Celia Kitzinger, 16 May 2024
There are more than 500 centenarians in Devon, and she’s one of them.
Until September 2023, she lived at home with her daughter.
Now she’s deprived of her liberty in a care home, where she’s been for around six months, following discharge from hospital after a fall.
She wants to return home.
But now she’s been diagnosed with vascular dementia and assessed as lacking capacity to make decisions about where she lives and receives care, and who she has contact with.
There seem to be some question marks about the adequacy of the capacity assessments and that’s “in abeyance” pending receipt of care home records which will enable consideration of her presentation on a day-to-day basis.
The problem with a return home is that the applicant local authority, Devon County Council, has received safeguarding concerns – hoarding and clutter, and her daughter restricts access and is alleged to be “coercive and controlling”. The local authority is of the view that it’s in her best interests to remain at the care home. Her three sons agree. Of course, if she has capacity to make the decision for herself, then the court has no jurisdiction.
Meanwhile the court is looking into a possible return home – either because she may capacitously choose it, or because it may be the outcome of a best interests decision. They are investigating what a care package would look like. This is proving difficult because the daughter is declining to engage. The social worker (who was also in court) has tried to visit and “gain cooperation” but without success. It seems that the daughter believes she should be the sole carer for her mother.
The judge, DJ Eaton-Hart, sitting at Torquay & Newton Abbot County Court, expressed concern about the delay “especially with a lady of her age” but reluctantly accepted that another directions hearing would be needed before a final hearing, and has asked for the case to return before him on the first available date after 26th July 2024.
Transparency Issues
There’s been a history of listing problems with cases before DJ Eaton-Hart. They’ve been appearing in Courtel/CourtServe without any descriptors to indicate what the issues are before the court, and also without any contact information – which makes it very difficult for would-be observers to obtain links.
But I was pleased to see that on Wednesday 15th May 2024 it all looked correct – so I selected a case (COP 14203764) about “Where P should live and receive care” and “authorising a deprivation of liberty”. According to the list, the hearing would be a “directions hearing” , held via “Teams” and last for “ 1 hour”. And the Bristol hub email address was provided for contact. So far, so good.
I received an email with the Teams link, and with the Transparency Order as an attachment. This was continuing well.
But then, on downloading the Transparency Order (ten minutes before the hearing was due to start), I was dismayed to see that P’s name was spelled out in full on the face of the Order, and also appeared five times, in full, in the text of the Order itself. The Order also prevented reporting the identity of the local authority. The Order had been made by a different judge (DJ Smith) earlier this year.
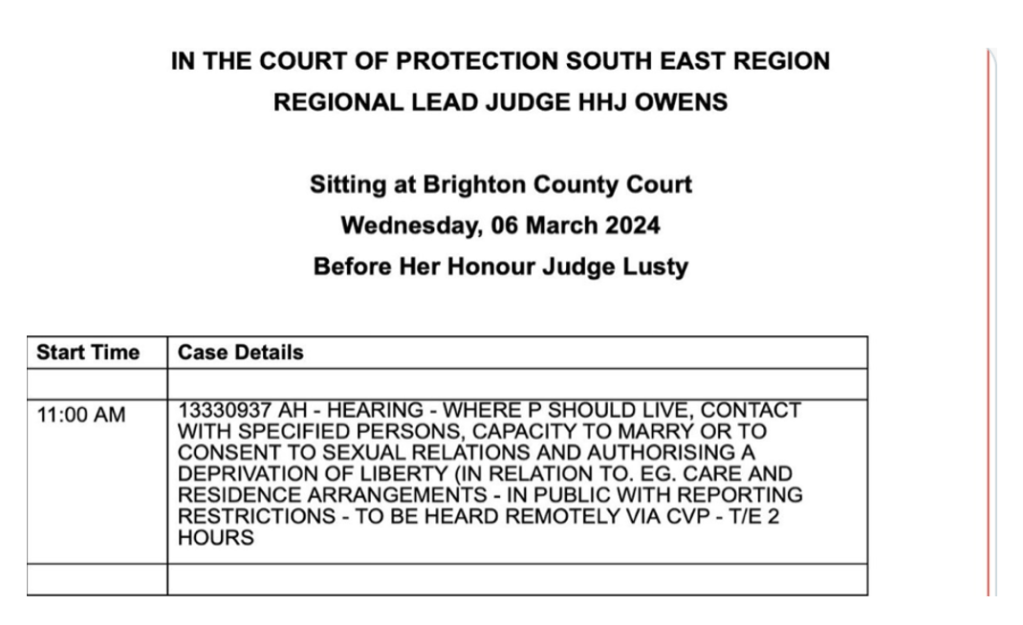
Here’s part of the offending Transparency Order. In every Transparency Order there’s a paragraph called “The subject matter of the Injunction” (usually, though not always, paragraph 6) which sets out the “Information” we are prevented from reporting. It’s the paragraph I always turn to first of all. In this case, as you can see below, it forbids us from publishing anything that identifies or is likely to identify the protected party (P) – the centenarian whose name is actually given in full (I’ve obscured it with those blue rectangles). It also prohibits (in 6(i)(c)) from saying anything that identifies or risks identifying the Local Authority – that’s Devon County County Council (not spelt out in full!).
I immediately emailed the court.
Please could you alert the judge to my concerns about this TO as follows:
1. P’s name should NOT be given in full on the TO – it’s both on the face of the TO and in the body of the TO.
2. It is not usual for the Local Authority to be covered by the information (see 6(i)(c)). In exceptional circumstances, where the judge has decided there is a risk that identifying a public body risks identifying P, a public body is sometimes anonymised – but only after anxious consideration of other ways of protecting Article 10 rights (e.g. restricting aspects of P’s identity from public reporting to minimise risks of jigsaw identification). Can the judge confirm that the Art8/Art10 balancing exercise has been carried out and other ways of protecting Article 10 rights considered?
