Back in October 2025, the Open Justice Court of Protection Project hosted an open WhatsApp forum as a basis for live discussion of the hearing, over three days, of the case brought by the Attorney General of Northern Ireland, asking the Court to reconsider Cheshire West. More than 150 members of the public joined the group and discussed the hearing (see “When open justice undermines public confidence”) and raised a lot of questions about the work of the Supreme Court and the way it operates. My challenge, after that, was to find a retired Supreme Court judge willing to answer them.
It was a privilege and a pleasure to have the opportunity to talk with former Supreme Court judge, Lord Jonathan Sumption, for an hour over video-link on Friday 28th November 2025.
Lord Sumption was a Justice of the Supreme Court between January 2012 and December 2018, when he retired on reaching the (then) mandatory retirement age of 70. His legal expertise is in Commercial, EU and Competition, Public and Constitutional Law. He has also published extensively about the relationship between politics and the judiciary (e.g. Trials of the State: Law and the Decline of Politics (2019) and Law in a Time of Crisis (2021)) and is an accomplished historian.
****
CK: The reason people are particularly interested in the Supreme Court right now is because of the recent case reconsidering Cheshire West.
JS: I have not reminded myself of the details of that case. I know that it’s a widely held view that it was wrongly decided. The leading judgment however, was given by Lady Hale, who is a considerable authority in the field.
CK: And a feature of the current case before the Supreme Court is that none of the seven justices who heard the case were expert in this field. So, it came as a shock to observers to hear the very basic questions they were asking and some of the language they were using, and the ignorance they displayed about some key aspects of the Deprivation of Liberty Safeguards and the Mental Capacity Act in practice.
JS: I think it’s right that there are no Family judges currently on the Supreme Court. Which is not an unusual state of affairs because Family cases don’t often get there. When Brenda Hale was President of the Court a much larger number of Family cases ended up in the Supreme Court than was the case before, or after. If I can make one general comment at the outset: the function of the Supreme Court is to get the law right and to deal with general questions of principle. On the whole the Supreme Court, rightly in my view, does not like the idea of islands of law governed by principles that are peculiar to that area of law. It seeks to relate specialised areas of law to general principles – and that has been a strong feature of recent case law in family law. So the fact that specialists in this area are surprised, even dismayed, by what goes on when a case involving their field is being heard, shouldn’t actually be that surprising.
CK: Thank you. That’s helpful.
1. Job description
CK: If I can turn to the first set of questions – they are effectively about your job description. We can see what goes on when you’re sitting, but what are you doing the rest of the time? We even wondered about what happens in the lunch break – do you all sit together and talk about the case?
JS: In the lunch break, we do eat together but on the whole we talk about anything other than the case in hand. Frankly one needs a bit of a rest from the case you’ve just spent two-and-a-half or three hours hearing. More generally, the system is this –unless it’s changed since I retired. We receive papers a few days in advance. They will consist of the judgments of the courts below the written arguments of the parties and interveners, and the essential documents. We read those, and we meet about a quarter of an hour before the hearing[1]and exchange preliminary views. That exercise is deliberately kept short because we don’t want to find that people dig themselves into their first impressions about the case before they’ve heard the arguments. We then go in and listen to counsel. It is the job of counsel to acquaint us with any special features of their particular area, bearing in mind that – at the most – there may be no more than one or two of the panel who are specialists in the relevant area. When we’ve finished the hearing, we retire and have a much more detailed session in which each member of the panel will deliver what really amounts to a mini-judgment of, say, five minutes, starting from the most junior and working up to the most senior. At the end of that, we will have an idea of where the majority view lies – or possibly where the unanimous view lies. Somebody will be appointed to write the principal judgment. The view expressed at this meeting is not always writ in stone. People do sometimes change their minds. Actually sitting down to write a judgment is a very exacting discipline, and if there’s something wrong with your reasoning in your mini-judgment, it is the time when you’re likely to discover any logical fallacies in one’s existing view. Sometimes the majority view may change. Although there is always a lead judgment, anybody is entitled to give a judgment. The next stage is when the panel has produced its draft judgments. In the old days, the practice was simply that each judge wrote their own judgment, handed it down like tablets from the mountain, and that was that – you just counted up votes, and that gave you the answer. It’s a much more consultative process now. We look at each others’ drafts, we may criticise them, we may point out things that we think don’t stack up, and sometimes that will result in the judgments being modified. But the worst sin that a judge in the final court of appeal can commit is to leave the law unclear. There is a process of – you can loosely call it – negotiation, in which people who are writing a judgment may take on board points made by others so as to achieve the greatest possible degree of consensus.
CK: Yes, I looked at some of the judgments you’d been involved in and the Nicklinson one struck me because I think every judge wrote a judgment in that case.
JS: That’s true. Some of them wrote very short judgments that were essentially agreements with somebody else, adding a grace note of their own.
CK: And you were picked up for your judgment by academic John Coggan[2] for the moral arguments you introduced in the Nicklinson judgment, which is not your usual stance on how the law should be developed.
JS: They’re not anybody’s usual stance. As I pointed out in the opening paragraph of my judgment in Nicklinson[3], judges try to steer clear of general moral pronouncements, because that tends to get in the way of other cases. Perhaps the second worst sin that a judge in the final court of appeal can commit is accidentally to decide half a dozen other cases that aren’t before him.
CK: What are the pressures on judges to reach a consensus in order to keep the law clear – and can you say a bit more about concurring and dissenting judgments?
JS: You concur with or dissent from the ultimate conclusion, and sometimes it happens that the majority consists of people who agree on the outcome but disagree on the reasons. That’s a very unsatisfactory state of affairs, because it means that although you’ve got a clear answer to the case in hand, we are not giving clear guidance as to what the law is, so that the lower courts can apply it in subsequent cases. We go to quite a lot of trouble to avoid that situation. There have been notorious cases when there was a majority for a particular conclusion, but a majority against every possible reason for reaching that conclusion. That is a very sorry state of affairs. I can remember a case on which I sat in which there were two competing camps, each with two people – plus me. And I had a different reason for taking the view I did from any of my colleagues. That, I thought, would have been a disaster. Seeing that I was in a minority of one, I therefore agreed with one of the other groups, so there would be a clear answer. Now there are those who would say that’s an intellectually dishonest process. But what would be the point, other than indulging one’s personal vanity, in giving a judgment with which nobody agreed. Sometimes you have decide which of two alternative views you disagree with least strongly – because the object is to ensure that the law is clear.
