a care order was made for him to live in his current home. By all accounts (according to his counsel), John likes living where he is, is very sociable, gets on well with his carers and is happy and settled. This was clearly important, given that John’s life will be changed completely not long after he turns 18.
What was the court being asked to do?
It wasn’t clear to me at first what the court was being asked to consider. HHJ Burrows needed to clarify this point:
Judge: [to Stephen Williams, counsel for LA] What are you asking the court to do?
Counsel for the LA described issues to do with identifying an appropriate place for John to move to.
Judge: Does he have to leave the placement when he’s 18?
Counsel for LA: There is no issue in terms of registration. […] The Local Authority is effectively booking out the entire placement, which could cater for more than one resident. Equally, and more importantly, the Local Authority acknowledges that remaining in a children’s placement is not in [John’s] best interests in the long term. We are taking appropriate steps to identify properties.
So, it seemed the main issue, from the Local Authority’s perspective, was finding somewhere for John to live. All parties agreed that John lacked capacity to make this decision himself, as well as decisions about his care needs. However, the Official Solicitor requested that the Local Authority provide capacity assessments for financial decisions (John’s mother currently acts as appointee, but wishes to be removed from this role), as well as use of social media and the internet (which are subject to restrictions in John’s care plan).
John’s Mother
I was wondering why, given that she had been mentioned a few times, John’s mother was not at the hearing, or a party to proceedings. HHJ Burrows asked about this during the hearing:
Judge: [John’s] mother is not present today and you said she’s not indicated a wish to be involved in proceedings. How much has she been involved in the early stages of the planning? Counsel for the LA: I don’t have instructions on that … [he passed the query to John’s Social Worker, who had joined the hearing by telephone] Social Worker: My understanding is that she DOES want to be involved in all aspects of planning and I thought she would be joining today. Judge: Have efforts been made to involve her? Social Worker: I was in touch with her last week. Apologies if that hasn’t filtered through. Judge: I am rather glad now that I didn’t just make the order in the absence of a hearing. It’s vital that this lady is involved, not only in care planning but in these proceedings and she needs to know about these things for his future life. I am surprised she’s not here. This is perhaps an oversight by somebody who should have put her in touch. Let’s carry on and see where we get to.
Counsel for the LA later addressed the lack of planning to ensure John’s mother was part of the court process. He said that ‘urgent enquiries’ would be made of John’s mother, ‘as to whether she wishes to be a party’. I thought that HHJ Burrows’ response to this was heartening:
Judge: I’m not talking about her being a party [….] obviously we can consider that, but she obviously wants to be involved. It’s very common for parents and close relatives having access to all of the papers and having access to me, as if she were a party. Sometimes parents are a bit cautious about the court, as if we are adjudicating about their parenting. She’s been through care proceedings which must be AWFUL and I want her reassured that the purpose is not to judge her and we will benefit from her knowledge and experience. [Judge’s emphasis]
Counsel for the LA: Yes, we will contact her. You will see she’s submitted evidence.
Judge: Yes I have read it.
Counsel for the LA: You have my apologies that I haven’t granted her permission to submit [further statements.] I would suggest giving her two weeks to respond [about proposed properties for John to move to].
Judge: No doubt the Official Solicitor will wish to respond, but they will wish to see what the mother has to say. When you say ‘statement’ it can just be a letter to me, it doesn’t have to be formal, if she wants to talk to me at the hearing that is fine. I want to make it more user-friendly for someone who might be intimidated by the court.
That felt like a breath of fresh air. I wondered how many other parents and relatives are afforded this sort of compassionate understanding of what it’s like to be faced with engaging with the judicial system, and efforts made to adjust the ‘intimidating’ processes and etiquette.
Capacity for Sex
A brief but interesting discussion took place about John’s age, sexual development, current situation and decision-making capacity in relation to sex.
Counsel for the Local Authority was discussing the ‘PBS Plan’ [Positive Behaviour Support Plan] in relation to John’s ongoing care needs. His current plan was devised in 2021, by CYPS (NHS Children’s & Young People’s Service).
Counsel for LA: CYPS will confirm with [care provider] that the plan is sufficient and whether the school [has addressed] sexual relationships, he has had some….
Judge:What? Sexual relationships?
Counsel for LA: No apologies. Education about this. He’ll be 18, he’s looking forward to going to clubs and bars, ‘picking up chicks’ in his language….
Judge: Is there evidence he doesn’t have capacity for sexual relationships?
Counsel for LA: It’s not yet assessed. There’s no suggestion of an assessment about capacity for this yet [this was also agreed by the Official Solicitor]. We are more looking to see what the school can provide, and also to see if he is even indicating an interest in this …. [Counsel’s emphasis]
Judge: But presumably it’s an important part of care planning. He’s expressing an interest in women … he may want to have sex with a woman today. What would you do? [Judge’s emphasis]
Counsel for LA: Well, it’s not been expressed as present. It’s been described as bravado. He’s expressed a wish to meet girls. The Local Authority is keeping it under close review.
Judge: Yes, but he’s entirely under the care of the Local Authority and any development needs to be [….] sexual relationships should be moving towards the top, if not occupying the top, of the agenda.
I was thinking the same thing, really. The judge was anticipating a situation that could change rapidly. It didn’t sound as if the Local Authority knew what sexual and relationship education John had received, yet he was talking about going to clubs and ‘picking up chicks’. An aspect of life that is not restricted for John is contact with others (confirmed by the Official Solicitor’s Position Statement).
Counsel for John later addressed this issue in her submissions:
“Sexual relationships. This something we sought to explore in the round table meeting, given he is interested. On exploring further, we were told he has never acted on any comments – he has a favourite character in Coronation Street who says things like this [‘picking up chicks’]. We understand his needs are more sensory than looking for a partner. We understand that this is to be kept under review, see what happens over the next year. It isn’t the case he hasn’t had the opportunity to explore this if he wants to – he’s a very social young man. The Official Solicitor is satisfied about the plan over the next year.”
Both the Local Authority and Official Solicitor are therefore in agreement that a capacity assessment for sexual relations is not currently needed and will be kept under review.
The Outcome
HHJ Burrows invited final submissions from both counsel and asked whether (by the end of November) the court would ‘likely be in a position to formulate, approve or see enactment of a transition plan?’.
The Occupational Therapist is visiting potential properties and will whittle this down to two or three appropriate places, which John will then be invited to visit. A statement of John’s wishes and feelings will be drawn up for the court. Then there will be a further (remote) hearing, with HHJ Burrows who will be sitting in Manchester, on 30th November at 10am to decide whether further evidence is needed.
I had received the Transparency Order (which is the court injunction stipulating what can and cannot be reported) and it did indeed prevent identifying where John lives – but not (explicitly) the name of the local authority.
The public listing – see the start of this blogpost – for this case had named Gateshead Council (which is why I was interested in observing the hearing, because I work in Gateshead).
HHJ Burrows took the bull by the horns (for which I felt very relieved):
“The second question – to both of you [counsel] – the Local Authority is identified in the list. We have an observer today – I can see no conceivable reason she should be prohibited from mentioning that Gateshead is the applicant in this case. There’s no reason for that is there?”
Counsel for LA: I have no instructions otherwise.
Judge:It’s on the public list. The horse has bolted in this case. For Dr Martin’s benefit, there is controversy at the moment about identifying public bodies. I can see no reason why not to identify in this case.
The judge asked that he receive the Order ‘by tomorrow please’.
And that was the end of what was a very efficient (44 minutes’ long), and very human hearing, which (although I did not – yet – learn a great deal about John as a person or his wishes and feelings) did keep ‘P’, and his mother, at the centre of the court’s focus. I formed the impression that this was entirely because HHJ Burrows made sure of it.
Claire Martin is a Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a member of the core group of the Open Justice Court of Protection Project and has published several blog posts for the Project about hearings she’s observed (e.g. here and here). She tweets @DocCMartin
The focus of many Court of Protection cases is where someone will live, what care and support they will receive, or what medical treatment they should be provided. Once that substantive decision has been made, the Court’s attention will often turn to what is described as “conveyance planning”.
A “conveyance plan” is, in the simplest sense, a plan which provides how a person will get from one place to another. However, conveyance is often one of the most complex areas legally and logistically in a case.
Sometimes “conveyance plans” are an integral part of a “transition plan”. The two terms are often used interchangeably but that misunderstands the difference between the two things. A “transition plan” is not simply about how somebody gets somewhere (that is conveyance). Rather, a “transition plan” should be focused on how P’s care, support or treatment will be delivered in a different setting. The idea behind transition planning is that P is not overly impacted by a sudden change of surroundings or care/treating team.
There are some examples of cases involving conveyance issues which can be found on the Open Justice Court of Protection Blog:
The legal challenges in respect of conveyance planning
Sometimes a conveyance plan is simply presented as a logistical nicety. That fundamentally ignores the legal complexity which is involved and often indicates a misunderstanding of core aspects of the Mental Capacity Act 2005 (and other statutory frameworks).
There are three legal issues that frequently arise in cases involving conveyance planning:
Powers of entry. Lawful entry into a person’s home is strictly limited by statute, even in circumstances where a person lacks the mental capacity to make certain decisions for themselves. There is no power of entry contained within the Care Act 2014, and this was a conscious decision on the part of Parliament. There is no explicit power of entry contained within the Mental Capacity Act 2005. However, a court may authorise entry using the provisions contained with sections 15 and 16 of the Act. In some cases, public bodies have argued that entry should be secured using section 135 of the Mental Health Act 1983, put simply, that approach is unlikely to be necessary in the context of Court of Protection cases. Nor should public bodies expect the police to use powers under section 17(1)(e) of the Police and Criminal Evidence Act 1984 to secure entry to a private property save in emergency circumstances.
Who is responsible for conveyance? One of the most surprising debates that has become common in complex conveyance cases is who is responsible for arranging the conveyance. Likewise, there is sometimes a presumption that the police will assist in respect of conveyance when no such obligation exists in law. It is impossible to distil a universal rule as to who is responsible for organising the conveyance, but the basic principle is that it will fall on the party seeking the order.
Restraint. In too many cases, conveyance has taken place without any authorisation of the deprivation of liberty which arises from the conveyance arrangements. Active thought needs to be given to whether the proposed restraint will go beyond the parameters set out in sections 5 and 6 Mental Capacity Act 2005 and amount to a deprivation of liberty?
What a good conveyance plan looks like
In my experience, good conveyance plans consider the following issues:
P: Who is P, what is their prior experience of medical treatment, what are their future needs likely to be, how can we prevent their needs intensifying? What does P want?
Property: Where does P live? How do we extract them from that property? What is our lawful ability to enter? How do we physically enter?
People: Who do we need to be part of the conveyance? Is this a case where we need to use sedation (or even general anesthesia) in someone’s living room, or is it a case where P will be driven to hospital in a family member’s car? Do we need other parties (perhaps a fifth P) to be involved?
Passing it on: Who do we need to share P’s experience with for the future? What can we learn from this case that we can pass on so that other professionals might learn from it?
Failures in conveyance planning have consequences
Conveyance planning is not a luxury or a nicety. It is a means of properly protecting P’s rights and sometimes protecting them from harm. The failure to properly plan someone being conveyed to hospital can imperil their physical health. Shortcomings in planning how P will be extracted from an address can cause them to be subject to excessive physical restraint or to be injured during their extraction. Ultimately, conveyance plans that don’t properly consider P’s experience, may have longstanding implications for their care and treatment: they may become fearful of hospital or changes in care settings.
A considered conveyance plan is positive for all involved. In the most basic sense, it avoids the risk of something going wrong during the transfer of location. But it also can give the change of location or care/treatment arrangements the best chance of success. The most human way of explaining this is our own experience of travel: we are always much happier when we reach our destination if we have had a positive journey without delays, lost luggage and plenty of opportunities to use the loo, to eat and drink.
Ian Brownhill is a barrister at 39 Essex Chambers and HM Assistant Coroner for Kent. Ian tweets @CounselTweets and is a member of the Advisory Team for the Open Justice Court of Protection Project.
Drawing on my experience with the Open Justice Court of Protection Project – and with some helpful input from other core team members – I submitted my views about open justice to the Ministry of Justice consultation, just before the deadline at 11.59 on 7th September 2023. I’ve reproduced what I sent below (with typos corrected- why do I only see those after pressing ‘send’?).
As I think is clear from the document itself, I’m slightly embarrassed about the very basic nature of my suggestions for “the way forward”. The twenty Key Performance Indicators (KPIs) I’ve developed to assess whether or not the Court of Protection is meeting the requirements of open justice seem to me to be entirely self-evident – as I expect they are for anyone who reads the document. It’s awkward to have to spell them out because obviously the Ministry of Justice must already know that open justice requires that the public is informed about hearings – including when and where they’re taking place, and what the hearing is about; that it must include making clear that we can observe a hearing and how (remotely or in person); that it’s necessary to tell us how to contact the court for information or to obtain a video-link for remote hearings. But those requirements (KPIs 1-5) often aren’t met – so until they are, it does actually seem necessary to keep mentioning them in any plan for “the way forward”. Equally, it’s really obvious that court staff should be able to tell us what courtroom a hearing is in (but in practice they often can’t) and that there shouldn’t be a big sign on the courtroom door saying “PRIVATE” when the hearing isn’t intended to be private (but in practice these signs are common) (KPIs 9 and 10). It’s also glaringly obvious that open justice is defeated if nobody replies, in a timely manner, to our emails requesting remote access (KPI 13): but that too is a daily experience. Since these are the daily barriers we confront in seeking to observe court hearings, that’s what I’ve written about.
The ‘categories’ of response (as organised by the main content headings) are as prescribed by the “Call for Evidence”. Questions were grouped together under these category headings. Under each category heading, I’ve often addressed the broader issue instead of, or in addition to, the specific questions posed – but where what I wanted to say was a direct response to one of the questions, I’ve reproduced the questions from the “Call for Evidence’, in red, as a subheading. (Note, I’ve used the question numbers as assigned in the “Call for Evidence”, so they are not numbered consecutively in this document.)
I look forward to seeing what evidence has been contributed by other people and to the outcome of the consultation.
**********
Open Justice – The Way Forward
Response to Call for Evidence
Celia Kitzinger, 7 September 2023
Index to contents
About the Open Justice Court of Protection Project
Questions on open justice
Listings
Accessing courts and tribunals
Remote observation and live-streaming
Public access to judgments
Access to court documents
Public legal education
Closing Summary
A. About the Open Justice Court of Protection Project
The Open Justice Court of Protection Project (OJCOP) is an unfunded voluntary project, independent of any public body, initially launched by Celia Kitzinger and Gillian Loomes-Quinn on 15th June 2020 with the aim of encouraging members of the public to observe Court of Protection (COP) hearings and to blog about them.
As a direct consequence of our Project, thousands of people have observed COP hearings over the last 3 years and several hundred people have contributed blog posts reflecting on the experience.