The judge raised this with counsel at the beginning of the hearing: “Why does the Transparency Order name P? And why does the Transparency Order prohibit reporting of the identity of the local authority?”. Counsel asked for a pause to take instruction which was arranged for later in the hearing, after the substantive issues had been addressed.
After the 10-minute adjournment, both counsel and the judge agreed that the naming of P on the Order “shouldn’t have happened” – that it was “an oversight”. Counsel for P via the Official Solicitor said naming P on the Order was “obviously wrong” and that “the Order clearly shouldn’t have been sent out”. He asked what could be done to stop this from happening again. Also, Counsel for the local authority said they had “no issue with the local authority being named”.
The judge was clearly troubled that “something’s gone wrong with the Order” and wanted to “acknowledge my role and Judge Smith’s role in not spotting that earlier”. He said there were “learning points for those involved in drafting – and also I have to say, those approving – the Order. This is not the proudest moment of those involved in this case, I should think. Please file a new Transparency Order, and I’ll take steps to raise this with the COP hub”.
I was impressed with the way counsel and the judge handled the problems with the Transparency Order. They swiftly acknowledged that it wasn’t as it should be, and they fixed it there and then, without delay (albeit without, so far, having sent me a new TO). This speedy response contrasts favourably with several cases recently in which delay has been caused to reporting by observers being required to fill in and submit COP 9 forms, or write position statements: decisions about transparency orders very like this one have been postponed to future hearings, months ahead, even though nobody has made positive arguments for protecting the identity of a public body. It’s as if once the mistakes have been made, it’s painfully cumbersome to unpick them – and so unjustified prohibitions have remained in place for many months. This really concerns me. Open justice delayed is open justice denied.
Another impressive feature of this case was that the judge accepted judicial responsibility for the errors in the Transparency Order (even though it was a different judge who had made the Order). He referred to those who had drafted the Order but acknowledged that it was a judge who had signed it. He was also clearly committed to making sure that it didn’t happen again.
My understanding, from discussions at Court of Protection User Group meetings, is that the applicant solicitor is the person who usually drafts the Transparency Order. Busy judges seem to be signing off on the Orders without checking them. Of course, judges should not be “rubber-stamping” Orders, but equally it would be helpful if legal practitioners drew up Transparency Orders correctly in the first place.
In a case earlier this year, another member of our core group, Daniel Clark, similarly wrote to the judge (DJ Geddes, Lead Judge for the North-East-East Court of Protection Regional Hub) about a problematic Transparency Order. She, too, responded robustly and swiftly:
“Before we go any further, I’m not sure whether the message was relayed [to Counsel] that there had been a request to vary the Transparency Order, quite rightly because it’s wrong, or at least appears to be wrong, in that it includes…a prohibition on revealing information that Wakefield is a party to these proceedings, which shouldn’t have been included ordinarily. Does anybody object to me varying [that section] to that draft order? [nobody objected] Okay…I put out a plea to practitioners again – just stop doing it. It’s always difficult for it to be picked up when gatekeeping draft orders and the more that are right, the less time we have to spend on them when there’s much more important things to be thinking about including the actual facts of this case.” (Judge approves P’s conveyance (against his wishes) to a care home – and tells lawyers to “just stop!” routinely anonymising public bodies in draft Transparency Orders)
We are finding that a significant minority of Transparency Orders prohibit identification of public bodies (local authorities, integrated care boards, health boards, NHS trusts – and even the Office of the Public Guardian) for no apparent reason. When we point this out, lawyers and judges seem genuinely surprised to find the extent to which their Orders have restricted open justice and rarely seek to justify them. Almost always the prohibitions are simply removed – but sometimes not for days, weeks or even months after the hearing.
And it does worry me that the task of ensuring the appropriateness of the Transparency Order seems to be falling squarely upon members of the public – not all of whom have the knowledge and/or confidence to challenge these prohibitions in court.
Best of all, of course, is when Transparency Orders are appropriately drawn up and there is no need to challenge them. But when they’re not, we really appreciate those judges, and advocates, who’ve read the Order in advance of the hearing, understand what it says, have identified the problems, and address them proactively in public court. It’s immensely reassuring to see lawyers and judges engaging with the open justice implications of Transparency Orders – and thereby pre-empting our challenges.
Victoria Butler Cole KC set a good example recently when sitting as a Deputy High Court Judge at the Royal Courts of Justice (COP 14002430). Right at the outset of the hearing, after establishing who was in court, she made sure everyone was aware that the TO prohibited reporting that risked identifying P and P’s family, where they live or are cared for and their contact details. “But,” she said, “it also says that the Local Authority cannot be identified”. Parishil Patel KC, the barrister representing both Leicester City Council and Leicester and Rutland Integrated Care immediately responded by saying, “We will amend that and will not be seeking anonymity for the public bodies”. Perfect1. The judge and the lawyers took responsibility for ensuring open justice and I didn’t have to intervene. More like this please!
Celia Kitzinger is co-director of the Open Justice Court of Protection Project. She has observed more than 500 hearings since May 2020 and written more than 100 blog posts. She is on LinkedIn (here), and tweets @KitzingerCelia
- Well, not quite perfect. It would have been even better if anyone had actually sent me the Transparency Order, but I’ve no record of ever having received it – either the original version forbidding mention of the local authority, or any subsequent version. The judgment, however, has been published here: Re HC [2024] EWCOP 24 (and it does name the public bodies).