2. Expertise
CK: As a Supreme Court judge you have been involved in making judgments that are absolutely central to your areas of knowledge and expertise, obviously, but equally in others (like Cheshire West) that were not. What is the difference for you as a judge in those two different kinds of contexts?
JS: I was not an expert in mental health issues, but I was extremely familiar with human rights law including the right to liberty. As I have said, we try to relate our conclusion about a particular case to general principles of law, and there is a mass of relevant case law on deprivation of liberty much of which has nothing to do with mental health. If you have no personal experience of the particular area of law that you are dealing with, you have to work harder to get on top of it. But I think that most judges would defend a system in which the panel does not consist entirely of specialists in that area and may not have any specialist in that area. Sometimes when you go into an unfamiliar area of law and read the judgments of the courts below, you say to yourself “Blimey! What’s been going on here?” Specialisms are important and valuable, but specialist practitioners and judges sometimes lose the habit of looking over the garden wall at what’s happening next door. That can mean you get little islands of law governed by completely different principles to the whole of the rest of the law.
CK: So what is the expertise that you bring when you’re not an expert in that particular area of law? What is the knowledge and skill-set you bring that is not subject-specific?
JS: Well, we have a general grasp of the principles upon which the common law works. The common law, which is essentially a system of customary law, is an accumulating body of instincts[4] which have influenced judges over the years. It has certain consistent ways of thinking about problems even if they arise in unfamiliar contexts. A judge who is not a specialist in that area will very often come into a case and find that the principles on which this particular specialism has worked for many years either don’t stack up or are inconsistent with principles that the common law regards as important. To give you one example. One of the very first cases with which I was involved was a case about financial provision in a divorce. For some years, the Family Division had treated companies as being completely transparent. They ignored the general law about companies which treated them as separate legal persons, and they treated the assets of the husband’s company as if they were his (it usually was the husband, but the principle would be the same if it was the wife’s). That may have seemed to many Family judges a just thing to do. But you can’t have a system in which the Chancery Division, which deals with companies, treats them in one way and the Family Division treats them in another.
3. Subpanels
CK: How are the 5 or 7 or however many judges on a panel selected – or do they self-select? – for a particular case. Who chooses who hears a case?
JS: In the first place, the Registrar[5] does. A Registrar is usually an extremely experienced judicial administrator who will know who the specialists are in a particular area, will try to produce a balanced panel. He or she will also try to share out the work equitably between the 12 justices. The initial selection will then go to the President and Vice President of the Court – who may just agree with it or may suggest changes. One thing that doesn’t happen – at any rate in my time – justices were not supposed to lobby for inclusion in a particular panel. And they didn’t, in my experience, either.
CK: Would it be helpful to have more than 12 justices?
JS: Twelve is enough. If the object of increasing the number of justices were to be to ensure more specialists on each panel, I think that would be a bad idea – for the reason I’ve already given. I think that you need a specialist, possibly two, but having a majority of specialists tends to undermine the purpose for which the Supreme Court exists. The workload is manageable with twelve. In my time, the Supreme Court tended to hear about 80 cases a year so each justice would probably hear about 40 cases, on average, in the Supreme Court. Then there were also the Privy Council cases. Remember that we also have to take time to write judgments.
CK: In terms of writing judgments, that must take a lot of time.
JS: Yes, it does.
CK: And at the hearings I’ve watched, the quality of the submissions has varied and I imagine some are more helpful than others. So when the level of knowledge assumed is set at too high a level for the non-specialists or when a submission is simply incoherent (which, in my view, some have been), it must then be much more of a struggle for judges to write a judgment. Because you’ll presumably have to do some background research of your own?
JS: Well, we tend to do background research anyway. But obviously the amount of background research that needs to be done is very much affected by the quality of the submissions that we receive. On the whole, and this is a very broad generalisation, the quality of advocacy in the Supreme Court is high. It is the most prestigious court. Barristers like to appear before it. And clients are prepared to pay for quality once they’ve got to that level of the judicial hierarchy. We do get cases where the advocacy is very poor, but not often.
CK: How do you manage that?
JS: We simply have to do more work ourselves.
CK: So during hearings, I’ve seen judges constantly interrupting advocates and asking for clarification and explanation.
JS: Making a submission is not the same thing as giving a lecture. It’s more like a seminar. It’s a very interactive process. The most productive part of a hearing is often interrogating a barrister about his or her view – “what do you say about this?”, “how do you reconcile what you said an hour ago with what you said 10 minutes ago?”, and so on. This isn’t designed to wrong-foot the barrister or make a fool of him. It’s designed to ensure, first, that we’ve correctly understood his submissions, and secondly that he has an opportunity to address things that may be causing us concern. When a barrister reads the judgment after the case is over, he shouldn’t find himself (or herself) saying, “I wish that I’d known that they were thinking along those lines: I could have put them right!”. That’s a very frustrating thing for an advocate and it’s also a bad thing for the administration of justice. The point on which we didn’t give him an opportunity to put us right may turn out to have been rather a good one.
4. Evidence and arguments
CK: Obviously you have a huge bundle of submissions and evidence and case law in front of you – but do you go outside of that after the hearing, and before handing down a judgment? What’s involved in doing your own background research? Would you google things? Would you talk to colleagues across a different area of law?
JS: You might sometimes talk to other colleagues on the Court itself. You wouldn’t normally discuss it with people outside the Court. You’ve got to be careful about discussing a case with people who are not involved because it’s you who’s actually heard the arguments and read the bundles. But sometimes it is helpful to discuss an issue with a colleague with specialist knowledge. I can remember an English rating case, in which it turned out that quite a lot of the cases were Scottish We were rather impressed with the Scottish cases. But we didn’t have a Scot on our panel, so it seemed sensible to discuss with our Scottish colleagues – there are always two members on the Court – what the basic principles were behind these cases and whether they were based on a completely different set of legal principles to the ones that would apply in England. That’s one example of the kind of thing that happens. In terms of seeking out additional information, that’s sometimes necessary when you’re writing the judgment. When considering an authority cited to you, it is often helpful to know what earlier case-law it was based on and what has been said about it in subsequent cases. The Supreme Court’s task is to keep the law up to date and to keep it coherent. So you very often need to know how the law has come to be as it is. That will quite often involve looking at the earlier legal history. I will add this though: sometimes the legal research will present the case in an entirely new light – in a way that counsel had not anticipated in their submissions. If you are inclined to decide the case on a basis that has not been the subject of submissions by counsel, you should usually give counsel notice of this and either invite written observations or re-list the case for a further hearing. It doesn’t happen that often, because counsel normally get the agenda right – but when it does, you have to counsel the opportunity to address you on the new turn that the argument has taken in private.
