By Amanda Hill, 17 May 2024
“Open justice is a fundamental principle in our courts”.
That is the standard line included in many of the court listings. This means that members of the public, like me, can observe hearings. Sometimes, obstacles are put in our way. In this hearing, certain members of the public were excluded from the hearing despite being admitted. This time it was for a good reason though and I will explain what happened and how to avoid it happening in future.
I would also like to focus on two particular elements of the substantive matters in this hearing –an ageing mum whose ability to care for her son is being questioned, and record keeping by professionals.
Background to the hearing[1]
The protected party in this case (COP 13337913) is S, a man in his late twenties who has autism spectrum disorder and global learning disability, and can display challenging behaviours. He has lived for a number of years in a supported living placement.
The applicant is the London Borough of Islington, with S as first respondent and his mother (M) as second respondent.
S’s mother lives over 2 hours away from S but – according to the position statement sent to me by her legal representative, Rosie Scott, M provides not only a lot of practical support to S but also a great deal of emotional support. She’s been very concerned about the placement for a long time and believes it to be unsuitable for him for various reasons, not least that she believes S is very unhappy there. One of the options that the court was being asked to consider in this case was whether M’s home is suitable for P – in other words, could S move back home.
Open justice – cock up not conspiracy
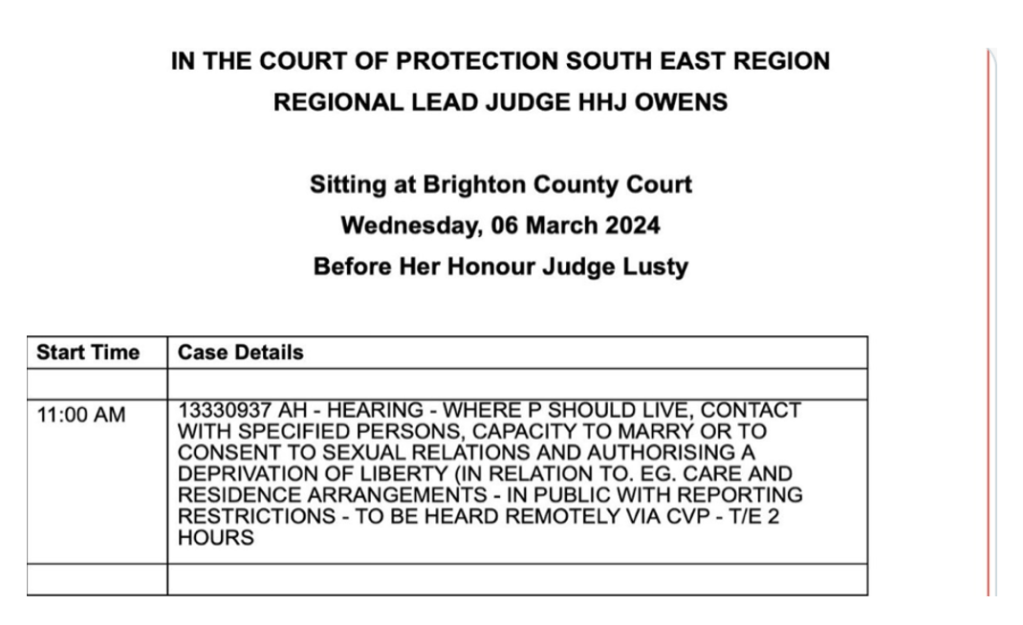
The case was listed as follows:
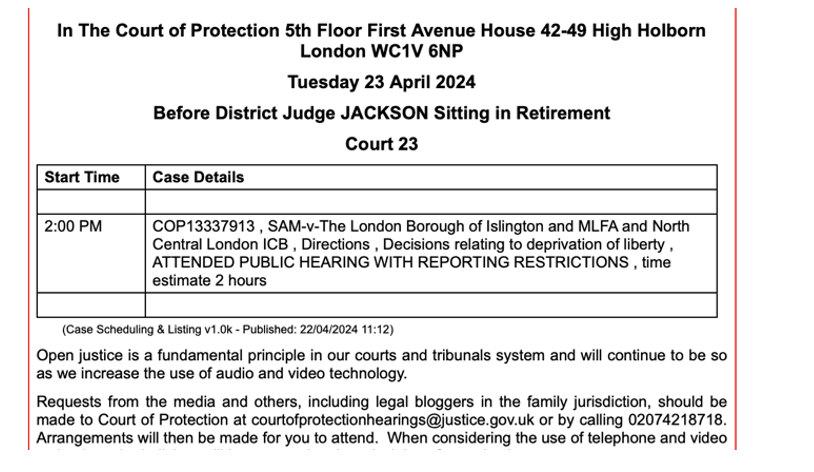
I think that District Judge Jackson was sitting in retirement in order to ensure judicial continuity in this case. Although the listing didn’t indicate that a link was available, I emailed the court to ask if I could observe remotely[2] (which I later realized the mother did too).