The Project does not seek to promote a particular perspective on the Court of Protection, but through its work aims to give people the information they need to access court hearings, to read about court hearings observed by others, and to form their own views (see our Project policy, available as a downloadable pdf from our “About the Project” webpage).
The current Project team has five core members – none of us lawyers or journalists:
Celia Kitzinger, retired academic
Gill Loomes-Quinn, disability rights scholar-activist
We are supported by an Advisory Group composed of two COP barristers (Victoria Butler-Cole KC and Ian Brownhill) and a COP solicitor (Kirsty Stuart). For more information see our “Meet the Team” webpage.
The Project was launched as a direct response to the exigencies of the COVID-19 pandemic. With the first announcement of restrictions on contact, the (then) Vice President of the Court of Protection, Mr Justice Hayden, closed down access to the physical courtroom and directed that all COP hearings should be heard remotely unless there was a “genuine urgency” and it was “not possible to conduct a remote hearing”. He also said that Practice Direction 4C (permitting the attendance of members of the public and journalists) was “unworkable at present” and disapplied it (“Remote Access to the Court of Protection Guidance”, 31st March 2020). We saw the move to remote hearings as posing a direct threat to transparency and open justice in the Court of Protection.
Access to members of the public (and journalists) had previously been permitted by virtue of the Court of Protection’s own “Transparency Pilot”, initiated four years earlier, in 2016. Having previously held almost all hearings in private (“serious medical treatment” hearings were a significant exception), the “Transparency Pilot” created a situation where hearings were, by default and unless otherwise directed, open to members of the public (and journalists). We could observe hearings, and write about them, subject to reporting restrictions (known as “Transparency Orders”) – usually limited to anything identifying the vulnerable person at the centre of the case (commonly known as “P” for “protected party”) or their family, and where they live. The Pilot was subsequently integrated into ordinary Court of Protection practice – with all hearings listed as “Public” by default. By the beginning of the COVID-19 pandemic, both Gillian Loomes-Quinn and I had observed dozens of Court of Protection hearings, and published material about them (including live-tweeting a Court of Protection hearing back in 2017).[1]
The public nature of Court of Protection proceedings was effectively reversed at the beginning of the pandemic. Although the (then) Vice President had stated that “In each case active consideration must be given as to whether any part of any remote hearing can facilitate the attendance of the public, if so Practice Direction 4C may be applied and the transparency order reissued” (§59 (“Remote Access to the Court of Protection Guidance”, 31st March 2020), there was very little evidence of any such consideration in practice. All remote hearings were now listed as “Private”, albeit with a footnote stating that we could nonetheless apply to observe them via video-link or telephone conference call. We quickly discovered that most such applications were unsuccessful. Either we were told that we couldn’t be sent the link because the hearing was “private”, or we simply got no response to our enquiries. The threat to transparency was real and obvious.
It did not occur to us to “ask permission” of anyone to create our Project and we chose not to apply for funding since we wanted to remain independent of any particular backers. We simply came up with a Project name, created a social media presence for it and started to provide information about upcoming hearings via our website, our Twitter handle (@OpenJustice COP) and other social media. We also offered support, based on our own experience, to would-be observers seeking to navigate access. Those activities remain central to the Project.
From the outset, the uptake exceeded our expectations. Within the first two weeks after our website went live in June 2020, more than 70 people had contacted us for help with observing hearings and we’d published six blog posts by members of the public. By the end of the first year, we’d published 139 blog posts with 97 different authors, and today it’s nearly 400 blog posts, written by around 200 different authors. They’re written by social workers, best interests assessors, case managers, psychologists, nurses, doctors, midwives, medical ethicists, policy officers, academics, journalists, third-sector workers, law students, paralegals, lawyers, birth rights activists, a care worker, a speech and language therapist, a court interpreter, an intermediary, a police officer, school students wanting work experience in relation to medicine and law, and family members of potential or actual “P”s – and observers have watched remote hearings from Europe, Japan, and the USA (including this medical-ethicist blogger, Resolving End-of-Life Treatment Conflicts: Comparing the COP in England to Analogous Mechanisms in Ontario, California, and Texas). The Project has opened up public awareness of the Court of Protection as never before.
Today, despite the arguably ‘niche’ nature of our Project, we have nearly 6k followers on Twitter, and 233k unique visitors to our website from more than 150 countries. We’ve supported thousands of people to observe hearings – and I’ve personally observed more than 470 COP hearings in the Court of Protection since 1 May 2020 (most remote, around 15-20 in person).
The Court of Protection has been broadly positive about and supportive of our Project. The former Vice President, Hayden J, has said publicly that he is “very grateful” for the work that we do, and Poole J has said: “… the Open Justice Court of Protection Project is an important project that makes a significant contribution to transparency and public understanding of the workings of the Court of Protection” (§68, Re A[2022] EWCOP 44).
In responding to this Call for Evidence, I’ve answered those of your questions to which I feel I can best contribute – and my answers come directly from experience with the Open Justice Court of Protection Project, and are specific to it. Your questions are very broad and very ambitious. By contrast, the evidence I’m sending you is rooted in my ordinary everyday experience of observation in the Court of Protection at a hands-on level over more than three years and we have rather modest proposals for improving open justice (see our 20 Key Performance Indicators). I suspect they may sound rather mundane and prosaic – even as though I am labouring the self-evident. But what I have learnt over the last few years is that the high ideals and lofty principles of open justice depend upon – and can only be realised through – the ordinary, daily, taken-for-granted practices of the court. “Fine words butter no parsnips”. If I sound acerbic or frustrated at times, that is because I struggle, daily, to bridge the gap between the court’s stated commitment to transparency and its repetitive, predictable, seemingly intractable failures to achieve it. I am impressed with the level of commitment and hard work shown by judges and lawyers at all levels of the Court of Protection – but it is glaringly apparent that they are working within a system that doesn’t support them adequately. I agree with the view that “You have got to recognise the system is broken and needs to have proper financing’. Townend, J. and Prasad, A. (2023) Courts and Tribunals Access and Observation Workshop Report. Oxford: Sheila Kitzinger Programme, Green Templeton College, University of Oxford. Better resourcing is fundamental to promoting open justice and transparency in the justice system.
B. Questions on open justice
1/. Please explain what you think the principle of open justice means.
The principle of open justice means that the public (not just journalists or designated categories of accredited observers) should be able to observe hearings; that we should be able to communicate about what we’ve seen and heard in court, our views about it, and our experience of the justice system; and the principle best translates into practice as a collaborative – not a confrontational – enterprise. I expand on this below.
1.1 The public (not just journalists or designated categories of accredited observers) should be able to observe hearings
Open justice means that the public (not just journalists or designated categories of accredited observers) should be able to observe hearings. This is because there aren’t enough journalists covering court hearings, and because members of the public have both personal and professional investments in the Mental Capacity Act 2005 and in the Court of Protection, which journalists can’t be expected to address. Despite the claim that journalists are “the eyes and ears of the public”, there are, as evidenced below, significant differences between what journalists ‘see’, ‘hear’ and report about court hearings, and what members of the public ‘see’, ‘hear’ and report. Open justice requires that we have direct access to the court and are able to observe for ourselves the process whereby judges and lawyers are “doing justice” with our own eyes and our own ears.
Open justice is too important to delegate to journalists alone, for the following reasons.
(i) There aren’t enough journalists to cover all the hearings
There’s very rarely a journalist in court. The PA journalist Brian Farmer is the only member of the press who regularly attends COP hearings, and he virtually never attends hearings outside of the Royal Courts of Justice – which means that about 95% of COP hearings (held at First Avenue House or in regional courts across England and Wales) simply never have a journalist in attendance. If the public couldn’t attend either, there’d be nobody watching and ‘open justice’ would be simply an abstract ideal.
Unlike court journalists, the majority of the hearings I observe are hearings before district judges and circuit judges in regional courts. These hearings are often perceived as ‘routine’ or ‘mundane’ in their content: they rarely raise issues of life and death or novel points of law. But they do engage human rights principles (especially deprivation of liberty, and the right to private and family life) which are of fundamental importance to the people involved in them, and for all of us who might in future be “P” or members of P’s family in a Court of Protection hearing.
And even in the Royal Courts of Justice we’ve covered really important hearings that have never been reported by the press: for example Mr Justice Hayden’s criticism of the Royal Hospital for Neuro-disability in Putney, London for adopting an institutional “ethos” of care that appeared (in the hospital’s view) to trump the law, resulting in decision-making processes that were “both poor practice and ethically misconceived.” (“’Burdensome and futile’ treatment and dignity compromised: Poor practice at a leading UK hospital”).
There’s often a belief that as long as the courts are open to journalists, that’s sufficient for open justice: they can act as the ‘eyes and ears of the public’. But in practice, our experience is that the direction of information flow is often from us to journalists, rather than the other way around – with some journalists asking me to alert them to any “good cases” coming up in court. We’ve supported journalists by advising them of hearings, helping them to navigating the tricky business of access to the remote court, and explaining the way the reporting restrictions work. It turns out, in many cases, that it is us members of the public (and not journalists) who have the relevant knowledge and expertise!
Dependence on journalists alone to report on Court of Protection matters would radically reduce coverage.
(ii) Many members of the public have intense personal/ family interests in Court of Protection matters and it is of benefit to them – and to their appreciation of and ability to participate in the justice system – to be able to observe hearings.
We’ve been contacted by many people wanting to observe COP hearings in preparation for a forthcoming hearing of their own – as well as by people wanting us to observe their own upcoming hearings, in the belief that having observers present will mean that the judge is more likely behave “fairly”.
Watching (other people’s) hearings in preparation for an upcoming COP hearing can educate and reassure family members.
“… it was very useful for me as a litigant in person in my mother’s case, to see how a hearing proceeds and the efforts of the judge to be fair and even-handed with someone presenting their own case for a family member.” (Anna, daughter of a P in a s.21A case)
“The law enabled a person with a learning disability to access the same rights and healthcare as any other citizen. This gives me a huge sense of relief that my family member will be safe and listened to with these structures in place, and free to live the life he chooses.” (NB, Full time carer)
Watching (other people’s) hearings after a challenging personal encounter with the Court can also help people to figure out what might have gone wrong.
“Having acted as Court of Protection Deputy for my mother’s Property and Financial Affairs, and having been threatened by the Public Guardian with my removal (otherwise known as ‘discharge’), I decided to ask to observe this case…. Speaking from my own experience, I now realize that, when I started what seemed to be merely a bureaucratic exercise of the sort with which we are all familiar (tax matters, planning applications etc), I was in fact already in the foothills of fully fledged court proceedings that could seamlessly lead to actual court hearings. One thing I, and I believe the applicant here, did not understand is that you cannot simply inform the court that you want to desist with your application; you have to make a formal application to withdraw it. In my case, my application to withdraw was refused and I was at a complete loss as to why. I now realize that at least part of the reason might have concerned costs, as it did here.” (Georgina Baidoun, lay COP deputy for Finance for her mother)
There is no way that a journalist’s account of what happened in court could achieve the targeted personal effects described here. For people with personal/family involvements in the COP, there is no substitute for this direct, first-hand experience of observing the Court of Protection in action.
(iii) Many members of the public work professionally with the Mental Capacity Act 2005. Direct observation of hearings improves their understanding of how the statute applies in action
“I have found the whole observation experience very beneficial. The googling, looking up of legislation, reading up of quoted case law – both during and after the court attendance – has given me a crash course in legislation, that I now realise, I only thought I understood. Listening to a talk about how the Mental Capacity Act is implemented in the courts is one thing – actually observing it as it happens is very different!” (Louise Burrell, social worker)
“I think the most important learning for me from being able to observe this hearing, is the way it has again, allowed me to watch the Mental Capacity Act 2005 ‘in action’ and understand how a senior High Court Judge … works through the process of reaching a best interests decision. I’m also able to take away with me some ideas that I can incorporate into my own practice when completing best interests assessments myself in future.” (Astral Heaven, DOLS Manager)
“My overall experience at the hearing was incredible. It made me rethink how I viewed ethics and its involvement in medicine. Now I will embark on my medical career with a better understanding of what ‘best interests’ means in practice. Doctors, much like the judge and barristers I observed, have the responsibility to protect vulnerable people in society, and I learnt that prioritising their wishes, beliefs and values before your own opinion is the only way to ensure this protection.” (Eloise Crang, aspiring medical student)
“For my part, I left [the hearing] with a resolution to examine my own practice, and to consider deeply the motivations for the clinical decision-making forums (e.g. Multidisciplinary Team Meetings) I am part of that do not physically place the person or their family at their centre.” (Caroline Barry, Consultant in Palliative Care)
“As a consultant for Lasting Power of Attorney and an Advocate for Advance Care Planning, learning more about the Court of Protection work and processes is important to me. I have attended previous hearings and found the experiences invaluable… I left the hearing with greater confidence in how to navigate the system, but more importantly, with great respect for seeing compassion in action.”Clare Fuller (Speak for Me consultancy)
“As an experienced Best Interests Assessor… I find that both reading the reflective blogs and participating as an observer in the Court of Protection, is highly beneficial in terms of my continued professional development. … Observing this hearing has been of significance for me, aiding a deeper reflection on some of the pitfalls within proceedings that can impact on the outcomes for P, most notably around professional miscommunication and when choosing the right professional to assess capacity.” (Eleanor Tallon, Independent Best Interests Assessor)
“This experience has been incredibly useful in giving me insight into the court – not only as to how barristers and judges interact and advocate in the Court of Protection, but also in displaying the practical implications associated with a lack of capacity under the Mental Capacity Act 2005. To see how deeply decisions about mental capacity can impact a patient’s life and the decisions that are made on their behalf was just eye-opening. … It is a great opportunity to see how the provisions and materials we learn about in our studies really affect people in a court of law.” (George Palmer, law student)
For these members of the public, the hearings provided a direct and unmediated opportunity to see how the statute (the Mental Capacity Act 2005) is applied to individual cases, and the processes by which best interests decision-making is achieved. It’s no overstatement to say that these observations have been in some cases transformative for health and social care professionals in developing legal literacy in ways that profoundly impact their daily practice.
(iv) Journalists are not the “eyes and ears of the public”
On the rare occasions journalists do cover Court of Protection hearings, there’s often a marked divergence between the way members of the public report what happened and the press report of the same hearing.
In part that’s because of the range of expertise that public observers bring to watching hearings. For example, one case that attracted a lot of media attention concerned whether it was in the best interests of William Verden, a teenager with a learning disability, autism and ADHD, to have a kidney transplant. Media reports (e.g. here) were short, pithy, factual, and aimed at a general readership. But members of the public who observed the hearing and blogged about it did so from specific professional and personal viewpoints and presented sustained and in-depth examination of the issues involved: from the perspective of a medical ethicist and mother of an autistic child (Imogen Gould); as an academic researcher on kidney donation (Bonnie Venter); and as a trainee barrister focusing on advocacy in the court (Jordan Briggs).