5. Interveners
CK: How are decisions made, and by whom, about who gets to intervene, and on what basis are those decisions made?
JS: The decisions are normally made by the Petitions Committee that decides whether to grant leave to appeal or else by the presiding judge of the panel assigned to hear the case.
CK: What is the Petitions Committee?
JS: To appeal to the Supreme Court, you need permission, either from the Court of Appeal or from the Supreme Court itself. Applications to the Supreme Court for permission to appeal come before a petitions committee of three judges. This work is distributed around all 12 justices of the Court. So three judges will be given a pile of applications for leave to appeal and in the next door room three other judges may be looking at a different pile of applications.
CK: And will the judges on the Petitions Committee also be those who hear it if permission to appeal is granted?
JS: Not necessarily.
CK: And on what basis is the decision made about-
JS: The test is not whether we think the judgment of the Court of Appeal was right. That’s one factor. The most important factor is whether this an issue which ought to be decided by the Supreme Court so as to provide a higher level of authority for the decision. The test is whether the case raises a question of legal importance for the law generally. We sometimes refuse leave to appeal, although we think the Court of Appeal got it wrong, simply because it doesn’t actually matter to the general development of the law.
CK: And in terms of applications to intervene?
JS: Interveners need permission to participate. The practice changes from time to time. When I was on the court, there were a lot of interventions. Sometimes they were allowed to address the court through their advocate, and sometimes they were required to present their points in writing. I believe that in the last few years the Court has become more restrictive about interventions. Interveners are normally NGOs or single-issue pressure groups which have some claim to special knowledge or experience of the field. Sometimes the effect of the intervention can be dramatic. For example in the Rwanda case[6], the United Nations Commissioner for Refugees applied to intervene and his legal team basically took over the case when it came to the hearing. That’s unusual – but it’s what happened in that case, because the United Nations Commissioner for Refugees has a great deal of knowledge of this problem on a world-wide basis and was therefore in a position to assist with both evidence and with submissions on the law.
CK: In the Attorney General for Northern Ireland Reference case the Secretary of State was an intervener.
JS: It’s quite common for the Secretary of State to intervene. If an appeal raises issues which significantly affect the public administration, the Secretary of State may have a point of view which ought to be heard. The Secretary of State isn’t entitled as of right to intervene. He’s got to apply for leave to intervene like anybody else – but it is more likely that the Secretary of State will be allowed to intervene than any other applicant, because the State – particularly in public law cases – will normally have a genuine interest. But there are cases where the Secretary of State has been told “no – it’s nothing to do with you”. There was a case not long ago involving hire purchase commissions where the Secretary of State wished to intervene because he thought it would be extremely expensive for the HP companies and their insurers if the decision of the Court of Appeal was upheld. Well, the court is not normally concerned considerations like that. In that case – I wasn’t on the Court at that time, it was after my retirement – the Secretary of State was sent packing.
CK: There was some concern in this case, and also in another recent case – the For Women Scotland Equality Act case – about particular pressure groups that were not allowed to intervene, and they felt they had been excluded from the justice process and that their voices were not heard.
JS: Their concerns are misplaced, in my view. The thing about interventions is that they are designed to allow the court to hear from a party that either has a particular expertise, or has a point of view which will not necessarily be represented by the parties to the appeal. That’s the basis on which people are allowed to intervene. The problem about interventions is that they can give the impression that the hearing is actually a political debate. Most interveners are single-issue pressure groups or NGOs which are basically political lobbyists. The Court is not there to debate the politics of the thing or to give everyone who’s got a bee in their bonnet the opportunity to let it out. So when I was on the Court we probably gave leave to intervene too often, and I think I’m right in saying that it’s become more restrictive subsequently. I think that’s a good thing. Many people have strong views about a particular issue. It doesn’t follow that they should be entitled to intervene into somebody else’s litigation in order to express them. Nine times out of ten, their strong views will be reflected in the submissions of the principal parties. There’s absolutely no point in allowing people to intervene simply for the purpose of duplicating or adding volume to someone else’s submissions.
6. Reference
CK: The case brought by the Attorney General of Northern Ireland was different from other cases I’ve watched before in the Supreme Court which have worked their way up through the Court of Protection and then to the Court of Appeal. It came as a Reference from Northern Ireland and there was no particular person at the centre of the case, and it was a pre-emptive application in the sense that the applicant wanted to know whether enacting the law in a particular way would be lawful – compliant with the European Convention on Human Rights. That’s a very different use of the Supreme Court from the way I’ve seen it used before. Can you say a bit about applications like this.
JS: The Court doesn’t have very many cases like that, but they’re liable to happen in cases which arise from the devolved jurisdictions. The legislatures of Northern Ireland, Scotland and Wales do not have the same plenitude of power that the UK Parliament at Westminster has. Their powers are limited in certain ways – in particular, they are not entitled to enact things that would be contrary to the Human Rights Convention. So there is a procedure, which is most commonly used in the case of Scotland, where before an item of devolved legislation receives the Royal Assent the power to make it is considered by the Supreme Court on a reference by the relevant law officer. You’re right that, normally, the courts are not there to give legal advice. They’re there to decide cases that have actually happened. But cases about the powers of the devolved legislatures are different, because if the devolved legislatures are going to legislate in a way that they have no power to do, that would produce chaos. It is much more sensible that what they are intending to do should be considered in advance by the Court.
CK: So is it a different process for you from considering “did the Court of Appeal get it wrong?” to instead be asking pre-emptively “is this proposed legislation going to be wrong”?
JS: The question is inevitably more abstract. So it’s only appropriate to do that if the issue is sufficiently crisp – for example if there’s a ‘yes’ or ‘no’ answer to it. You don’t want to be doing that if the answer is “it all depends”.