I did not get a reply to my initial email, so I phoned the court just over an hour before the hearing was due to start at 2pm and a little over 10 minutes later I received an email with the MS Teams link asking me to join 5 to 10 minutes before the start time. I also received a copy of the Transparency Order. So far, relatively straightforward.
I clicked on the link a few minutes before the hearing and as is usual was placed in the “waiting room”. After a few minutes I was allowed in and I could see an empty courtroom. I was surprised to find that the court clerk wanted to check who I was and if I was at the right hearing. I confirmed the case number and she seemed happy. In the event there was a 30-minute delay to the hearing starting because the parties had asked for more time.
The problem was that there were a lot of other people in the waiting room during this wait and the clerk did not know who they all were. As I had been admitted, I could observe the chaotic goings on behind the scenes before the hearing started. The legal teams eventually entered the physical court room and the clerk was trying to ascertain who was who in the waiting room in order to admit them to the hearing. The clerk explained to those in the physical courtroom that I was the only observer who had received the transparency order but that there were other people in the waiting room who wanted to observe. Some people were authorized to attend as people impacted by the case, such as M and somebody else from the local authority. M logged on and then lost connection.
The court rose at 14.35 but then the judge left 3 minutes later to wait for M to reconnect.
At this point there were a lot of chaotic connection problems. Somebody was admitted, who turned out to be the mother of a different “P” from another hearing I blogged about here. She was asked by the court who she was and she replied that she was from the Stolen Lives campaign. She had requested the link but not received it. She was then told that she could not observe because, essentially, she had not received an official link. So, she was ejected from the hearing. Another person joined by Teams but then by telephone due to connection problems. It seems that they were a supporter of M. At one point there was a discussion between the remote LA representative and this person, trying to find out what was happening. A member of the legal team had to intervene to remind them that this was still a courtroom and they should not be speaking. I think this experience shows the difficulty of remote hearings using MS Teams. Some of the formality is removed. However, it can also be intimidating – I stayed a silent observer with my camera off throughout all this.
Other people who I had seen waiting before the hearing started had disappeared and were not re-admitted at all.
I gathered afterwards that the problem was that the link for the hearing had been sent to one person and then sent on by them unofficially to other people who wanted to support M, when they did not receive it directly from the court.
As stated on the Open Justice Court of Protection Project website, “If you haven’t received the link in a timely manner, re-send it with URGENT in the subject and forward it to us (openjustice@yahoo.com). We can’t share the links but we might be able to help.”
Unless a judge specifically allows it, links cannot be shared with other people. Whilst this can seem frustrating to those who want to observe, it is so the court knows who is observing, has email addresses for them, and can ensure that they have received the Transparency Order (at least in principle – in reality the track record of the court sending out Transparency Orders is rather patchy).
What probably felt like the court obstructing open justice in this case was simply that the official process had not been followed.