What journalists ‘see’ and report is organised with reference to whether it’s (in their terms) ‘a story’ or not. Members of the public observe court hearings through a multiplicity of very different lenses. Compare for example media reports of the case of the woman with agoraphobia ordered by the court to give birth in hospital with the blogs from our contributors, who include a woman with agoraphobia, a medical ethicist, and some midwives. Each of them brings her or his own unique personal and professional experience to bear, and each of them speaks authoritatively to a specialist constituency in relation to whom they are able to engage with acknowledged expertise.
A fundamental difference between press accounts and the blogs authored by members of the public is that while journalists, by and large, focus on communicating “the facts” and the story behind them, members of the public regularly provide commentary on the case they’ve observed, reflections on their experience of observing it, and make connections with their own personal and professional experience.
Journalist Polly Rippon and I both watched and then wrote about the same hearing and we reflected together on some of the differences. This was Polly Rippon’s story, as published in The Times.
At my invitation, Polly Rippon also blogged for us about her journalistic choices in constructing her story for The Times – and she and I discussed why it is so different from the approach I took as a retired academic psychologist. We compared her first sentence (“A judge will decide whether a woman with a learning disability and a £1 million fortune should be allowed to marry a convicted thief and fraudster who her daughter believes is after her money”) with the rather less gripping first sentence of my blog post: “This case before Mrs Justice Roberts (COP 13503831 heard on 6th – 8th July 2021) concerns coercive control and a planned predatory marriage (or civil partnership)”. This led me to reflect on my own approach to reporting hearings from my perspective as a member of the public:
“I actively try to avoid foregrounding what might be considered ‘shocking’ or ‘exciting’ material in favour of a more educational, measured approach. My key aim in this blog post was to communicate what I’d learnt from the hearing about the law on controlling or coercive behaviour. My own background is in academic Psychology, so it’s not surprising that after this first sentence, I moved quickly into giving a psychological account of controlling or coercive behaviour, including a link to an article in a counselling journal. Mindful of the blog’s audience of lawyers and those concerned with the law, I then described the behaviour as an offence under s. 76 of the Serious Crime Act 2015 and quoted an extract from the Statutory Guidance Framework. I provided all this background information up front, at the beginning of the blog, before addressing the specific issues in this particular case. Comparing my account with the Times piece, I can see how far removed it is from a ‘human interest’ story!”
As I also reflected in relation to the ‘predatory marriage’ case, another absolutely key difference between journalists and bloggers is that the former focus overwhelmingly (with recent significant exceptions, such as the excellent “The Trial of Lucy Letby” podcasts) on the outcome rather than the process of the hearing.
“In writing for the Project, I want to communicate the process by which justice is done – not just the outcome. So, the details of the questions asked and the answers given – and the way those answers are phrased – can really matter. This is what we get from observing a hearing, as opposed to simply reading the judgment afterwards. In the blog post about this case there were lots of places where I quoted as close to verbatim as I could (given that we’re not allowed to audio-record) because I felt the exchanges in court revealed aspects of the case, and the participants’ perspectives on what was going on, in particularly vivid ways.Compare, for example, the Times summary statement that the man “said that he was the victim of a conspiracy by his previous victims” (which is an accurate and succinct summary of the facts) with the more detailed account in the blog, which includes my own personal reflections on this.
“He denied allegations of wrong-doing in relation to other women – including those contacted by BU’s daughter, saying that this was “a collective accusation and a false accusation”.
Patel: Are you saying that all these complaints were coordinated and there was a sort of conspiracy to get you?
NC: Oh God, yes.
Patel: Oh, you are?
NC: Yes.
He projected (from my perspective) an impression of someone who felt aggrieved and misunderstood – a victim of conspiracy. It was hard to know whether or not he actually believes this.”
Because of the focus on the court process (as opposed to simply outcome), blog posts by members of the public also tend to be massively more detailed, describing the moment-by-moment unfolding of the hearing, and including (so far as possible given that we’re not allowed to audio-record hearings) verbatim dialogue. Compare, for example, this journalistic take on a hearing from March 2023 (“Judge overseeing treatment dispute raises concern about lack of legal aid”) with a PhD student’s detailed description of the same hearing (“Treatment escalation for a teenager in ICU”).
In sum, as members of the public, we have our own eyes and our own ears. Journalists and members of the public sometimes ‘see’ and ‘hear’ very different things when they attend the same hearing – and write very different kinds of reports of it.
1.2. Open justice means that we should be able to communicate about what we’ve seen and heard in court, our views about it, and our experience of the justice system.
Our blog posts attract a specialised readership – mostly health and social care professionals working within the remit of the Mental Capacity Act 2005, but also lawyers (including ‘aspiring’ lawyers, students, pupils, and paralegals) and a smaller but significant proportion of family members of ‘vulnerable’ people, many of whom have personal experience of the Court of Protection.
Many more people read our blog posts than will ever be able to make the time (or develop the courage) to observe a Court of Protection hearing. For many, we – rather than journalists – act as their “eyes and ears” because we observe and write, in detail, from identifiable perspectives, in ways that resonate with their own experience. For example:
“Excellent commentary on a nightmare of a case…. One of the most challenging things about my job (speech therapist) is when there is a chasm between families and clinicians and their interpretation of ambiguous/non-purposeful responses. It is often very difficult to know how much to walk families along the path of realisation and the clinical context matters enormously…. With the impossible time pressure on clinicians, this is sometimes just impossible. I’ll be the first to admit I don’t always get it right. …. Thank you so much for these reports from the Court of Protection. They are of enormous benefit to a wide range of readers. They certainly make me reflect on the privilege and pain of accompanying those who experience these heart-breaking traumas.” (Tom Richards, Speech and Language Therapist)
“Would you please pass on my grateful thanks to “Anna” for taking the time to tell her story of her journey through the awful DOLS procedure. My friend discovered your website and passed on the link to me as I am going through the very same situation at the moment with my mother. I could not believe the similarities – it was almost the mirror of my situation! All of the professionals I had meetings with just dropped in random sentences such as ” it may go to the high court”, ” it will take months to resolve” . No one sat down with me and explained the whole thing …. I learned more from ten minutes reading Anna’s story than I did from any meeting with any of the professionals … I hope other people will find your website and read this story in future. It should be part of the Adult social care training programme , and I will be suggesting this when I contact my mother’s social work team.” (e-mail from Family member of P, quoted with permission)
This kind of engagement embodies the principle of open justice that underpins our Project.
There are restrictions on what we are allowed to write – most relevantly, for our purposes, the reporting restrictions imposed by the court in the (somewhat Orwellian-named) “Transparency Order”.
1.3 Open justice is a collaborative enterprise.
Having started out with the assumption that we would be doing “fly on the wall” observation, and with some concern about how the judiciary (in particular) would view our presence in court, I have learnt that open justice works best as a collaborative process. It changes the way that justice is done: first just through our presence, as lawyers and judges accommodate to having observers in court; second through our active engagement with the processes whereby justice is done.
(i) Simply observing changes how justice is done
Public observers in the Court of Protection have become much more common in the three years since our Project began. “Before Covid, I’d never had a public observer in court,” one barrister told me, “but now I’ve learnt to expect it. There were 12 observers in one of my hearings in December”.
First, counsel now regularly opening cases with introductory summaries for observers – often at the prompting of the judge who asks them to do so “for the observers”. This is generally seen as a positive: “It’s good practice to have to think ‘how can I summarise this case in 2 minutes’ at the outset. I think it helps to do that in most cases anyway, but a public observer’s presence means we are more likely to have thought about it first. It aids the judge’s understanding and just as importantly the understanding of non-lawyer participants/litigants.” (Barrister)
Second, when observers are present lawyers are more likely to clarify and highlight key legal concepts and to avoid acronyms, jargon and initialisation. “There’s a few bad habits that have been corrected: […] we’re thinking about how we communicate and tend to explain the ratio of authorities, or what obscure pieces of legislation mean….” (Ian Brownhill, barrister); “That drive to ‘clarity’ goes for lawyers and (as I perceive it) judges too, who are more likely to explain what they are doing in straightforward terms” (Barrister). One barrister is especially positive about the effect of observers in ensuring that fundamental legal principles come to the fore and as a result are “more rigorously and consistently applied”: “There has been real enthusiasm for public observers in the Court of Protection. It has been seen as a real opportunity to counter the perception of it as a secret court. As a result, we have been taking the time to expressly set out the first principles and legal principles which should govern everything the Court does. This exercise, which was prompted by a desire to make the proceedings accessible and easier to follow has actually meant that as the principles are pushed to the forefront of everybody’s mind, they are more rigorously and consistently applied.” (Josh Hitchens, barrister)
Third, we’re told that blogs by observers create an opportunity for self-reflective learning “We reflect on our advocacy by reading the blogs!” (Ian Brownhill, barrister). “I have actually found the blogs produced by observers to be really interesting and useful.” (Barrister). “Reading the blogs is entertaining – a little bit like the review following opening night. It keeps everybody on their toes” (John McKendrick KC).
Fourth, there seems to be some agreement that having observers in court means that lawyers, and the judge, are “on best behaviour”: “It absolutely changes things – practitioners and judges are less sloppy I think, and take the time to properly set out the facts, the law and judgments when they might otherwise refer to things in a more shorthand way. This, I think, is a good thing since it means that anyone participating or watching (often family or even P themselves) can actually follow what is going on far better. It means we are all on ‘best behaviour’ essentially!” (Barrister); “I think observers make the barristers try harder in a hearing – like in a driving test. You never drive like that normally. They are more aware of what they are supposed to do in court” (Solicitor). Eight barristers (independently of one another) told me that having observers present improves judicial behaviour – in particular via what was characterised by one of them as “improved civility in court”. They referred to “rudeness” from judges who were “hostile” to or “impatient” with their oral submissions in court, or “dismissive” of P and P’s family members. One barrister emphasised that that Court of Protection judges are “very good – from DJs up to HCJs. They are serious about the role they are performing and appear to enjoy the work” but added that being observed “acts as a brake on some of their more obstreperous characteristics”. One commented that judges behave better in front of observers, knowing that the public would be “horrified” at their customary level of disrespect (e.g. expressing the view that some hearings are “a waste of time”). Some family members also believe that having observers in court leads to better behaviour by the judge, and that the judge was “fairer” to them because observers were there: “ [Observer’s] presence was valuable – the judge was quite snappy and aggressive with me before he arrived; and was clearly in fast-forward mode. That changed.” (Litigant in Person)
(ii) We actively engage with the justice system
The role of our Project is to support the oft-stated judicial aspiration for greater transparency in the Court of Protection, and to the extent that we may be seen as challenging the court, we try to frame our engagement as that of ‘critical friends’.
Our engagement activities include:
attending Court of Protection User Group meetings (there are around three each year for each of the eight regional groups), so that we can raise issues of transparency directly with judges and lawyers
liaising with a nominated Deputy Service Manager in HMCTS, who has taken on responsibility for trying to improve listings – we alert her to errors and she contacts the teams that are getting it incorrect to target and support them
giving invited talks about transparency matters to lawyers and judges (e.g. Park Square Barristers in Leeds, 19 January 2023; CPBA Annual Conference, 39 Essex Chambers, 13 July 2022; Court of Protection Practitioners’ Association Annual National Conference, Principality Stadium, Cardiff, 24November 2022; Inner Temple Advocacy Weekend, 29-30 January 2022).
mentoring law students and aspiring barristers by supporting them to observe and blog about hearings and thereby (hopefully) creating a new generation of legal professionals for whom transparency is an established norm.
We’ve twice made lengthy and detailed submissions to the Court of Protection Rules Committee – on Transparency Orders (outcome pending) and on closed hearings.
None of this was what we’d envisaged in setting up the Project just over three years ago. It has emerged organically, and in partnership with the court as part of its commitment to transparency.
3/. What is your view on how open and transparent the justice system currently is?
Our Project sounds like a success story for open justice – and in many ways it is. But I want to make visible the hard work it takes to make this happen, the multiple barriers to transparency we have to overcome day after day, and the slow pace of change. It shouldn’t be this difficult.
Transparency in the Court of Protection works (when it works – and it often doesn’t) because of the hard work and dedication of individual judges, lawyers, court staff and members of the public – all of us battling against a system which seems set up to obstruct us.
Here’s how it’s supposed to work.
The fantasy version of access to remote hearings in the Court of Protection
A member of the public looks in the “Court of Protection” section on Courtel/CourtServe for a hearing to observe.
The listing provides essential basic information including:
whether hearings are public or private
what hearings are about
what the attendance options are (in person/remote)
the type of hearing (e.g. directions, case management, final)
contact information (to confirm the hearing is going ahead and/or request remote access)
She picks a hearing to observe – say, a challenge to a deprivation of liberty (because that’s what her mum’s case is about), in the Midlands (because that’s her Mum’s area), at 11am the next day (when she’s free), and she chooses one that says it’s being held via cloud video platform (as she lives a long way away). She sends off an email to the contact address given and receives a reply with the link and a Transparency Order attached well in advance of the start of the hearing, and logs into the hearing without problems.
But that’s not how it actually works in practice.
The reality
Very few members of the public find Courtel/Courtserve an accessible or user-friendly resource. Almost all observers rely on our Project’s version of the listings: without our version, their observation simply wouldn’t get off the ground.
But our version of the listing depends on us being able to decode – or make informed guesses – about the hearings. Quite a lot of hearings are listed as “private” when we don’t think they are. Many don’t say what the hearings are about, and unless we’ve observed earlier hearings in the same case, we have no way of knowing. Some don’t say whether the hearings are in person, remote or hybrid (and the initialisation “CVP” doesn’t mean anything to most members of the public, so we have to spell that out).
We provide a “template email” on our home page for people to use when requesting access to remote hearings because we discovered that without it, members of the public were not providing sufficient information (e.g. the case number and the name of the judge) for court staff to respond to their requests. Emails saying “can I observe the hearing at 11am tomorrow please” do not meet with success and are frustrating for everyone.
Nonetheless, a large number of people who’ve made well-formed requests to observe hearings get no reply. I know this because we suggest that emails are copied to us so that we can provide support with access, if necessary. And it often is necessary – and still sometimes there is no response (or the response comes too late to observe the hearing). My own experience is that I get no reply – no reply at all!– to about one in every six requests to observe hearings, even after sending repeated emails, and phoning the court. (Usually nobody answers the phone.) I’m knowledgeable and persistent: for most would-be observers the failure-to-respond rate is much higher.
The problem seems to be that the listings instruct the would-be observer to email the regional hub – so Birmingham for a hearing in Worcester, or Bristol for a hearing in Truro, or Cardiff for a hearing in Caernarfon. Court staff at the hub then have to forward the email to the regional court. Court staff at the regional court then pass it on to the judge in the regional court whose hearing it is (often, they say, for “permission” for the observer to attend – although in fact no “permission” is required for public hearings). They then wait for the judge to get back to them, and the whole process happens again in reverse: regional court staff send email to hub and hub replies to would-be observer. This is a cumbersome and time-consuming process. It places burdensome and unnecessary pressure on court staff – and I am told that they are already overworked and under-resourced (and also that there is rapid staff turnover, resulting in frequent unmet training needs). It is setting everyone up to fail. Surely HMCTS can devise a better system?