7. Overriding a previous Supreme Court decision
CK: Effectively, the Attorney General of Northern Ireland is saying that Cheshire West got it wrong.
JS: Yes. And if there’s a decision of the Supreme Court that is arguably wrong, the sooner we decide whether it is, the better.
CK: So I have learnt that this means invoking the 1966 Practice Direction which means that the Supreme Court can decide that it got a previous decision wrong. But there aren’t many of these cases and-
JS: That’s because the Court normally gets it right.
CK: I wonder what the process is for getting it right this time. One of the judges hearing the Attorney General of Northern Ireland Reference was also a judge, alongside you, in Cheshire West, that’s Hodge, and he wrote a dissenting judgment. So he is now effectively in the position of re-hearing Cheshire West with the opportunity to make the same judgment (then dissenting) that he made 14 years ago.
JS: He’s got to carry three colleagues with him. He’s not deciding it on his own.
CK: True. But how does the Supreme Court go about deciding that the Supreme Court itself got it wrong?
JS: The same way that it decides any other issue. There is no such thing as an infallible institution. Sometimes we might say, “well, this isn’t the way we’d decide it nowadays, but there are good reasons for leaving the law as it stands, and allowing Parliament to change it”. Sometimes the Court decides that, actually, we cocked up. That happens! Cheshire West is a controversial case. It’s perhaps once every five years maybe that the Court overturns a previous decision of its own. That may be because they think they just got it wrong first time round. It may be because they think that the circumstances have changed. It may be because they think that in cognate areas the law has changed – for example, new statutes.
CK: One of the issues raised by Cheshire West is the cost of that decision. It’s very expensive for the public bodies. You said earlier that the Court isn’t interested in the question of whether it’s expensive to comply with the law.
JS: It may be relevant in public law cases because traditionally the courts do not make decisions that require tax-payers to shell out. Taxation and expenditure are very much matters for Parliament. It is also obviously right that every item of public expenditure has an opportunity cost, so what the government spends on X cannot be spent on Y or Z. That’s one reason for the sensitivity of the courts in cases that have significant implications for public expenditure. When I said that the courts were not interested in the costs of things, I was thinking of private law. The Court will not normally be impressed by an argument which says, “if you decide in favour of the claimants, then an awful lot of insurers are going to go bust”. But it might sometimes be impressed by an argument which says “this has huge implications for public expenditure – and for taxation”. Because that’s a public issue.
8. Open justice
CK: We are an open justice organisation. We believe that members of the public – as well as journalists – should be able to go into public courtrooms and observe hearings and publish information about them. That’s exceptionally well organised by the Supreme Court because it’s live-streamed, the building and the courts are open to the public and it’s a welcoming space. But the proceedings are not always intelligible. So you can be sitting in the room, as I was, and listening to the arguments, and not understanding them. And even the information put up on the court website in advance of the hearing was barely intelligible. What do you think is the responsibility of the Supreme Court to promote better public understanding and transparency?
JS: The pre-hearing handouts ought to be intelligible and accurate. But some legal issues are highly technical. Advocates have limits to the time that they’re allowed to be on their feet. Requiring them to always explain things in language which is not necessary for the Court, but is necessary for the audience behind, is a luxury which – in a time-limited world – we can’t always afford. But the judgment should make it absolutely clear, and should also be written in language that is easy to understand. Moreover, when the judgment is announced, a summary is read by a member of the Court and that summary is exclusively directed to lay audiences. It will never, or certainly should never, be difficult to understand.
CK: Is there anything more you think the Supreme Court could do to be more transparent?
JS: I think it’s an extremely transparent court. I think it has avoided the obscurities which sometimes featured in judgments of the appellate committee of the House of Lords. It has opened up the hearings to an unlimited range of people with the live-streaming. I think that the practice that was invented when the Supreme Court took over from the Appellate Committee of the House of Lords, of reading out a simple summary of the facts and how the case was decided, is an admirable one. There is no such thing as a perfect institution in the world, but I think the Supreme Court comes closer to it than most.
Celia Kitzinger is co-director of the Open Justice Court of Protection Project and she is very grateful to Lord Sumption for accepting the invitation to be interviewed for this post.
[3]R on the application of Nicklinson and another [2014] UKSC 38 The first paragraph of Lord Sumption’s judgment reads as follows: “English judges tend to avoid addressing the moral foundations of law. It is not their function to lay down principles of morality, and the attempt leads to large generalisations which are commonly thought to be unhelpful. In some cases, however, it is unavoidable. This is one of them” (§207)
[4]“… The common law is not an uninhabited island on which judges are at liberty to plant whatever suits their personal tastes. It is a body of instincts and principles which, barring some radical change in the values of our society, is developed organically, building on what was there before. It has a greater inherent flexibility and capacity to develop independently of legislation than codified systems do. But there is a price to be paid for this advantage in terms of certainty and accessibility to those who are not professional lawyers. The equities of a particular case are important. But there are pragmatic limits to what law can achieve without becoming arbitrary, incoherent and unpredictable even to the best advised citizen, and without inviting unforeseen and undesirable collateral consequences. …” Sumption, in Mirza v Patel [2016] UKSC 42 at para. [226]
[7] R (on the application of AAA and others) (Respondents/Cross Appellants) v Secretary of State for the Home Department (Appellant/Cross Respondent) UKSC/2023/0093 plus BBC report of the case here: https://www.bbc.co.uk/news/uk-67423745
When someone lacks capacity to make a will, it’s possible to apply to the Court of Protection for a will to be made on their behalf. It will be made in their best interests under s.18(1)(i) of the Mental Capacity Act 2005. These are called “statutory wills”[1].
In 2022, I applied for a statutory will on behalf of my sister, Polly Kitzinger. It was a simple and uncontested case. The judge decided it on the papers, without a hearing – as I understand is the case with most statutory wills. That means no observers and no Transparency Order to tell everyone what they can and cannot report. The proceedings are essentially ‘private’, and section 12(1)(b) of the Administration of Justice Act 1960 applies – meaning we can’t publish anything about it. I can only write about Polly’s statutory will here because we applied, and were granted, permission of the court. How we did that will be the subject of another blog post.