That said, I think that there is scope for making the official process more efficient. It can be hard for court staff to manage (I could tell the clerk in this case was doing her best to do things correctly) and it can also be frustrating for would-be observers. I assume that in this case the link was shared because those wanting to observe had not received the link when requested. And I had needed to telephone the court staff to receive it. That takes up court staff time too.
So I think all this was cock up rather than conspiracy but it does not help the reputation of the court in terms of its commitment to open justice.
The hearing finally started properly at 3pm.
“None of us are getting any younger”
M wants her son to move back home with her and her other son.
Counsel for the local authority, Lee Parkhill, set out at the start of the hearing that steps were being taken to consider that, as well as alternative placements in care homes that would be closer to the mother’s home.[3]
When this was discussed during the hearing, the judge stated that she had asked “some time ago” for an assessment of the viability of M caring for her son at her home. She continued by saying that it had been a long time since M had cared for him (in 2013), and he had gone from a teenager to a grown man and “none of us are getting any younger”. The judge wanted to know if M would still be able to care for him, to see how able she is as a carer as she is “not getting any younger”. She wanted to see something of this nature, to “find out more about that”.
Rosie Scott pointed out that there would be a care package in place and that M would not be caring for him on her own. The judge went on to say that she would like that aspect to be dealt with to avoid expensive renovations (which it had been outlined would have to be made to M’s house to allow S to return home). The judge asked how M handles S’s behaviour, that she would like to know more about that “as it’s important”, that it might show a way forward. The judge asked for more information about M’s role currently and what she would want to do. There was talk of a “trial” of M doing more for S and by mid-July an assessment of how it had gone with the mother’s interventions and S’s reactions to them. A carer’s assessment of M as a carer was also needed.
It should be said that the judge wanted to ask M about this but it had been explained at the start of the hearing that although she was attending remotely, she was ill with laryngitis and could not speak. She had in fact appeared on camera at the start of the hearing at the judge’s request, and she was lying down in bed. This was unfortunate given the judge’s focus on her physical ability to care for her son.
The judge’s concern also led me to reflect on the many unpaid carers looking after loved ones who are just quietly getting on with it without any input from the court. And the wheels of justice can move very slowly. This felt to me an additional pressure on M – I would hate to be questioned as to whether my own age and health could prevent me caring for a loved one, especially as a team of carers would be in place. Many protected parties in the COP want to go home and are indeed allowed to, with a team of appropriate carers in place.
Record keeping
There were question marks about the record keeping at S’s placement and the need for accurate record keeping was in the draft order. Asma Niazi, counsel for the OS and S’s litigation friend, addressed the gaps in record keeping that had been identified. For example, M says that S asks to go home with her each time she visits but the records don’t record that. M wants access to the records. The judge came back to this issue later. She said that it never ceased to amaze her that “professionals don’t record things properly”. She stressed the importance of recording things properly and there was a discussion about methods of communication. The judge asked “Why can’t they (the placement) just provide a detailed account?”. This exchange made me reflect on how important record keeping and access to records are, the duties of professionals and also a parent wanting to know exactly what was being written about their son.
A further hearing in this case was scheduled for 22nd August 2024.
Amanda Hill is a PhD student at the School of Journalism, Media and Culture at Cardiff University. Her research focuses on the Court of Protection, exploring family experiences, media representations and social media activism. She is on X as @AmandaAPHill
[1] Rosie Scott, Counsel for the second respondent, kindly sent me her position statement, which greatly helped my understanding of this case. I also asked for the other two position statements but did not receive them.
[2] The Remote Observation and Recording (Courts and Tribunals) Regulations 2022 (in Practice Direction on Remote Observation of Hearings, June 2022) empowers judges to “allow remote observation of in-person and hybrid hearings” as well as remote ones (§3).
[3] It is forbidden to record any part of a hearing and I don’t touch type so my notes will not be 100% accurate.