If an observer is lucky enough to receive the link in time for the hearing, there’s still a good chance that the hearing will be vacated – about 1 in 3 of all COP hearings are (and most observers don’t know what “vacated” means so we’ve had to explain that too). It’s more likely than not that she won’t have received a Transparency Order (in fact, it’s more likely than not that she will never receive a Transparency Order) – and there’s also a real risk that the cloud video system won’t work well enough for her to either see or hear what’s going on. We do provide would-be observers with a link to the gov.uk information about how to use CVP but sometimes that’s not enough. I once watched – and then blogged about – a two-and-a-half hour hearing with no sound (“The silent courtroom: A remote hearing without sound – and why transparency matters”).
Workarounds
To the extent that transparency “works” in the Court of Protection, it relies on a range of pragmatic “workarounds” that enable us to bypass systemic pressure points, limitations and fractures in the system. Although we continue to lobby HMCTS to get the system working better, we’re increasingly figuring out ways around the system. And by “we”, I mean all of us – observers, court staff, lawyers and judges. Here are some of our workarounds.
Since lists are obscure and incomprehensible to most members of the public, the Open Justice Court of Protection Project runs our own listing service on social media, where we translate “s.21A”, “CVP”, etc into intelligible prose and also select out some “Featured Hearings” which we think are likely to be accessible/of interest to observers.
Knowing that hearings are often not in the COP list on Courtel/CourtServe (the only public listing service for county courts), we also spot-check the Daily Cause Lists across England and Wales for ‘missing’ hearings. A systematic check of Daily Cause Lists for incorrectly listed COP hearings takes about 2 hours and often adds a third as many hearings again – but we only do this occasionally due to time constraints. (Things have improved – a systematic check in 2020 doubled the number of CoP hearings!)
Some Tier 3 judges know (because we’ve complained in the past) that if they leave the RCJ and hear cases in regional courts, there’s very likely to be a listing problem (often their hearings don’t appear at all, anywhere) – so when they have hearings in the regional courts, they ask their clerks to alert me.
When hearings are listed as “private”, we know that this is most likely to be because someone filled in List Assist instead of the COP template, and that the hearing is actually public, not private. I sometimes make a special effort to attend “private” hearings to check this out – and I’m almost always correct. On the Open Justice Court of Protection Project listings we either omit the word “private” or say that although it’s listed as private, we doubt that it is.
Because so many emails to the regional hub contact address provided in the lists get no reply, I often contact the judge’s clerk for the link, or one of the barristers if I know who’s involved in the hearing.
Knowing how frequently there’s no reply to my requests for links for remote hearings, some court staff and a couple of lawyers simply send me the links to hearings without waiting for me to ask for them. This reduces stress on everyone!
Because there’s no information at all on the RCJ website as to what hearings are about, lawyers involved in cases they think the public will be interested in regularly alert me themselves. (That’s true of some cases in the regional courts as well, although at least there is some, minimalist, information available there.)
There’s no way of knowing when cases I have been following are back in court – no search facility that enables me to search on the case number, and no way of setting an automated ‘alert’ using the case number to inform me that a case is being heard again (including the possibility that it’s being heard in the Court of Appeal, or before a different judge, or has been removed from the Tier 3 list and returned to a regional court). So, when I’m following cases with multiple hearings over time (several of the cases I’ve observed have continued for years with 5-10 hearings), I often have to rely on lawyers to let me know, via a personal email, that the case is back in court.
A judge regularly gives me permission to circulate the link to his hearings directly to other observers – because otherwise I have to negotiate emails from members of the public complaining of lack of access, which I have been in the habit of forwarding to his clerk so she can send the link to them.
Several judges send me links (unrequested) to out-of-hours or urgent hearings that have not made it onto the published lists.
Several judges have, on more than one occasion, delayed the start of a hearing so that observers can be there from the beginning– knowing full well that it’s likely to be a tardiness not of our own making.
We know some judges who have set up personal MS Teams systems in their own courtrooms so as to avoid having to use cloud video platform, and to provide the best experience for remote access (which is often how P and their family access the court as well as observers). At least one RCJ judge has delayed the start of a hearing and moved courtrooms to enable an observer (and only an observer) to attend a hearing remotely.
Journalists who have access to information not made available to the public (e.g. via the alerts service) sometimes let me know via a personal email.
My conclusion is that “the justice system” is not at all open and transparent: it’s a system that seems designed to frustrate the judicial aspiration for transparency. It’s not fit for purpose.
The transparency we have achieved via the Open Justice Court of Protection Project is the outcome of the collective commitment of judges, lawyers, court staff and members of the public (plus journalist Brian Farmer) who’ve dedicated their time, knowledge and skill to making it happen – because some of us really believe that transparency is fundamental to justice in a democratic society. It would be good if “the justice system” could support that.
4/. How can we best continue to engage with the public and experts on the development and operation of open justice policy following the conclusion of this call for evidence?
Please engage with the Courts and Tribunals Observers’ Network (of which I am a part). It brings together a range of stakeholders with expertise across different courts and tribunals and we are actively seeking to inform the Government and Judiciary and other relevant bodies about access problems in the justice system and to help develop better policies and law.
C. Listings
Listings are currently desperately inadequate – although I have been forced to recognise (in conversation with observers in other courts) that the Court of Protection may be better than most. It’s extraordinary to me that the Court of Protection – a court with “transparency” as a central philosophical principle – produces court listings entirely unsuited to delivering on its stated objectives.
I’ve been writing publicly about problems with the court listings since August 2020 – and tweeting about particular instances, expressing my concern in talks before lawyers and judges, and sending written complaints to relevant persons and organisations. There have been some improvements, but the pace of change is glacial.
Here’s one from the Courtel/CourtServe list today that gets it right and I’m displaying it first of all because it shows that it’s possible to list hearings in a way that the public find accessible and covers all the relevant information. This hearing is about “Appointment of an Interim Deputy” – something members of the public who are family members of vulnerable people are often concerned about, especially if they want to be Deputy themselves or have been removed from acting as a Deputy. It’s important for people to see that they can watch a hearing about this issue. It’s clear that the hearing can be watched remotely, that it lasts an hour, and the contact information is correct. It doesn’t look that complicated to me – so I don’t really understand why so many listings get it wrong.
Here are some of the most egregious problems.
1. Failure to list hearings in Courtel/CourtServe (or any other public online list)
If we don’t know that a hearing is happening then it is effectively taking place in secret. Obviously, I can’t know how many hearings are happening in secret without ever being publicly listed – but I do know of some. I’m not referring here to urgent or emergency out-of-hours hearings – I know it’s inevitable that those can’t make the listings – but to hearings that everyone involved in them knows are happening weeks or months in advance. Here’s one recent example.
It was a hearing I particularly wanted to observe concerning a young woman with autism, mental health issues and some physical health problems who was ready for discharge from hospital but was refusing to return to the bungalow where she’d been placed previously and been desperately unhappy, leading to several episodes of self-harm. There were questions about her capacity to make her own decision about where to live and about her best interests. The case was heard on appeal by Mr Justice Peel (Wilshire County Council v RB & Ors [2023] EWCOP 26) who says in that judgment that the case would be re-heard, the appeal having been allowed, by HHJ Robertshaw on 27 June 2023 for three days.
My subsequent letter to Mr Justice Peel (see below) describes what happened next.
The depressing reality is that I wasn’t even particularly surprised. There’s a recurrent problem with hearings simply not appearing on any listing accessible to the public – not on Courtel/CourtServe’s COP list, not on the Daily Cause list for the relevant court, and not on the RCJ or First Avenue House lists.
The correspondence below provides another example: a hearing in Northampton before a Tier 3 judge (Lieven J) never appeared on a public list – as I explained to my HMCTS contact. (My suggested solution has not been implemented). Hearings before Tier 3 judges on circuit are regularly omitted from the listings: I’ve described other cases in my blog posts including “A ‘secret’ hearing on life-sustaining treatment” before Hayden J in Newcastle.
Dear Jess
I was told by someone involved in the case that there was a hearing before Lieven J today at 10.30am, and I wanted to observe it.
The hearing was not listed on the Royal Courts of Justice Daily Cause list.
I checked with the person where the hearing was happening and was told Northampton.
I looked in Courtel/CourtServe. There was nothing in the COP list for Northampton.
I went to the Northampton Daily Cause list in Courtel/CourtServe and found two hearings before Lieven J but they were listed for 12noon and 2pm and the case numbers lead me to believe that they were not COP hearings.
Finally, I wrote to Northampton County Court asking whether they were able to help me, and I copied in Lieven J’s clerk, Sarah McMohan. Most members of the public would not, of course, know who Lieven J’s clerk is, or have the chutzpah to bother her.
I have not received a response from Northampton County Court, but Sarah McMohan replied promptly with a link to the hearing, and I was able to watch it. So this had a happy ending.
But yet again a hearing before a Tier 3 judge has taken place without ever appearing on a public court list. This is a recurrent and apparently intractable problem which I have documented many times before. Is there anything that HMCTS can do about it?
In my view ,the best solution would be to continue the doomed attempt to get these hearings listed in the regional courts but, recognising that this often doesn’t happen, to also list them on the RCJ Family list where these judges’ hearings normally appear, and where those of us who regularly observe hearings know to look for them. A note could be added to say that they are not actually happening in (or from) the RCJ or the actual location could be given in place of the RCJ Court number.
In this case, since it was an MS-Teams hearing anyway, the fact that the judge was conducting it from Northampton rather than London was irrelevant except for the fact that it led to a listing failure.
When I report these listing failures, I am usually told that there is a “training need” and that someone will send a memo round. Then it happens again. If you have ideas about how to fix this, that would be wonderful.
Best wishes
Celia
When I learn about a hearing from a source other than the listings (from a published judgment as with the hearing before HHJ Robertshaw, from a barrister as in the hearings before Lieven J and Hayden J; or from family members), I always look for it in Courtel/CourtServe. About 50% of the time, I can’t find it – not in the COP list, and not in the Daily Cause list. It’s a “secret” hearing, and I’m only able to watch it because I have “inside” information. This does not support the judicial commitment for transparency.
Hearings are also frequently listed in CourtServe in the wrong place – not in the COP list which is where they’re supposed to be, but in the Daily Cause list for the individual court (and often under a sub-list for a particular judge) – making them challenging to locate. Every so often I go systematically through all the Daily Cause hearings listed for a particular date looking for COP hearings that should be in the COP list instead or as well as the Daily Cause List: the percentage of COP hearings that don’t appear in the COP list has fluctuated between about a quarter and about a half ever since I’ve been doing this.
Here’s an example from last year that I incorporated into a talk for lawyers and subsequently tweeted. A hearing (which actually I did manage to observe and blog about) before DJ Birk in Leicester did not appear in the COP list. I found it (as the slide says) in the Leicester Daily Cause list, under a sub-list labelled “Daily DJs”. Additionally: it says it’s PRIVATE – which turned out to be wrong – and it doesn’t say what it’s about : “MATTERS IN PRIVATE” is about as opaque as it’s possible to be. In fact, it turned out to be really interesting for me to observe: see “When family members apply to become parties: A hidden and “private” (but not sinister and secret) hearing”).
2. Hearings are regularly and erroneously labelled “PRIVATE” or ‘NOT OPEN TO THE PUBLIC”
Almost all COP hearings are supposed to be listed as “Public”. That’s the default, except for two categories of hearings: “Dispute Resolution Hearings” (DRH) and “closed” hearings, both of which are always held in private. It’s open to judges to hold other COP hearings in private – or to exclude the public from part of a hearing that is otherwise in public – and this happens occasionally, but rarely.
On that basis, it should – surely! – be straightforward for HMCTS court staff to list COP hearings as “Public” because 95% or more of them actually are “Public”. But (as already illustrated in the slide above) they don’t. I struggle to understand why there is a repeated and seemingly intractable problem with this.
Here’s a recent example.
4 September 2023
to COP.Manchester
Dear DJ Gray
I’m writing in my capacity as co-director of the Open Justice Court of Protection Project. We support the judicial aspiration for transparency in the COP by encouraging members of the public to observe hearings.
Looking at the hearings listed in Courtel/CourtServe for tomorrow (see photograph below), I notice that all three of the hearings before you are marked as “NOT OPEN TO THE PUBLIC”. It’s very unusual for COP hearings not to be held in public. Is this actually correct? We have not alerted the public to your hearings in case you are planning to hold them in private, but we are surprised to see this, as there is no indication that they are Dispute Resolution Hearings.
I notice also that none of them includes case descriptors (i.e. indication of the issues before the court). This is also unhelpful for transparency purposes.
I wonder if you can offer me any help in understanding how your hearings have come to be listed like this.
Thank you for your support of open justice.
Celia
CourtServe listing
In response, the Team Leader from the Court of Protection in Manchester thanked me for bringing the matter to his attention and said: “The points you raise have identified a training need for one of my colleagues … who is new to the role of usher and has recently taken on the responsibility for producing the daily lists…” (email 5th September 2023)
As I said earlier, most of my observations about listing problems are responded to with reference to a “training need” – but the same problems recur over and over again.
3. There’s no information as to what hearings are about
There was a clear official statement, when the Court of Protection Transparency Pilot was launched more than seven years ago now (on 29th January 2016) that descriptors of the issues before the court would be made publicly available in listings. According to the “Pilot Background Note”: “Policy officials will also work with Her Majesty’s Courts and Tribunals Service to amend the way in which court lists are displayed, so that they provide a short descriptor of what the case is about, allowing the media to make an informed decision on whether to attend the hearing” (Available at https://www.judiciary.uk/wp-content/uploads/2015/11/cop_transparency_pilot_background_note_19.11.15.pdf, downloaded 6 September 2023).
Nearly eighteen months later, this still hadn’t been achieved, and the judiciary seemed unsure about how to go about implementing it. The (then) Vice President of the Court of Protection, Mr Justice Charles, said: “It is recognised that it is important that cases are appropriately described when they are listed to provide information to the public at large of what they are about and when and where they will be heard. Comment on how this should be and is being done is welcomed. As is more general comment on how the public and the media can make themselves aware, or should be made aware, that certain types of case are due to be heard…” (Charles J, The Transparency Pilot, 20th June 2017)
It’s still the case that many (sometimes most) listed hearings don’t have any indication of what the hearing is about. None of those posted on the Royal Courts of Justice website ever does – and it’s enormously frustrating for members of the public who have special interests in observing hearings on particular issues. Some indication of their content (‘treatment withdrawal”, “caesarean”, “coercive and controlling behaviour”) would be much more likely to induce observers to attend. (So, too, would be some indication of their likely duration.)