Not all applications go as smoothly as Polly’s, and hearings do take place when there’s a dispute. They sometimes appear in the public listings and then they can be observed and reported. In the first part of this blog post, I report on a case listed as concerning “whether the court should authorise the execution of a statutory will”. An elderly woman with dementia was at the centre of a family conflict about who should inherit what. It was a complicated and painful situation, involving an estate valued at over £1 million, which included the family farm and it’s still not resolved as far as I know.
There’s a problem with publishing only information about statutory wills that result in hearings. By definition, these are the most challenging – often contested – cases. My aim here is to document some of the complexities in a disputed application (the case I watched concerning the family farm, COP 13947478) and also to demystify a routine case (my application for Polly, COP 11757133). As I’ll show, even a straightforward application that’s decided ‘on the papers’ has emotional complexities and administrative challenges – albeit not to the same degree as cases resulting in hearings.
Part 1 describes the contested hearing I observed.
Part 2 sets the hearing I observed in the context of my own experience of a much more straightforward application.
Part 3 reflects on the process of making a statutory will application and considers the costs and benefits of doing so.
I’ve not been able to find any published accounts from other family members about applying for a statutory will – probably due, in large part, to reporting restrictions which make only anonymised reports lawful. My account of the experience is potentially useful, in my view, partly because some family members (including lay deputies and people holding power of attorney) may never have considered the possibility of making this kind of application. Others may be aware of statutory wills, but hesitant to apply because they are daunted by the legal process involved, anxious about creating family divisions, or concerned about their own “conflict of interests”. Unlike professional deputies, a lay person who might apply for a statutory will may well be a potential beneficiary and/or in family relationships with others who might benefit from, or be ‘disinherited’ by, a statutory will. Making a statutory will application means having to live with any stigma or blame associated with the outcome.
I hope that this account of my own experience might both inspire others to think about the pros and cons of making a statutory will application, and also alert lawyers and judges to what statutory will applications can be like for lay people – and to consider whether the process can be improved.
Part 1 – A contested statutory will: “Mrs P”
The Open Justice COP Project has published only two previous blog posts about statutory will hearings: “An emergency statutory will for a dying man” and “Judge approves statutory will in contested hearing”. We were unable to observe another case, held in private, concerning a multi-millionaire with severe dementia (“Secret justice”). So, given my personal interest in statutory wills, I was pleased to be alerted to another hearing (COP 13947478) listed in Courtel/CourtServe to consider a statutory will application on 6th June 2025.
The protected party (Mrs P) is in her early eighties and she’s been diagnosed with vascular dementia. Until about three years ago, she lived at home with her (second) husband on the family farm. He died a few years ago, and she moved into a nursing home.
Mrs P has a daughter from her first marriage, and two stepsons from her second marriage. In 2019 she appointed one of her stepsons (“S”) as her attorney for both property and affairs and for health and welfare – and it was he who was making the application for the statutory will.
Counsel for the applicant, was Daniel Currie (St John’s Buildings); counsel for two of the respondents (Mrs P’s daughter and other stepson) was David Green (Atlantic Chambers). The protected party (Mrs P) was represented, via the Official Solicitor, by James Kirby (Lincoln’s Inn).
Mrs P’s last will was made in 2005. She and her husband made mirror wills, each appointing the other as executor and giving each other the entire estate. If the other did not survive, the wills gave the farm to S (Mrs P’s stepson) on condition that he live there and farm the land for five years. The residuary estate was to be divided equally between Mrs P’s daughter and her other stepson. When her husband died in 2022, this meant that Mrs P inherited the farm and all the couple’s savings and investments.
Shortly after her husband’s death, Mrs P attempted to make a new will. Her wishes at that point seemed to be that S should be her main beneficiary and should inherit the farm, but that her other stepson, and her daughter, should not benefit. She wanted her grandchildren (her daughter’s children) to benefit instead. She was not able to make a will to this effect because a capacity assessor found that she lacked “testamentary capacity” (the specific capacity needed to make a will[4].
Nobody disputes the finding that Mrs P now lacks capacity in this area of decision-making. Without a new statutory will, her previous will, made in 2005, is what will determine how her assets are distributed.
This was the situation that led Mrs P’s stepson, S, to apply to the court for a statutory will to be approved by a judge, on behalf of Mrs P – and he had drawn up a draft for consideration.
The statutory will drafted by Mrs P’s stepson gives the farm to him – as does the 2005 will – but unlike the 2005 will, the new draft proposed that neither Mrs P’s other stepson (his brother) nor Mrs P’s daughter would inherit from her estate. He proposed dividing the residuary estate 80% to him and 20% to Mrs P’s grandchildren. This bears some relation to what seem to be Mrs P’s most recently expressed (but non-capacitous) wishes though her alleged wishes are disputed by Mrs P’s daughter and the other stepson who are the second and third respondents in this case. Their view is that the previous (2005) will should stand, and that there is no need for the court to make a statutory will.
There’s another source of contention too. In his role as her attorney for property and affairs, S has spent more than £200k of Mrs P’s money renovating the farmhouse. He says the renovations were undertaken in her best interests to enable her to return home – which the local authority deems to be in her best interests. He also did much of the work on it himself, losing earning potential by so doing. It was confirmed in court that Mrs P is shortly to return home with live-in care. However, Mrs P’s daughter and other stepson dispute the extent to which the renovations were in Mrs P’s best interests and note that if S is to inherit the farm, he would personally benefit from this expenditure. Of course, the cost of renovations also reduces the value of the residuary estate (from which they were due to inherit under the 2005 will) – and it is also being reduced by Mrs P’s ongoing care fees (she’s self-funding). This will become even more of an issue going forward given that the cost of Mrs P’s care will increase when she returns home.
At the time of the hearing, the Official Solicitor (representing Mrs P) had organised a Court of Protection Visitor to meet with Mrs P and find out her current views. The OS had then put forward a proposal for a statutory will which was different from both the 2005 will and from the will proposed by S. The Official Solicitor’s proposal was for a will which did leave some money to Mrs P’s daughter and the other stepson (the one not inheriting the farm) and also took into account the reduction of the residual estate (by, for example, the money spent on the farmhouse). In addition, it included various elements which were designed to reduce the risk of a conflict between S’s interest as legatee and his duties as Mrs P’s LPA, and measures to reduce the scope for further disputes between Mrs P’s potential legatees during her lifetime (all relevant elements to considering Mrs P’s best interests).
However, none of the family members agrees with the Official Solicitor’s proposals. The daughter and the stepson who doesn’t inherit the farm argued that there was no need for a statutory will, and that that the 2005 will should stand: if the court does decide on a statutory will, they want a larger bequest from Mrs P’s will than is proposed by the OS. Meanwhile S is concerned that the fixed financial bequests the OS proposes should go to Mrs P’s daughter and other stepson could mean (depending on Mrs P’s future care costs) that they cannot be met from Mrs P’s liquid assets and that the farm would have to be sold. He says that selling the farm “contradicts totally the express wishes and feelings of every conversation he’s ever had with her”.
The parties are all represented by lawyers in court. I didn’t hear from any family member directly, but it’s clear that relationships between family members are strained. Obviously, a contest about the statutory will is unlikely to enhance family relations or support any ability to work together to support Mrs P. It must be painful, for example, for Mrs P’s daughter that her stepbrother has collected witness statements from Mrs P’s hairdresser, and from her friends and neighbours, in support of his contention that the relationship between mother and daughter was poor.
The hearing also revealed how knotted and tangled such cases can be. A will may include provision for passing on a family asset like a farm (perhaps passed down through many generations) and involve blended and multi-generational families (with children, step-children and grandchildren) and different types of inheritance arrangements which mean some inheritance might be fairly secure (or even enhanced by money being spent on them) whereas others are uncertain or depleted (as in the allocation of ‘residue’ from the estate). There may also be very different levels of involvements in care, different impacts of the care set up on potential legatee’s ability to earn, and disputed views about the nature of relationships.
The parties have agreed to mediation. If it fails there will be a two-day hearing at the end of 2025 or beginning of 2026.
Observing this case made me very aware of how complex wills can be – and how this is amplified when it comes to writing a statutory will, especially if there is conflict between potential beneficiaries.
It also made me reflect on my own experience of applying for a statutory will – and why in some ways it was so simple, and why, in other ways, it still felt so very difficult.
Part 2 – Applying for Polly’s (uncontested) statutory will
The aim of my application in May 2022 was to update a previous will my sister Polly had made 18 years earlier (in 2004) when she’d taken out a joint mortgage with her partner to purchase a lovely cottage in Wales – the first time Polly had owned her own home. She and her partner moved in together with great excitement and joy and wrote ‘mirror wills’ making one another each other’s primary beneficiary.
Five years later (in 2009), Polly was involved in a car crash which left her with devastating brain injuries. She now lives in a nursing home entirely dependent on 24/7 care. She lacks capacity to make her own decisions about, for example, medical treatment or where she lives and has profound physical disabilities too which severely limit her life and (originally at least) were expected to severely reduce her life-expectancy. An expert report in 2010 predicted she’d be unlikely to live beyond 2020.
The primary beneficiary of her original will, her partner at the time, was at Polly’s bedside almost every day of the eight months that Polly was in hospital following her car crash in 2009. She continued to be involved after Polly moved to a specialist neuro-rehabilitation centre and then on into long term care. But she eventually went on to rebuild her own life without Polly. In 2011 she sold their cottage and moved away, transferring Polly’s share of the equity into Polly’s bank account – an account that I manage as Polly’s finance deputy. She removed Polly from her own will in 2013 and has since married someone else. She chooses to have no contact with Polly any more. Her family is sure Polly would have wanted her partner to get on with her life in this way (and, indeed, some other members of Polly’s family made similar choices).
In this situation it seemed appropriate to consider a new will for Polly to take into account her changed circumstances. It also seemed clear that she couldn’t rewrite the will herself (nobody doubted but that she would be found to lack testamentary capacity), so it would be in her best interests to rewrite the will for her, which means making an application to the Court of Protection.
Making a statutory will, involves – like making any other best interests decision – consideration of the person’s past and present wishes and can also take into account a range of other issues such as inheritance tax, the potentially shifting value of different gifts (e.g. a farm versus the residue of the estate), or risks of (future or ongoing) family acrimony and litigation. You can see some such considerations in the Mrs P case I observed. None of these issues applied to Polly as her situation, and her finances, were very straightforward.
In thinking about the terms of a new will, I already had Polly’s 2004 will. That will, not only makes her partner her primary beneficiary, but also says what should happen if her partner died before her or the legacy failed for any other reason. Polly has no children or dependents: her will stated that if her estate did not go to her partner, then it should be equally divided between me and one of her other sisters, Tess (choosing the two of her four sisters with whom she had particularly close relationships). She had named me as her executor.
I tried (with little success) to ascertain how Polly felt about her will now. I then discussed options with Polly’s family and the one friend of Polly’s who has stayed in touch with her situation. Might, for example, Polly now have wanted to leave her money to charity? The consensus from those close to Polly was that in her new circumstances Polly would have wanted the money to go to her ‘second choices’ in her 2004 will – i.e. me and her other sister, Tess – both of whom are still directly involved in Polly’s life.
The appropriate course of action seemed to me fairly clear and, as Polly’s finance deputy, I have a duty to administer her finances in her best interests. But, in fact, I didn’t get around to applying for a statutory will until 2022 – arguably almost a decade after I should have done. I suspect I am not alone among lay people in this tardiness, so it’s probably worth reflecting on why such delays might happen.
2.1 Why I delayed applying for a statutory will
My failure to apply for a statutory will for many years after I was aware that it was appropriate to do so was partly because there were just too many other things to do. Polly went from one crisis to another, and I was very focused (especially in my additional role as her welfare deputy) on trying to ensure all medical interventions were in her best interests and, in particular, that decisions took into account her strong previously expressed wishes. I was working closely with my sister, Celia Kitzinger, to understand medical law and practice in this area. It was very time-consuming to try (and repeatedly fail) to ensure compliance with the Mental Capacity Act 2005 in situations where some medical staff seemed unfamiliar with the Act or unwilling to comply with it.
A great deal of effort was also needed to join up crucial aspects of Polly’s routine day-to-day care and for this I was working closely with my sister, Tess Kitzinger-McKenney. We felt that sisterly and welfare deputy input was needed in relation to a range of issues from trying to ensure care staff followed specialist guidelines about hoisting and correct positioning in her wheelchair to attempting to control her chronic pain. For many years, Polly also had episodes of “challenging” and “aggressive” behaviour – and sometimes only the presence of Tess or me would calm her; being with her was also particularly important for medical appointments (to ensure continuity, provide accurate history, convey correct information across sites etc.).