There is a set of “descriptors” provided for use in listing cases in the regional courts and in First Avenue House. First Avenue House routinely provides this information (e.g. in FAH list of 6 September 2023, “Whether the applicants should be appointed as deputies for property and affairs’; “(a) Where ESZ should live (b) Authorising a DoL in connection with care and residence (c) Contact with specified persons”; “(a) Assessments of capacity and need for care and support (b) Access to KB in order to carry out such assessments”). This information is should be, but is not, systematically supplied in the regional courts listings – albeit that this is something that’s been improving (slowly) over the last three years. Information remains minimal – and is often likely to be inaccessible to ordinary members of the public (e.g. s.21A, s.16, DOL, LPA). A few summarising sentences would, of course, be excellent but is almost certainly beyond the resources of the court.
The Project has created some (very modest) “Key Performance Indicators” against which to assess the performance of the Court of Protection in relation to transparency in listing. The most recent assessment is as follows:
KPI 1. List the hearing in the COP list on Courtel/CourtServe POOR (more than a third of COP hearings did not appear in the COP list on CourtServe on the date of assessment)
KPI 2. Make it clear the public can attend – POOR (fewer than a half of hearings said they were PUBLIC)
KPI 3. Tell us how we can observe (i.e. remotely/in person) – VERY GOOD (a pleasing improvement on this KPI – almost all of listings provide this information)
KPI 4. Supply correct contact information – FAIR (nearly 1/5 hearings provided contact details for the court where the hearing was taking place, rather than the regional hub)
KPI 5. Tell us what the hearing is about– FAIR (around half of the listed hearings provide some indication of the issues before the court – another pleasing improvement)
Many people who contact the Open Justice Court of Protection Project believe that the court is deliberately obstructive of open justice. I understand why it can feel like that. It takes an effort of imagination to realise that problems of transparency are caused not by deliberate intent, but because of systemic failings in the necessary infrastructure needed to support open justice. Open justice fails despite the judicial commitment to it. I don’t really believe that the lists are deliberately designed to discourage us from observing hearings. It’s just that – very often – they have that effect. It’s glaringly apparent that the listing system wasn’t set up in an outward-facing user-friendly way for members of the public. It needs a thorough overhaul.
Finally, two listing issues, in particular, that have arisen this year in connection with our work relate to (1) ‘closed hearings’ and (2) committal hearings.
In relation to ‘closed hearings’, we were dismayed to discover that we’d misreported the facts of a case due to the judge having decided to run secret ‘closed’ hearings (without P’s mother and without us) in parallel with the hearings in open court which we’d attended and reported on. We didn’t know about the decisions made in the secret hearings (the intention was to conceal this information from P’s mother) and the observers felt we had been misled by the court, making (as we said) a mockery of open justice. We wrote a blog about this here: Statement from the Open Justice Court of Protection Project concerning an inaccurate and misleading blog post and publicised the threat this poses to transparency on the Radio 4 programme Law in Action (“Secrecy in the Court of Protection”). We subsequently made a submission to the subgroup of the Rules Committee set up to advise the (then) Vice President about how closed hearings should be dealt with in future. This led to New Guidance on Closed Hearings from the Vice President of the Court of Protection. Since then, we have seen “closed” hearings listed on the RCJ site – so although we still don’t know which case they concern, or what they’re about, and although we still can’t observe them, at least the court is providing public notification of the fact that closed hearings are happening. We don’t think any of this would have come to light without our Project, and we’re proud to be able to highlight a concrete achievement in ensuring better transparency in the future.
In relation to committal hearings, it’s only this year that we’ve had the opportunity for the first time to observe and report on hearings at which judges consider whether someone (usually a family member) should be sent to prison for breaching court orders – for example, for publishing material on social media identifying P when there’s an order that they must not do so, with a penal notice attached. This year we reported on one such hearing in A committal hearing to send P’s mother to prison – and the challenges of an in-person hearing. This is an ongoing case: P’s mother recently lost an appeal against her suspended custodial sentence. One reason why we’ve not observed these committal hearings previously is because they have not been correctly listed. There is a Practice Direction (Committal for Contempt of Court – Open Court) which says that says that open justice is “a fundamental principle” and that “the general rule is that hearings are carried out in, and judgments and orders are made in, public” (§3), and that these hearings should normally be publicly listed with the information that an application is being made to commit someone to prison, and the full names of that person and the person/organisation seeking committal (§5.2). In fact, it seems that some committal hearings – in both the Court of Protection and in the Family Court – have been listed as private, and/or the fact that they’re committal hearing is not included in the list, and/or the names of the applicant and alleged contemnor are not published (see Committal hearings and open justice in the Court of Protection)). Here’s one recent example which is in breach of the Practice Direction because it doesn’t name the applicant or the person alleged to be in contempt.
On request, I was subsequently provided with a name, but no information about the alleged offence or the outcome of the hearing. I was told that the judgment would be published on the judiciary.uk website. I have not been able to find it there, despite checking regularly having since the end of June 2023). Some weeks ago, I asked the court to help me locate it, and was told “we are awaiting the directions”. I don’t know what that means. I suspect that someone whose name has not been made public has been given a prison sentence in secret and that there is no public record of this. This is not open justice. I find this very troubling. It reinforces, and provides concrete evidence of, exactly the notion that Mostyn has said he hopes to dispel – “the idea, which continues to be peddled by certain sections of the press, that the Court of Protection is a secret, sinister court which dispenses justice behind closed doors.” (Mr Justice Mostyn “Judge defends Court of Protection as not a “sinister secret court“, Today’s Wills and probate)
KPI 6. If the court is going to hold hearings with the deliberate intention of excluding one party (usually a family member), there needs to be some public accountability for this so that we at least know that it is happening, how often, and why. Listing the hearings as ‘closed hearings’ is a good start. I don’t think the court is planning to produce an annual report covering the number and nature of ‘closed’ hearings, but I think it should.
KPI 7. Hearings at which the court is deciding whether or not an alleged contemnor should be sent to prison should normally be listed in accordance with the Practice Direction, held in public and a judgment published. This is not always happening and it’s corrosive of open justice.
6/. Do you find it helpful for court and tribunal lists to be published online and what do you use this information for?
It’s essential to have these lists published online. It would also make a huge difference if they could be searched (e.g. via case number) and if it were possible to set up an ‘alert’ so that we could know (without bothering barristers) when a case is coming back to court.
We use the information to inform members of the public about hearings they can observe. We check the online lists every day and reproduce them in a more accessible form on social media (fixing problems with initializations, explaining obscure terminology, removing the word “private”, and correcting or adding contact information (RCJ managers have supplied us with an additional email address and a phone number – neither available from their website – to support us in seeking to gain access). See above for the problems and difficulties we face.
I’m concerned about the proposal to allow professional users to access lists “not available to the public”. As a member of the public, I’m already excluded from information available to journalists, including the “alerts service” whereby the COP brings to the attention of journalists those cases in which it proposes to impose particularly draconian reporting restrictions – thereby giving journalists the opportunity to contest or query those reporting restrictions. As a member of the public, I also have an investment in knowing about these hearings in advance and having the opportunity to consider the appropriateness of unusually stringent reporting restrictions and making the case for greater transparency.
If the core members of our Project were to be excluded from some more comprehensive lists available to journalists, this would negatively impact on our ability to contribute to open justice. We recommend some mechanism for members of the public (neither accredited journalists nor duly authorised lawyers) to apply for access as well – in a swift, efficient manner. I appreciate that lists with additional sensitive information might not be suitable for general public access, but would want to be sure that the core group members of organisations such as ours with a legitimate interest in accessing these lists, and a track record in open justice, would be able to access them too. I have laboured the point (earlier in this submission, see my answer to Q1) that open justice cannot and should not be delegated to journalists alone – because there are not enough journalists covering the courts and journalists do not always function as the ‘eyes and ears of the public’ given the multiplicity of legitimate personal and professional interests members of the public bring to hearings, and the in-depth and detailed analyses they often write about them. So, if there are to be lists with restricted access, projects like ours should be able to gain access too.
7/. Do you think that there should be any restrictions on what information should be included in these published lists (for example, identifying all parties)?
Court of Protection lists do not identify all parties – they routinely suppress the name of “P” (the vulnerable person at the centre of the case) and their family. More problematically, they often do not include the names of public bodies as parties.
8/. Please explain whether you feel the way reporting restrictions are currently listed could be improved.
Court of Protection hearings are generally open to the public and should be listed as “Public with reporting restrictions”. They often say “PRIVATE” instead. I’ve detailed this problem above. We don’t know what exactly the reporting restrictions are until we receive the Transparency Order – but there is a ‘standard’ template which restricts publication of any information likely to identify P and their family, and where they live. There is currently a sub-committee of the Court of Protection Rules Committee investigating how Transparency Orders can be improved.
D. Accessing courts and tribunals
You say: “We are seeking your views on whether there is more the government could offer to support public access to court and tribunal hearings”.
Supporting the public with accessing courts and tribunals needs to start by improving the listings (see section C above) – since we’re unlikely to go along to a courtroom if we don’t even know that a hearing is happening.
In-person hearings pose a range of access challenges beyond simply locating the court. For example:
We need to be able to check, in advance of travelling to the court, that an in-person hearing is actually happening. Since about 1 in every 3 hearings (in my experience) is vacated, we risk a wasted journey. I have repeatedly tried phoning courts in advance of leaving home to check whether hearings are going ahead, and never had a satisfactory response. (I now ask barristers or judge’s clerks instead, when I know who they are.) Again, this is about having more – appropriately trained – outward-facing court staff that members of the public can access with questions like this. This means more funding!
A member of the public turned up at the RCJ for a hearing, listed as public, before Arbuthnot J on 7thDecember 2022. There was a sign on the court door saying “IN PRIVATE – NO ADMITTANCE”. He left the building. I learnt from Brian Farmer – who was similarly deterred from entering – that the sign had been left up in error. I have previously experienced “PRIVATE” signs on courtroom doors myself and wrote to HIVE and to Arbuthnot J about this on 11 December 2022.
While waiting to enter a courtroom in the RCJ for a hearing before Hayden J, I saw a sign on the door saying IN PRIVATE – NO ADMITTANCE”. As I knew the hearing was supposed to be PUBLIC (I double-checked this with the lawyers also waiting outside the courtroom), I alerted the usher and asked that it be removed. Unusually (ushers are generally helpful!), she was dismissive of my request and said she’d remove it “later”. As we entered the court the sign was still up, and I repeated my request. She seemed irritated by this and said she’d do it “when the hearing starts” – which rather defeats the purpose of open justice, since seeing the sign on the door would likely mean that potential observers would have left by then.
At Newcastle County Court, there was no listing up on the notice board for the hearing we wanted to observe before Poole J, and nobody readily available to ask. I’ve experienced this several times before – but this was a new experience for one member of the OJCOP core group, Claire Martin. She describes what happened: “Once through security, we spotted several rows of A4 notices on a board on the wall. They had the different courtroom numbers and cases being heard, with judges’ names and hearing numbers. Mr Justice Poole was not listed. What to do? A security guard suggested going to the first floor where courts and a reception desk were located. ‘Ask there’ he said. The reception desk on the first floor was empty. The listing boards on the first floor also didn’t include the hearing we were looking for. … There was a conspicuous absence of people whose job it was to ensure everyone knew where they were going. Perhaps these jobs don’t exist – or perhaps it was lunchbreak? We managed to intercept one person, a lawyer I think, who said she was really not sure but pointed us to a waiting area. The waiting area also had boards with listings, but ours wasn’t on these either. Celia attempted to identify whether the lawyers from the hearing we hoped to observe were in any of the six small consulting rooms (with small windows in them) leading off the waiting area, but was unsuccessful. … At that point, we saw Joseph O’Brien, counsel for FP, arrive. Then we knew we were definitely in the right place.” (A committal hearing to send P’s relative to prison – and the challenges of an in-person hearing)
Some observers have disabilities that affect their ability to access the court – remotely and/or in person. In our experience, it can be difficult for observers to feel confident that their need for reasonable adjustments will be understood and supported – even, ironically, in the Court of Protection which works intensively with disabled people. An observer with hearing loss struggled to hear the proceedings when seated, as directed, in the back row of the court. The co-founder of OJCOP, Gill Loomes-Quinn describes how “I found standing when the judge entered the room problematic (I have compromised mobility and use walking sticks) but the formality of the proceedings meant that I felt unable to draw attention to myself in order to request an adjustment to the expectation that I would stand” (“Under the radar”) Since then we’ve heard reports of an usher calling out “Stand if you are able”, which sounds much more progressive.
I bring my laptop to Court of Protection hearings and use it to make detailed notes and to access statute and case law during the course of the hearing to help me to understand, as best I can, the legal arguments. I am sometimes directed towards seating without any desk surface on which to rest a laptop – even when there is vacant seating with desk space on the press benches or further forward in the court. I once moved to a vacant seat and was ordered to return to the back of the court. As far as I can see this simply works to prioritise an outdated protocol (probably invented before laptops even existed) over the practical exigencies of open justice. I do realise that when I’ve complained about this to other court observers, they’ve simply expressed amazement that I’m allowed to take a laptop into court at all. Electrical sockets for recharging laptops are also few and far between in some courts – I realise this can be a problem for lawyers too, and have several times lent them my extension lead.
So, there are some quite modest Key Performance Indicators for transparency here:
KPI 8 The courts should be properly resourced so that there are trained staff available first thing on the morning of a listed hearing to answer questions about whether it is actually going ahead or whether it has been vacated.
KPI 9 Remove any signs on courtroom doors stating that hearings are PRIVATE when they’re not. (We recommend having a sign that says “THIS HEARING IS IN PUBLIC. EVERYONE IS WELCOME TO COME IN”. I’ve never seen a sign like that on a courtroom door – but what a difference it would make!)
KPI 10 Court staff should be able to direct members of the public to the correct courtroom
KPI 11 Paper-based listings should be displayed in courts – on entry and on the courtroom door, indicating the number/name of the hearing and the correct room number. (I think this is actually already required in theory, but it clearly isn’t happening in practice).
KPI 12 When observers attend physical courtrooms, staff should be proactive in considering access needs.
E. Remote observation and livestreaming
20/. How could the process for gaining access to remotely observe a hearing be made easier for the public and media?
Supporting public access to remote court hearings needs to start by improving the listings (see section C above) – since we can’t email asking for the link if we don’t even know that a hearing is happening.
Then someone needs to answer our emails promptly and send us the link. Very often, nobody replies to emails (or phone calls) requesting access, or responses come too late, after the hearing is started, or after the hearing is finished.
Here’s an example. I tweeted about this case because I was pleased to see that a hearing before a Tier 3 judge (on circuit in Teesside) was properly listed in the Court of Protection list: that’s a rarity (see Section C above). But then dismayed to find that despite two emails and a phone call (unanswered), I was unable to gain access.
I don’t take not getting a reply personally – I’ve seen how common it is and appreciate that the root cause is understaffing, but I have spoken to members of the public who’ve requested access to hearings (often on multiple occasions) and had no response – and some of them do take it personally, and it creates a very negative impression of open justice in the COP. This negative experience has particularly affected members of the public who wanted to observe COP hearings because they are family members of vulnerable people involved in Court of Protection cases – and were left feeling that they were excluded because of their own family COP hearings. I’m fairly certain that this was not the case (apart from anything else, it would require an unusual level of organisation and cross-checking) – but this (recurrent) experience creates a very poor public relations effect.