So I’ve lots of practical excuses, but I have to admit that my delay in sorting out Polly’s will was not just because of these challenges. I was also hesitant because of the potential conflict of interests. Over the many years since her brain injury, I’ve often argued in favour of ceilings of treatment for Polly (informed by evidence of Polly ‘s own wishes). This has sometimes prompted healthcare staff (mostly those unfamiliar with Polly or her family) to suggest that I want Polly to die so that I can inherit her money. Examples of this include (during one of Polly’s emergency re-admissions to hospital) a loud conversation between nurses in a corridor about my alleged financial motivations for resisting the reinsertion of her feeding tube – a conversation which seemed deliberately pitched at a volume that I could ‘over-hear’. During the same hospital admission, I returned to Polly’s bedside after nipping to the toilet to find a typed note stuck up above her bed. It was a quote from the bible that read: “The eternal God is your refuge, and underneath are the everlasting arms. He will drive out your enemy before you, saying, ‘Destroy him!’“.
Under such clouds of suspicion, and sometimes outright hostility, I felt more comfortable knowing that I wasn’t going to benefit from her will; it was her ex-partner (as long as she out-lived Polly) who would get everything.
2.2 Finding ‘the right time’ to apply
By 2022 updating the will felt long overdue. I knew that when Polly died (and she had already lived longer than originally predicted), I’d have failed to act on this aspect of her best interests. In particular I was sure that Polly would have wanted to leave money to Tess given the way that involvement in Polly’s care over the preceding 13 years had negatively impacted on Tess’s employment opportunities.
I was also aware that leaving the 2004 document as Polly’s last will and testament would put her ex-partner in an awkward position and leave a difficult situation for me at a time when I’d probably be dealing with layers of ‘complex grief’ myself.
By late 2021/early 2022 some pressures had also eased off. It felt like there was a bit of ‘breathing space’ because Polly’s placement seemed stable and her medication and nursing care well managed. She also finally seemed to be becoming more ‘settled’ . The “challenging behaviour” so evident for over a decade had become much less frequent: she’d become generally compliant, and there were fewer crisis calls.
I also wanted to get around to sorting Polly’s will at this point as I was acutely aware that our father (in his mid 90s) was needing increasing support and I thought that my role as his financial LPA and as his executor might become a big demand in the near future.
As it turned out not only did our father die the following year, but both Tess and I needed hospitalisation for our own medical issues. In the same year, Polly’s placement deteriorated after key staff left, including the excellent home manager and Polly’s wonderful key worker. A general staffing crisis followed. Then a CQC inspection found residents were at risk of abuse and neglect and the home was closed down. We had to move Polly with 28 days notice, and the only place we could find, and that the CHC agreed to pay for at the time, was a dementia unit.
Sometimes I’m grateful not to have a crystal ball to know the future. But – given what happened in 2023 – certainly 2022 was the window of opportunity that needed to be taken if an application for a statutory will were to be made!
2.3 Submitting an application – the practical steps
In early 2022 I looked up how to apply to get approval from the OPG for a statutory will on the government website here: https://www.gov.uk/apply-statutory-will
I set up a new OneDrive folder and all the sub-folders I’d need matched against the Office of the Public Guardian forms and labelled a bright yellow ring-binder ‘Statutory Will’ – with an optimistic sense that it should not be too difficult.
I wasn’t completely naïve – I’ve dealt with a lot of legal, financial and medical forms as Polly’s deputy – so I expected to face some unfamiliar language (I’d already had to look up the legal meaning of ‘engrossed’) and I also thought I might sometimes get in a bit of a tangle. To cheer me on my way I pinned up one of Polly’s cartoons above my computer. Polly had sent me this when she was a student; it captured the difficulty she was having writing an essay, caught in a tangle of vocabulary. This little sketch made me smile each time I looked at it, and provided a bit of sisterly solidarity from the past.
The application process started well. How to apply for a statutory will is clearly explained on the government website: https://www.gov.uk/apply-statutory-will. To start with, there’s an 8-page generic COP1 form to complete. This details the nature of your application. An explanation of each question and how one might answer it is helpfully included at the end of the form
The application also needs to include an up-to-date professional assessment of the person’s (lack of) ‘testamentary capacity’ (the COP3 – ‘Assessment of Capacity’ form) and a draft of the proposed statutory will.
Assessing testamentary capacity: I commissioned an experienced psychiatrist who works as a Special Visitor for the CoP to assess Polly. She examined relevant medical documentation and met Polly to assess her and to attempt to ascertain Polly’s current feelings about her will. This was not an easy task. Polly has profound cognitive and communication difficulties which can make it hard to interpret what she might be feeling or what she might know. For example, she recognises her own name (and the names of her parents and sisters) but quite what she knows or ‘recognises’ about herself and her family is unclear even though she seems to trust us. It certainly seems that she has little or no memory of her adult life, no understanding of her current condition and is unable to retain significant new information (such as the death of her mother). The expert assessment was consistent with our expectations. It found that, as a consequence of her brain injury, Polly was unable to retain any information for more than a few seconds or to weigh choices against each other. It also found that “Ms Kitzinger is not oriented to her own situation”, doesn’t understand “her own living situation, care needs or financial affairs”, did not know who she had been in a relationship with previously and that she specifically lacked the capacity to make a will.
Drafting the proposed statutory will: In order to provide the court with a draft statutory will I went beyond my early informal conversations from years earlier to formally consult those who knew her, and I again attempted (without much success) to ascertain Polly’s own wishes and feelings. I found getting back in touch with Polly’s ex-partner an emotional hurdle to overcome as we hadn’t been in contact for a while and I knew she found it upsetting to think about the trauma of Polly’s car crash and its aftermath. She was very willing to help however, and made it very clear she had no expectation or wish to inherit from Polly and that she supported the proposed re-writing of Polly’s will. There was a clear consensus from all concerned that the statutory will should simply remove Polly’s ex-partner so Polly’s money would go to me and Tess as the primary beneficiaries. I also proposed adding, that, if either of us died before Polly, each of our portion should go to Tess’s children (Polly’s much-loved niece and nephews).