In the case described above (before Mr Justice Poole) court staff sent an email later, after the hearing was finished, apologising for having been “unable to process your request in time” and saying “sorry for the inconvenience”. I responded to what I experienced as this rather ‘casual’ approach by explaining that failure to admit a member of the public to a “PUBLIC” hearing is not so much a personal inconvenience as a derogation from a fundamental principle of justice in a democratic society. To be fair, I expect the office was understaffed and he had a million other things to do that morning. I know that when tasks have to be prioritised, open justice never seems to be near the top of the list. The solution might be to fund the justice system better and to employ more staff (and address their training needs).
Judges also sometimes delay giving us access to public hearings (or refuse it altogether) based on misguided efforts to ‘screen’ observers. Some examples:
Recently I’ve been asked by a couple of different judges to confirm that I’m an accredited journalist or legal blogger as the ‘price ‘of admission. This is an unintended consequence of the Transparency Pilot in the Family Courts, which has backfired on transparency in the Court of Protection. (For one such example, see Just another failure of open justice: DJ Bland in Lancaster County Court.)
Several judges have asked would-be observers to provide their reasons for wanting to observe, or asked for home addresses (for remote hearings!), or demanded the name of the would-be observer’s employer.
One judge, whose hearing had been listed as “public”, circulated my request for the link (which he treated as a request for ‘permission to observe’) to the parties in advance of the hearing asking for their views. He didn’t hear back from them before the hearing, so didn’t arrange for me to receive the link.
One judge sent a message saying that I could be admitted to the hearing if I downloaded, printed and signed an “attendance form”, which I was instructed to scan and return in advance of the hearing in ten minutes time. No “attendance form” was attached – and by the time this was sorted out he declined to admit me because I was late for the hearing.
Complaints – from judges and court staff – that we ask “too late” to join hearings are quite common – where “too late” means after working hours the day before the hearing. They say they don’t have time to deal with our request. But we usually can’t apply any sooner than that, because lists don’t appear until 4.30pm the day before. We’re tried to explain this here: Why members of the public don’t ask earlier to observe hearings (and what to do about it).
Also, I spend a lot of time (up to an hour for some hearings) “waiting for the conference host to join” in the waiting room, anxious about whether or not I’ve been sent the right link (once I was on one link, the judge on another, and counsel on a third!), or whether anyone knows I’m there. Hearings often start late and presumably (at least sometimes) the lawyers know this because the judge has told them, or the judge knows this because s/he gave the lawyers permission to start late in order to continue a pre-hearing meeting – but nobody tells observers. Some communication to let us know what’s going on would be helpful. Lots of observers give up and assume they’ve done something wrong and are not going to be admitted to the hearing.
This all has a chilling effect on open justice.
KPI 13. When we email asking for access to a remote hearing, please could someone reply to our emails in advance of the time that the hearing is listed to start – even if just to say the hearing has been vacated or will be starting late.
KPI 14. Judges need to be clear about the Court of Protection rules for admission to public hearings. We are not required to be accredited journalists or ‘legal bloggers’; we are not required to provide home addresses or names of employers, or give reasons for wanting to observe, or sign attendance sheets.
KPI 15. My recommendation: If a hearing is listed as ‘public’, court staff should send us the link immediately (letting the judge know they’ve done so) without waiting for the judge to “consider our request” or “give permission” – since really, in the vast majority of cases, there is nothing to consider and no “permission” is required. I have also suggested to HMCTS that links could be published in the listings, thereby obviating the need for us to ask for them in the first place. I didn’t understand the explanation of why this can’t be done. If some consideration is, in fact, needed (e.g. if one party objects to observers, despite the fact that the hearing has been listed as public) then that consideration can happen at the beginning of the hearing and observers can be part of it – and then leave the platform, if necessary.
F. Public access to judgments
27/. In your experience, have the court judgments or tribunal decisions you need been publicly available online? Please give examples in your response.
No. This is a particular problem when there is no oral ex tempore judgment in court. We’ve often been waiting for judgments to be handed down and then some days after a hearing finishes, the RCJ website listing tells us that the judge will hand down the judgment “in public” at 10.30am but there’s “no attendance”. I think this just signals that this is the date and time at which a judgment is – or should be – “final” and therefore publicly available. But it’s usually impossible to get hold of it. I’ve been told many times that it will be published on BAIILI and/or The National Archives and I can read it then – and sometimes this happens within an hour or two of the judgment being “handed down in public” but sometimes it doesn’t happen for days or even weeks. It doesn’t make any sense to me for a list to say that a judgment is being handed down in public, but for it to be inaccessible to me for hours, days or weeks until someone puts it up on a public website. I think I should be able to contact someone and get it at 10.30am. Occasionally, the judge has specifically asked for it to be sent to me, knowing that I’ve been following the hearing (which is excellent), but I frequently pursue it without success.
On two occasions I’ve observed hearings before a Tier 3 judge (in both cases, Poole J) which dealt with ongoing matters previously decided before a less senior judge whose judgments had not been published. I asked, in the interests of transparency, for these judgments to be made publicly available and Poole J acceded to my request and they are now accessible to everyone. Publication of these two judgments was very helpful in supporting public understanding of these two cases and was a very positive move in the direction of open justice.
KPI 16. When judgments are “handed down in public” (according to court listings) they should be available to members of the public immediately.
KPI 17. When a member of the public asks a judge to consider publication of a judgment, that request should be taken very seriously.
G. Access to Court Documents
41/. As a non-party to proceedings, for what purpose would you seek access to court or tribunal documents?
I regularly seek access to court documents in order to help me follow a hearing and to support accuracy of reporting.
I request the skeleton arguments, or position statements, prepared in advance by the parties – since these usually underpin oral argument in court, even when they are not explicitly referenced. These are rarely offered – but when I request them, I tend to get them more often than not. As was said two decades ago, “ … the principle of open justice leads inexorably to the conclusion that written skeleton arguments, or those parts of the skeleton arguments adopted by counsel and treated by the court as forming part of his oral submissions, should be disclosed if and when a request to do so is received.” (Howell & Ors, v R. [2003] EWCA Crim 486 (28 February 2003)).
I’ve also requested final orders from public hearings – to which I believe I am entitled as a matter of law. It’s actually quite difficult to get these (compared with Position Statements) because the final Order isn’t approved by the judge on the day of the hearing, but several days later, by which time the judge (and the lawyers) have turned their attention to other matters and forget that I’ve asked.
Other documents I’ve been sent on request include: written closing statements, an EasyRead version of “what this court case is about” prepared for a P with learning disabilities; stand-alone “Summaries of the Case Law” documents (agreed by all parties); a restraint plan; and witness statements from family members who wanted to share them.
Court documents always help my understanding of the case and provide richness and texture to my reports.
KPI 18. If we ask for court documents, they should be sent in a timely fashion. If anonymisation is required, do it before the hearing so as not to create delay.
It’s worth noting that (for remote hearings in particular) we often don’t receive Transparency Orders – the injunction the court is supposed to serve on us regarding reporting restrictions. I only ever receive them for about 50% of hearings. Another member of the core Open Justice Court of Protection Project team has gone systematically through the 38 hearings (across 32 cases) that she’s observed: she has 14 (= 38%). One important reason for the failure to send Transparency Orders to members of the public is because it does not seem to be anyone’s (agreed) job. According to Senior Judge HHJ Hilder, “It is not Counsel’s role to provide orders. This is an HMCTS role.”, HHJ Hilder, Item 8 Minutes of COP User Group meeting, 20 April 2022), but when I’ve asked court staff, I rarely get them: either there’s no response at all, or court staff say they don’t have them and I should ask the judge. In practice, when I do get them, they’re overwhelmingly sent by counsel. Other practical impediments to sending us Transparency Orders include: nobody knows how to separate out the Transparency Order from the rest of the electronic bundle; and (absolutely routinely) counsel and their instructing solicitors have the Transparency Order, but not the observers’ email addresses, while court staff have the observers’ email addresses, but not the Transparency Order. Counsel sometimes ask me to forward Transparency Orders to other observers (on the false assumption that I’ll always know who the other observers are). I don’t know why this hasn’t been sorted!
KPI 19. Transparency Orders should be sent to all observers – we need to be clear about what the reporting restrictions are. In order for this to happen it needs to be part of someone’s job description and there needs to be a practical mechanism for doing it.
H. Public legal education
My experience is that the public has very little understanding of the justice system, and that this applies even to people working with the Mental Capacity Act 2005. We have learnt a huge amount ourselves in running this Project.
People struggle with understanding the language and concepts of the court – and also taken-for-granted aspects of court protocol, such as the order of speaking, the role of cross-examination, the function of expert witnesses, even what constitutes a judgment. There’s a huge amount of public education to do here.
58/. Do you think the public has sufficient understanding of our justice system, including key issues such as contempt of court? Please explain the reasons for your answer.
One of the core team members of OJCOP, NHS Consultant Clinical Psychologist Claire Martin says: “Absolutely not! I don’t think professionals know very much either – especially in the health service, which is my area of knowledge. We get very little training on the Mental Capacity Act 2005 and unless you are working with capacity all of the time – and involved in CoP, which most people aren’t, even if they use the MCA regularly – you won’t know much! My experience of observing the COP has taught me how little I knew beforehand. Unless you really make it your business to educate yourself, the baseline way of operating is with a global view of ‘capacity’ – I can’t count how many times I’ve read in patient notes, from medics as well as nurses, that someone has/does not have ‘capacity’ – and with ‘best interests’ operationalised as ‘what I/we think is best for this person’”.
On contempt of court in particular, this is something I am still learning about three years on. As part of my commitment to working effectively on this Project, I’ve done an online course on media law (aimed at journalists) which left me with the impression that (since our Project doesn’t cover jury trials) there were minimal risks of anything we write unfairly influencing a court case. My media law course, like the government’s own website focused on criminal hearings. Then I got an e-mail from Mostyn J suggesting I may be in contempt of court for publishing a blog post (by another member of the public) expressing opinions about a hearing before him while proceedings were still active. The judge suggested that there was “a not insubstantial (but real) risk … that the course of justice in the proceedings would be impeded or prejudiced, in that the mind of the court may have been subconsciously influenced on reading the post”. Partly as a consequence of that experience, I decided, at a subsequent fact-finding hearing (before Hayden J), against publishing a blog post in which members of the public expressed opinions about the ‘evidence-so-far’ from witnesses, until all the witnesses had completed giving evidence (Adjournment and interim judgment – Hayden J’s fact-finding hearing). I’m still not sure how ‘contempt of court’ might operate (or not) in either case – but it’s all been very educational, and something I am blogging about, thereby also supporting public education on ‘contempt of court’.
60/. What do you think are the main knowledge gaps in the public’s understanding of the justice system?
From the perspective of our Project: the existence of the Court of Protection and its role, why and how to make applications, what happens if you find yourself as a party especially as a LIP)or as “P” (there’s very little accessible information about this); the ‘inquisitorial’ rather than ‘adversarial’ nature of the court; its dependence on the MCA 2005. And all the individual details that make up a court hearing, most of which diverge markedly from the (largely American, largely criminal) trials that pervade the media.
Judges are increasingly taking the time to explain terminology and concepts, to read out (or display on screen) crucial evidence, and generally taking care to facilitate and support public understanding. This takes time and commitment. It has to be subordinated to, and run in parallel with, the substantive business of the hearing. It’s evolved over time, as a collaborative effort between those of us who want to learn, and members of the judiciary and lawyers who are sufficiently committed to open justice to help us with that. It’s a long way from the ‘fly on the wall’ notion I started out with at the beginning of the Project.
KPI 20. Every court hearing is also an opportunity for public legal education.Use it!
I. Closing Summary
Nothing in this document should lead readers to underestimate the huge amount of time and effort that lawyers and the judiciary (plus staff) of the Court of Protection have expended on open justice – both before and (especially) after the founding of our Project. Nonetheless, I have become concerned that the success of the Open Justice Court of Protection Project might lead to a sense of complacency – that the requirements of open justice are apparently met, as evidenced (for example) by our blog posts. I hope that by exposing what it takes to run the Project and the ‘workarounds’ we rely on to make any of this happen, the systemic failures of open justice can become clear – not in spite of the Project’s achievements, but because of them.
If the 20 KPIs listed in this document were met (and some of them are already!) the experience of members of the public observing hearings in the Court of Protection would be immeasurably improved. Meeting these 20 KPIs (or just most of them) would go a long way towards practical implementation of the judicial aspiration for transparency and open justice in the Court of Protection.
KPI 1. List the hearing in the COP list on Courtel/CourtServe (or whatever replaces it – where ever is displayed what is supposed to be a comprehensive list of COP hearings).
KPI 2. Make it clear the public can attend.
KPI 3. Tell us how we can observe (i.e. remotely /in person – is it hybrid? if remote is it phone or video-link (MS Teams or CVP)?.
KPI 4. Supply correct contact information.
KPI 5. Tell us what the hearing is about.
KPI 6. If the court is going to hold hearings with the deliberate intention of excluding one party (usually a family member) (‘closed hearings’), there needs to be more public accountability for this so that we at least know that it is happening, how often, and why (e.g. an annual report covering the number and nature of ‘closed’ hearings, and the reasoning behind them).
KPI 7. Hearings at which the court is deciding whether or not an alleged contemnor should be sent to prison should normally be listed in accordance with the Practice Direction, held in public and a judgment published.
KPI 8. The courts should be properly resourced so that there are trained staff availablefirst thing on the morning of a listed hearing to answer questions about whether it is actually going ahead or whether it has been vacated.
KPI 9. Court staff should remove any signs on courtroom doors stating that hearings are PRIVATE when they’re not. We recommend replacing it with a sign that says “THIS HEARING IS IN PUBLIC. EVERYONE IS WELCOME TO COME IN”.
KPI 10. Court staff should be able to direct members of the public to the correct courtroom
KPI 11. Paper-based listings should be displayed in courts – on entry and on the courtroom door, indicating the number/name of the hearing and the correct room number.
KPI 12. When observers attend physical courtrooms, staff should be proactive in considering access needs in relation to disabilities and more broadly.
KPI 13. When we email asking for access to a remote hearing, we should get replies in advance of the time that the hearing is listed to start – even if just to say the hearing has been vacated, or will be starting late.
KPI 14. Judges need to be clear about the Court of Protection rules for admission to public hearings. We are not required to be accredited journalist or ‘legal bloggers’; we are not required to provide home addresses or names of employers, or give reasons for wanting to observe, or sign attendance sheets.
KPI 15. If a hearing is listed as ‘public’, court staff should send us the link immediately (letting the judge know they’ve done so) without waiting for the judge to “consider our request” or “give permission”.
KPI 16. When judgments are “handed down in public” (according to court listings) they should be available to members of the public immediately.
KPI 17. When a member of the public asks a judge to consider publication of a judgment, that request should be taken very seriously and acted on unless there are good reasons to the contrary.
KPI 18. If we ask for court documents, they should be sent in a timely fashion. If anonymisation is required, do it before the hearing so as not to create delay.
KPI 19. Transparency Orders should be sent to all observers – we need to be clear about what the reporting restrictions are. In order for this to happen it needs to be part of someone’s job description and there needs to be a practical mechanism for doing it.
KPI 20. Every court hearing is also an opportunity for public legal education. Use it!
***********
Celia Kitzinger is co-founder of the Open Justice Court of Protection Project and has personally watched more than 470 Court of Protection hearings since 1 May 2020. She is a prolific blogger. She is on LinkedIn (here), and tweets @KitzingerCelia
By Amanda Hill, formerly ‘Anna’ , 3rd September 2023
When I saw this case listed, I didn’t fully appreciate the complex issues it would cover, especially about the difficulties of ensuring that somebody who is used to going out independently can do so safely – and the role that technology might play.
At the heart of this case is a woman I’ll call Sarah (I find the term P too anonymous and I like to try and visualise the person behind the letter P). Sarah is a 41-year-old woman diagnosed with Asperger’s syndrome (a form of autism), bipolar affective disorder, atypical anorexia nervosa, obsessive compulsive disorder and severe anxiety. She’s living in supported living, and she’s been accustomed to having a good degree of autonomy, including being able to go out into the community by herself.
However, there are now concerns about a man she has met who may have “groomed and sexually exploited” her, and it has been suggested that she may lack capacity to decide on contact with others and engage in sexual relations. This is the third time over the last few years that she has been exploited by a man. An initial assessment by her social work team was that Sarah “was unable to understand, retain and use/weigh relevant information relevant to the decision” to engage in sex. There is now an ongoing criminal case against the man and concerns for her safety.
After this, and without court authorisation, the local authority increased the 1:1 provision of carers, and prevented her from going out in the community alone. She objects to these restrictions on her freedom. Observing these hearings highlighted to me the practicalities of managing the difficult balancing act between the principle of autonomy at the heart of the Mental Capacity Act 2005 and the principle that vulnerable people in society must be protected.
The case (COP 14088706) was listed with the subject matter as ‘Capacity to Consent to Sexual Relations’. I don’t have much knowledge about the law in relation to capacity for sex (I’ve learnt a lot writing this blog post) and it wasn’t because of the topic that I chose to observe this hearing. Rather, in my role as a core team member of the Open Justice Court of Protection Project, I am focusing on hearings in the South East Regional Hub where the lead judge is HHJ Owens and, as she was the judge in this hearing, I thought I would observe it. The hearing did cover other areas that I do have a particular interest in, such as the role of Litigants in Person and Deprivation of Liberty – and, having previously focused largely on s.21A cases, because this is what my own mother’s case was about, I’ve discovered that I can learn a lot through observing COP cases concerning a variety of different issues.
I’ve observed two hearings in this case: one on Monday 17th July 2023 and another on Wednesday 9th August 2023. I received the Position Statements (PS) for both hearings from Oliver Lewis after the hearings, which greatly enhanced my understanding and which I have drawn upon when writing this blog. In fact, without them, I don’t think I would have really understood the case at all.[1]
1.Hearing of 17th July 2023
Access was straightforward and I was sent the Transparency Order in advance. The Clerk gave me access to the video-platform at 1.55pm (for a 2.00pm hearing). There were already a number of people attending. I could see Oliver Lewis of Doughty Street Chambers who was Counsel for Sarah via her litigation friend, the Official Solicitor (OS); Sebastian Elgueta of Garden Court Chambers who was Counsel for the Local Authority (LA); and two people who I learned were Sarah’s parents. Various other people joined after me, including the solicitor for the LA, the solicitor for the OS, a trainee solicitor and Sarah’s social worker. Sarah was not present, either at this hearing or the following one, I don’t know why. This means that we didn’t hear her voice directly. The clerk asked everybody in turn (including me) to confirm that they could see and hear him. I turned my camera and microphone on so he could see me, and I replied I could. Then I switched my camera and microphone off.
Then something happened that quite surprised me. Before the judge joined the platform, Oliver Lewis spoke directly to Sarah’s parents (who I shall call Dr and Mrs G) and because they had not taken part in pre-hearing discussions, asked them if they would like to be joined formally as parties to the case. They asked him to explain what that meant. This is something I know a bit about, as I asked to be joined as a party for my mother’s case, as I wrote about here. I was interested to know how it would be explained. Oliver Lewis explained that Sarah was a party to the case and had a litigation friend to represent her. They, her parents, were currently not parties to the case and so were not automatically entitled to receive all the information relating to the case (“the bundle”) or have their opinions heard. If they were joined as parties, they would play an integral role in the proceedings. Dr and Mrs G said that they would like to be joined as parties. Oliver Lewis explained that it would be up to the judge whether they needed to fill out an application form or if the judge could decide that they could be parties without the need to fill in the form. He then went on to explain that the hearing was about appointing an independent expert to determine capacity for “a range of capacity issues”. Mrs G said that the explanation was “very helpful”.
He then explained that the expert could cost between £2,000 and £3,000 and the cost would normally be shared between the parties, so that was a potential disadvantage to becoming a party. But if they didn’t have the means to contribute, they could ask the judge to excuse them from paying. (NB: In that case, the cost would be divided between the LA and Sarah, who is in receipt of Legal Aid). Oliver Lewis apologised to the parents for the “technical” nature of “all this”.
At 2.05pm the judge joined and made some introductory remarks about this being a formal hearing in a courtroom (even though it was online). She said that there was an observer present and reminded everyone about the Transparency Order preventing Sarah from being identified.
She next addressed the issue of Sarah’s parents becoming parties to the case, explaining (as had Oliver Lewis) that they would not be entitled to see all the documents if they were not joined as parties. Dr G said “We would like to ‘join’, if that’s the right word, but we are worried about the cost”. I thought at this point he was referring to the point made before the judge joined about the cost of the expert. However, in her reply, the judge referred to them not needing formal legal representation and that the court could assist Litigants in Person. She said “You are known as a Litigant in Person and we have an obligation to help you”.[2] The parents stated that they did want to be joined as parties. The Judge said it was clear that the parents have a personal interest in Sarah and what happens to her and she could see the benefit of them being involved. She waived the requirement for a formal application and said they would be joined as parties from that point on. As they had not been parties before the hearing, they had not seen “the bundle” of documents – so she asked Sebastien Elgueta to explain what the hearing was about. He apologised for not having formally submitted a draft order, and he then set out what would be in it.
As far as I know, there is no easy leaflet or resource for families on becoming an LIP in the Court of Protection, which I think would be really useful. I certainly wanted to feel fully informed before I became a Litigant in Person.
Some points about the style of the hearing
There were some IT issues during this hearing. At one point, Sebastian Elgueta dropped off the call (later apologising for the “IT meltdown”) and the judge rose for a few minutes and left the video platform. While we were waiting for her to return, Oliver Lewis spoke to Dr and Mrs G: “Are you OK? Is there anything you want to ask?” I thought this was very thoughtful of him. The judge and Sebastian Elgueta re-joined the call a few minutes later. Oliver Lewis gently pointed out to the social worker that she was not on mute. HHJ Owens was also very sympathetic to Sebastian Elgueta about his IT problems. The way that this episode was handled indicates the generally amiable spirit that the case was conducted in, which I think helped discussions in what are very difficult circumstances.
As a family member myself in COP hearings, I was interested in how the parents were treated. At points, I suspect reference to sections of the Mental Capacity Act 2005 would have been difficult for the parents to follow. At one point Dr G stated that Sarah’s mental health would decline if “getting an assessor (if that’s the right word)…..” took a long time, showing that language very familiar to professionals can be more difficult for lay people in the court to understand. That’s why it’s so important to explain things simply for parties who are lay people, something that can be lost with the time pressure of a hearing. Overall, I thought the parents were treated very well in the hearing, particularly by HHJ Owens and Oliver Lewis. Interactions were personable and done in a way to put people at ease. Even I was made to feel welcome as an observer. In my experience, this is a common feature of the COP, although obviously it is dependent on the personalities and style of the legal teams and the judge.
The substance of the hearing: Capacity to engage in sexual relations
Given that this case raised potentially very serious issues, the judge explained that she had had a gatekeeping concern which she took to the Vice President of the COP in early June 2023. There were question marks about Sarah’s capacity to make decisions about contact[3] with the man she was seeing (whom I shall call Mr Grey) and the risk he posed (which was information that would come from the police). The position of the Official Solicitor was that there seemed to be uncertainty as to what exactly the LA were asking the court to approve at this hearing, but the OS was concerned about how much Sarah’s autonomy was restricted in order to protect her. Sarah wants to continue to see the man, even if it is with a support worker.
Reading the PS of Oliver Lewis on behalf of the OS, I understand that the OS agreed that on the basis of an assessment done by a social worker, there was sufficient evidence to cause the court to have reason to believe that Sarah lacked capacity to engage in sexual relations. However, the OS disputed that there was good enough evidence to override the presumption of Sarah’s capacity in other areas, such as decisions relating to her residence, to consent to her ‘de facto’ deprivation of liberty, or to make decisions about contact with others, including Mr Grey.
So, although the hearing was listed as “Capacity to engage in sexual relations”, it became clear that it was about capacity to make decisions in various other domains as well. The OS was seeking to ensure that the LA’s view that Sarah lacks capacity for sex wouldn’t lead to an unlawful restriction of her rights in other areas. It seems that the OS was trying to ensure each domain was considered appropriately. And it was all urgent as imposing new draconian restrictions on someone’s liberty, such as an increase in 1:1 support hours for Sarah (to 105 hours from 48 previously) can’t be justified unless they’re absolutely necessary.
Therefore, the OS submitted on Sarah’s behalf that “there needs to be a comprehensive capacity assessment carried out by an independent expert (if there is no person in the local Trust able to do a report under s.49, and enquiries are being made) to assess capacity to make decisions about (a) residence, (b) care, (c) contact with others, (d) engaging in sexual relations, and (e) contraception”.
On behalf of Sarah, Oliver Lewis said (in his PS): “It is unfortunate that (Sarah’s) freedoms on a daily basis are proposed to be curtailed because of the sudden appearance in her life of (the individual). The Official Solicitor invites the court to scrutinise the necessity and proportionality of the proposed care arrangements.”
It was also stated that the individual is the third man who seems to have posed a risk to Sarah as a vulnerable adult in the last few years.
I wasn’t entirely sure what ‘Capacity to engage in sexual relations’ covers but it is a fundamental principle of the Mental Capacity Act 2005 that each person is presumed to have capacity unless it is established that they lack capacity ( s.1(2)) and a lack of capacity to make a decision cannot be established simply by reference to some ‘condition’ that a person has (e.g. mental illness) (s.2(3)(b)). It must be shown that the “impairment of, or a disturbance in the functioning of, the mind or brain” (s.2(1)) causes the person to be unable:
(a) to understand the information relevant to the decision,
(b) to retain that information,
(c) to use or weigh that information as part of the process of making the decision, or
(d) to communicate his decision (whether by talking, using sign language or any other means). (s. 3(1) MCA 2005)
The courts have warned about setting the bar for capacity for sex too high since this could operate as an unfair, unnecessary and discriminatory bar against mentally disabled people. It’s also been stated that the person must understand the salient information but it is not necessary for them to understand all the peripheral detail (LBC v RYJ [2010] EWHC 2665).
What counts as ‘relevant information’ depends on the decision being made and the circumstances of the case. In relation to sexual contact, a recent decision by Lord Justice Baker in the Court of Appeal (A Local Authority v JB (Rev 2) [2020] EWCA 735) found that the relevant information includes: the mechanics of sexual intercourse, the fact that both people must have capacity to consent (and must in fact consent), that pregnancy is a reasonably foreseeable consequence of (heterosexual) intercourse, and that there are health risks involved such as sexually transmitted diseases, the risks of which can be reduced by use of precautions such as a condom.”
The following issues were also discussed during the hearing.
Appointing an IMCA for Sarah. Oliver Lewis proposed that an independent mental capacity advocate (IMCA) be appointed for Sarah as “even if her parents love her very much”, Sarah might not want to discuss her sexual relations with them. The judge agreed and said it could be “vice versa” too. I found this a very human exchange. I learned afterwards that IMCAs were introduced by the Mental Capacity Act 2005 (ss. 35-41) and their role is to support and represent the person in the decision-making process.
Sarah’s mental health. At various points during the hearing, issues were raised showing concern for Sarah. Her parents said they were worried about the impact on her mental health of more delays in the assessment. Also, it seems that Sarah has to be accompanied at all times by a carer, even going to a café, and her parents were concerned that this was depleting her financial resources as she had to pay for the carer’s travel and coffees. Later in the hearing, after the judge had left to consult her listings team, Sarah’s solicitor returned to this point and suggested that the care should be provided within her existing care package. The parents confirmed that it was actually the additional cost of the coffee and meals for the carers that she was obliged to pay for. There was also a discussion about whether the police would be called in a particular situation, which was proposed by the LA in the draft care plan. Sarah’s parents said that she was terrified of the police as she had been chased by them once and she had found it very traumatic. On one occasion, they said, it had resulted in her being sectioned. The judge talked about necessity and proportionality of calling the police and it was removed from the care plan.
Urgency vs practicalities. It was clear that getting the care needs assessment (and a care plan proposed) was urgent as this had implications for the DOL. This was partly for Sarah’s mental health but also for her protection. After much discussion, HHJ Owens authorised 21 days for the identification of the expert to determine capacity, so that they could be appointed by the judge, and for a new care plan to be drafted in time for the next hearing on Wednesday 9th August 2003.
2. Hearing of 9th August 2023
On requesting the link the evening before the hearing, I was surprised to get a quick reply from the Administration Officer, telling me that HHJ Owens had asked her to let me know that there was a doubt over the start time but they would clarify the situation the following morning. Mid-morning the following day, the Administration Officer got back to say the hearing was to be in two parts: the first part, to start as listed at 2pm and to last 45 minutes, was going to be an “injunction application subject to reporting restrictions” and then the second part of the hearing was to last 95 minutes, being the “main COP proceedings, again subject to reporting restrictions”. I checked whether I could observe both parts and was told I could.
I was shortly sent the link and a new Transparency Order (TO). The difference between this one and the previous one was that not only could I not identify P, the protected party (Sarah) but also not the man who was to be the subject of the injunction (Mr Grey).
Injunction application
I clicked on the link a few minutes before 2pm and was soon admitted to the hearing. This time I could see the clerk and another person in a physical court room. The clerk again asked me to confirm that I could see and hear him, which I did, before turning my microphone and camera off. Unlike the previous hearing, nobody else joined until 2pm and then nearly everybody else joined at once. I soon gathered that this was because there had been a pre-hearing meeting attended by most of the others. Most people were using the Cloud Video Platform and included:
Oliver Lewis representing Sarah via her litigation friend, the Official Solicitor (OS)
Avril Rushe, Counsel for the LA (replacing Sebastian Elgueta, who was at the previous hearing).
Dr and Mrs G (Sarah’s parents and Litigants in Person)
There were also two instructing solicitors, Sarah’s Social Worker, and a mini-pupil with Dr Lewis.
There was also a man who had joined by telephone: Mr Grey.
Each person in turn was asked to confirm they could see and hear the Clerk. Then, at 14.08, HHJ Owens, the judge, joined the hearing.
Once again, the judge started by telling everyone that they should behave as if it was a physical hearing, that there was a TO in place and there should be no recording of any sort allowed. She stated that there was an injunctive order affecting this hearing, Mr Grey was not to be identified, there was a police investigation under the Sexual Offences Act going on in the background which was outside her jurisdiction.
This was a very stern warning given by the judge and my impression was this was so that the police investigation would not be compromised. HHJ Owens asked Mr Grey to confirm that he understood he was the subject of injunctive relief, and of the TO, which prohibits identification of Sarah and himself. She also mentioned that I was a member of the public and an observer, that I had been sent the TO and had observed the previous hearing – but I wasn’t asked to confirm this orally.
In her introductory summary, Avril Rushe explained that this was an application for an injunction against Mr Grey under s.16 of the Mental Capacity Act and the jurisdiction of the Court of Protection (COP) was the test of whether it is just and convenient for an injunction to be made against Mr Grey because he was a risk to Sarah. There was an ongoing police investigation against Mr Grey for alleged sexual assault against Sarah. He is on bail with a condition that he is not to contact Sarah, which is due to expire at the end of August and that may be extended. However, the bail conditions by the police were less robust than those that could be imposed by the COP, so they are asking for a court injunction against Mr Grey. There had been a wide-ranging injunction proposed originally but they were now proposing a “pared back” injunction as that would be more proportionate. This was that Mr Grey:
Must not speak to, call, text, email, or contact via social media (etc.) Sarah or any person involved in her care
He must not enter any property he believes Sarah would be in.
An open injunction was asked for (I gather this means with no fixed ending).
HHJ Owens asked about prohibiting Mr Grey from contacting Sarah via a third party.
Avril Rushe said that this was not being sought because there was no evidence of Mr Grey attempting to use a third party to contact Sarah.
The judge then stated that there was no current evidence, but what if that changed? She then asked Avril Rushe if Mr Grey could make oral submissions to the court and Ms Rushe confirmed that he could and that he had not seen the new terms of the proposed injunction.
The judge then asked all parties involved in the main Order to speak and said that after that she would hear from Mr Grey.
There was then a discussion because Oliver Lewis had not been sent the version of the Order that the judge had in front of her, so the judge offered to read out the new version of the Order that she was being asked to approve:
The proposed injunctive relief Order warns Mr Grey that he will be in contempt of court, which means he could have his assets seized, be fined or sent to prison (or all three, as she emphasised). Once the court has heard from all the parties and oral submissions from Mr Grey, the court decided that it is in Sarah’s best interests not to have any contact with Mr Grey and that he must not speak to, email, text or contact Sarah or any person involved her care and must not enter any property she is likely to be in, and the injunction would last until further order of the court.
She then asked if there was anything else on behalf of the OS. Oliver Lewis asked that full names be included rather than abbreviations in the order, to avoid any confusion for Mr Grey. HHJ Owens said that would be no problem and with the TO in place that would avoid issues with identification.
HHJ Owens then asked Dr and Mrs G if they wanted to say anything about the injunctive application and they replied “No, thank you”.
The judge then turned her attention to Mr Grey. She went through what he was being prohibited from doing and he replied “I won’t speak to her, I won’t have anything to do with social workers, I won’t be going to her home or place of work so I agree with them”.
HHJ Owens then stated that “It goes a little wider than that”. She reiterated that he should not speak, telephone, or attempt to contact Sarah in any way whatsoever, including Facebook, even via friends and in indirect form.” She also asked Avril Rushe whether as well as the social workers, should it be specified that Mr Grey be prevented from contacting Sarah’s parents? Avril Rushe confirmed that – and HHJ Owens stated that she would change the injunction accordingly.
She then returned to Mr Grey.
“And Mr Grey, any premises where you believe she might be. So, if you believe she could be anywhere, you must walk away”.
Mr Grey said “I understand”.
The judge then confirmed that the order would be “indeterminate” and he replied “Yes, I agree, as it’s not going to happen”.
HHJ Owens then said “That’s good, but the Order says that you mustn’t do it” and once again she outlined about contempt of court and what that entails.
She continued “So, Mr Grey, thank you for agreeing to this. I am satisfied that it is in Sarah’s best interests not to have contact” and then referred to wording that would be slightly different to the draft order.
She stated that “Mr Grey is prohibited from attending any further public hearing” so as to protect Sarah.
Mr Grey was then disconnected from the hearing and the Clerk confirmed that he was no longer present.
At this point, HHJ Owens suggested to Avril Rushe that she would need a sealed copy of the order sooner rather than later so she would rise to re-write it, and ask the COP hub to issue it so that it could be issued to Mr Grey as soon as possible. Avril Rushe confirmed that this would be “greatly appreciated”. HHJ Owens rose at 14.32.
She came back at 14.53. This time there were no discussions between the other attendees as everyone waited, some with cameras on and some with cameras off. On her return the judge confirmed that she had “perfected” the injunction, emailed the draft approved order to the hub and rang them to ask them to do it quickly and for the TO “to be appended”. She finished with that hearing by thanking everyone for their patience but “I thought it was important to deal with it now”.
At this point the court moved on to the “substantive hearing” about welfare.
I had never observed a hearing where an injunction had been placed on somebody, not least when they were present. I was conscious of how the need to keep Sarah safe and as quickly as possible was paramount, to the extent of HHJ Owens ensuring the injunction could be served immediately. The judge was very clear to Mr Grey about what would happen if he ignored the injunction.
This second part of the hearing essentially comprised two elements: the appointment of an independent expert acceptable to all parties and Sarah’s care and support plan.
Appointing an independent expert
The first element was non contentious. An independent expert (Dr Camden-Smith) had been identified who had agreed to do the assessment and provide a report for the beginning of November 2023. I learned from the PS that the letter of instruction would be written within a week of the court “agreeing the identity of the expert”. There was some discussion about what would be included in the letter of instruction, including asking the expert to diagnose whether Sarah has a learning disability – which is important because she does not currently have such a diagnosis and is therefore excluded from some health services such as sexual education.
The OS’s PS shed further light on what exactly the expert was being asked to report on and the following paragraph caught my eye: “In addition to the capacity assessment and review of diagnoses, the Official Solicitor seeks from Dr Camden-Smith an opinion as to steps the carers and the family could take to encourage Sarah to engage with activities for a sustained period, so that she builds her skills and has meaningful activities to look forward to on a weekly basis. This would decrease the risk that she rides around on buses on her own where she has now been groomed by three different men.” This underlines to me how important the role of the independent expert is and how much finding the right person counts as the impact on Sarah’s future, both in terms of freedom and safety, is immense. It also highlights to me the vulnerability of women like Sarah, who strive to live freely but may not appreciate how at risk they are.
Later on in the hearing, the judge scheduled a further hearing for 19th December 2023 to consider the report from the expert. But this meant that what should happen in the meantime had to be considered. Avril Rushe outlined that the LA was asking the judge to make best interests decisions under s. 48 of the Mental Capacity Act 2005, as there was ‘reason to believe’ that Sarah lacks capacity to engage in sexual relations (which would be confirmed or not by the expert’s report). The OS did not contest this and it was indeed ordered by the judge at the end of the hearing.
A new care and support plan
The second element, Sarah’s care and support plan, proved to be a much more contentious issue. In order to try to protect Sarah when the incident with Mr Grey had occurred, the LA had increased the number of hours of 1:1 support from 48 to 105 per week, without the authorisation of the court. Sarah’s social worker had subsequently produced a new care and support plan outlining a gradual reduction in hours from 105 to 79 and eventually back to 48. But the OS was not happy with the plan and Oliver Lewis seemed somewhat frustrated with the way the case had been managed so far. He said he and his solicitor were confused about “what is written in the care plan, what is being delivered and what is being proposed”. He wanted the LA to draft a new care and support plan that was much simpler than the current draft which was in the bundle. He went as far as to say that he and his instructing solicitor could not understand what the care and support plan was. “It’s a mixture of thoughts and intentions but does not set out needs and how care is to be put in place to meet those needs, so that the OS can understand and Sarah can understand”. The judge appeared to agree that the plan could have been written better as she said later that “The document as a whole….is not clear”. And Avril Rushe representing the LA acknowledged that some of the details needed to be ‘fleshed out’.
Oliver Lewis outlined that Sarah is a person who greatly values her independence and autonomy and is now distressed that she doesn’t have freedom. She has said “I want my freedom back”. There was concern that unless the situation was resolved quickly, it could have serious consequences for Sarah’s mental health, something both the OS and Sarah’s parents were very concerned about. She had previously been sectioned under the Mental Health Act and everyone wanted to avoid this happening again. But what could be done to protect Sarah whilst giving her as much freedom as possible?
“Find my Device”: A technological solution?
The proposed solution surprised and slightly shocked me, even though I can see why it was being considered: the use of technology via a GPS tracker. The idea was that Sarah’s whereabouts could be tracked, allowing her to go out independently but with a type of security blanket. Some of the 1:1 hours allocated could be used to monitor the tracker. This solution was supported by the LA, the OS and Sarah’s parents, even though there was disagreement as to the practicalities of how the tracker would be used.
The social worker had met with technicians to discuss what was possible. It would show whether Sarah was near to places she had gone to with Mr Grey (his home and a particular pub) where she may be at risk. But it would not show if she was at risk in a new location. There was also a major concern about her using public transport to get to day activities or to spend time. It was agreed that Sarah had been groomed by three men on the bus over the past three years, and the LA wanted Sarah to be “chaperoned” on public transport, but the OS and Sarah’s parents felt that the use of technology would be the least restrictive option and more proportionate.
Oliver Lewis proposed that the use of an app such as the android “Find my Device” could be the simplest to use. He stated something along the lines of “ …as many parents all over the world know – and I’m not equating her as being a child – but the Find my Device app could be adjusted so she does not switch it off”. Before the hearing, he had discussed with Sarah’s parents how it might work and that it could be used as a bargaining chip, as a price Sarah would have to pay to go out alone. “That might work”. The OS thought 48 hours of care should be returned to as soon as possible, as this is in line with the wishes and feelings of Sarah. With regards to the risk, the carers could use the extra hours to monitor her phone rather than going with her, and see if she goes to places where she is at risk. He said that it shouldn’t need much time for the technology to be sorted out.
Urgency vs practicalities – again:
There was then some discussion about how soon a new care and support plan could be completed and when the next hearing to consider it should be listed for. The OS wanted it as soon as possible given Sarah’s deteriorating mental health. But there were practical difficulties, given the social worker’s availability to draft the plan as well as the judge’s annual leave and whether judicial continuity was essential. The eventual decision was that the next hearing would be listed for 4th September 2023 and HHJ Owens would hear it. (In the event, that hearing was vacated. I’ll keep a look out for when it next returns to court.)
In reaching this decision, the judge considered what was realistically feasible. She stated that there was a “tension between an ideal world and what was practicably achievable”. She directed the LA to provide a revised section of the care and support plan covering the use of technology. She stated that “None of us know what the impact of the injunction will be, regarding Mr Grey and Sarah” and- as had been flagged by Oliver Lewis in his PS – Sarah “reacts well to people in authority telling her what the rules are. The Official Solicitor suggests that it would reduce the risk of [her] seeking out [Mr Grey] if the judge or social worker phrases the best interests decision as a rule, by telling her “You must not try and find [Mr Grey]”. This may have the desired effect and would be a better way of ensuring that [Sarah] does not try to seek a meeting with [Mr Grey[.”
In consideration of the injunction, the LA was asked to reflect on what was proposed regarding technology as a replacement for 1:1 support or a partial replacement. The judge stated “none of us understand what might be practically achievable” as tracking on a phone only indicates location. But 1:1 support on public transport might function as a considerable restriction. Technology may answer that, as if it shows she is spending hours on a bus and at risk from men, then it might enable action to be taken so that she is discouraged from doing that. So, a key sticking point was not resolved during the hearing and it will be very interesting to see what is proposed in the revised care and support plan.
One final point needed to be confirmed: Oliver Lewis asked HHJ Owens to confirm whether she was authorising the deprivation of liberty. HHJ Owens replied that, as she had alluded to, yes she was, there was a significant interference with Sarah’s right to liberty. Whether that would alter with a new care and support plan, there was still the issue of surveillance by technology, so it probably still would be. She asked whether he was raising the issue due to funding, as if there was no DOL, it alters funding.
Oliver Lewis replied that there was no funding issue, as this was not a deprivation of liberty in a care home (which would be covered by the DoLS regime in Schedule A1 of the MCA, for which P is granted non means tested legal aid), but a community deprivation of liberty in a supported living placement (for which legal aid is available on a means tested basis) and means-tested legal aid was in place. After some final technical discussions, the hearing concluded.
Final Reflections
The whole exchange about the proposed use of technology to enable Sarah to have more freedom to go into the community alone really made me think. As Oliver Lewis stated, many parents have become used to using smart phones to track where their children are. I also know families who use it to track where other family members are, even to the extent of knowing when to have dinner ready for. Or single friends using it to ensure that somebody has arrived home safely. Or family members living with dementia using “airtags” so that their families can see if they have started “wandering”. I have also read of smart phones sadly being used to enforce coercive control. It seems as though tracking has become somewhat normalised in today’s world, for better or for worse. I wonder, how does this fit in with the law, especially with regards to the concept of Deprivation of Liberty? And the concept of “freedom”?
I also discovered something new about DOL. I had thought that it was restricted to hospital and care home settings, which can lead to s.21A appeals, as had happened in my mother’s case. But deprivation of liberty in the community was something I hadn’t heard of.
I am very interested in finding out what steps will be put in place to help keep Sarah safe whilst giving her as much freedom as possible – and whether the injunction served on Mr Grey achieves its objectives.
Anna was the pseudonym of a woman whose mother was a P in a Court of Protection s.21A application. Since March 2025, Amanda Hill is allowed to reveal that she is Anna, because the Transparency Order covering her Mum’s case has been varied (changed). Amanda Hill is a PhD student at the School of Journalism, Media and Culture at Cardiff University. Her research focuses on the Court of Protection, exploring family experiences, media representations and social media activism. She is a core team member of OJCOP. She is also a daughter of a P in a Court of Protection case and has been a Litigant in Person. She is on LinkedIn (here), and also on X as (@AmandaAPHill) and on Bluesky (@AmandaAPHill.bsky.social).
[1]I am also grateful to Celia Kitzinger for substantial feedback on earlier drafts and assistance in making sense of this case.
[3]I have learned that capacity for sex and capacity for contact are separate and are assessed separately. It’s quite often found that P has capacity for sex, but not capacity for contact and this poses problems