Forms about finances, family tree and other facts: In addition to the CoP1 (application form), COP3 (Capacity form) and the draft will I needed:
COP1a ‘Annex A form “Supporting information for property and affairs applications” – this provided information about Polly’s assets
COP1c form “Supporting information for statutory will, codicil, gifts(s), deed of variation or settlement of property form”.
CoP24 form – my witness statement about why a statutory will was needed.
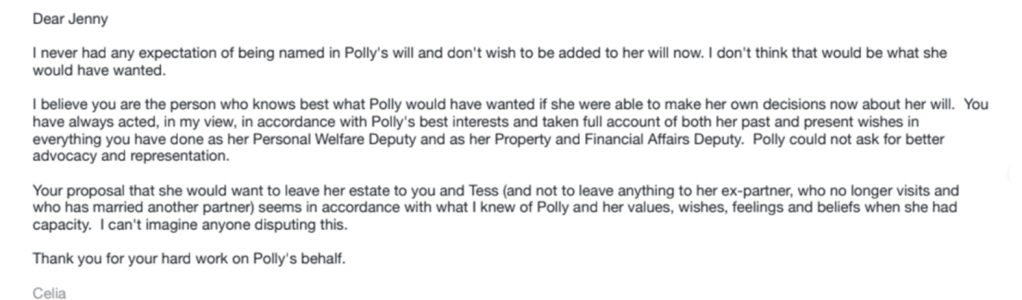
I also had to submit Polly’s original will from 2004 and a family tree showing Polly’s family connections, along with statements from people who might be seen (at least by the OPG) as having a reasonable expectation to inherit. See below for an example, a statement from my sister Celia confirming that she had no expectation, or wish, to benefit from Polly’s will.
Finally, I needed to provide evidence of ‘consent to act’ in relation to the executor of the new will. See the rather convoluted email below that I ended up writing to myself as evidence for this purpose!
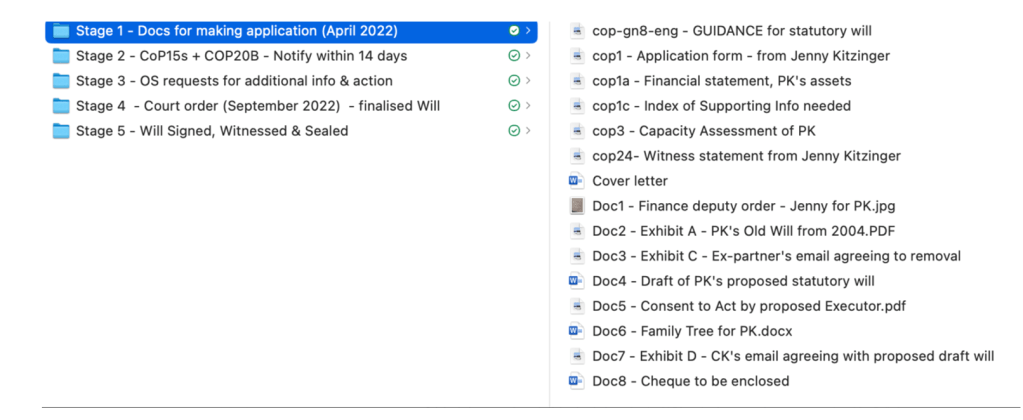
My computer folders for stage 1 of the process (putting together the documents for the application) is shown in the screenshot reproduced below. You can see “Docs for making application” is one of my folders on the left – and everything I needed for the application is listed in the right-hand column.
You’ll also see from the screen shot that there were several further steps to go through before the will was finalised and sealed (authorised) by the court.
But at this stage (Stage 1), I was just relieved to print everything out (as apparently paper copies had to be submitted) and to enclose a cheque to cover the (approximately £400) fee for the application. The requirement for a cheque was one of the more surprising aspects of Stage 1 given that I hadn’t used one for many years. But I eventually found an old cheque book, took everything down to the post office and then went straight to a café for a ‘reward’ of hot chocolate and a slice of lemon-drizzle cake.
2.4 Action needed between submitting the application and the order authorising me to execute the will
I submitted the application to the CoP on 8th April 2022. On 25th May 2022, an order was issued (by DJ Beckley) ordering that Polly be joined as a party to proceedings and inviting the Official Solicitor to act as Polly’s litigation friend. The case number assigned was COP 11757133-04.
I was pleased to see that DJ Beckley’s order emphasised the need to resolve the matter as quickly as possible and with the minimum possible expense to Polly (referring to Rule 1.1 of the Court of Protection Rules 2017). It set a deadline of 17th August 2022 (almost 3 months from the date of the order) by which time the court should be notified whether it was likely that the parties would reach an agreement, when they’d be able to file a proposed consent order and whether a hearing would be needed.
I then received a letter from the Official Solicitor accepting the appointment, stating her fees (£228 to £360 plus VAT per hour), and asking for further information.
At this point there was a bit more work for me to do as the applicant. This was in relation to three forms:
COP15 forms – “Notice that an application form has been issued” – had to be sent to relevant parties (this included Polly’s ex-partner and my sisters, but also Polly’s niece and nephews). This gave them the opportunity to be joined as parties and they could have intervened if they wished. (In the case of Mrs P it may have been this process which alerted her daughter and other stepson.)
COP20B form – this needed to be sent to the OS, confirming that I’d served the COP15 forms.
COP14 form – this had to be sent to Polly (with a copy to the OS) notifying Polly that the OS had been appointed as her Litigation Friend. I completed the form and posted it to Polly at her care home. I opened the envelope myself a few days later when I visited and read the form out to her and explained it to her as she stared into space. I tried again another day – but she appeared rather disinterested.
I also had to serve ‘the Official Solicitor and each party’ with the application and copies of all the documents I’d submitted to the court. To my surprise there seemed to be no shared system for lodging and sharing such documents efficiently. I also had to go back to some paperwork at this point as the letter from the OS explained that the OS found it useful to have documents in word format rather than pdfs (a lesson learnt there – I now always try to ensure I store word versions of documents as well as pdfs).
An unexpected and difficult bit of paperwork for this part of the process was the request from the OS for an up-to-date assessment of Polly’s medical condition which should include “an assessment of life expectancy, and the likelihood of Ms Kitzinger requiring increased expenditure in the foreseeable future for their care need”.
The letter from the OS stated this was ‘ordinarily’ provided in the COP3 form – but, in fact, the COP3 form did not have a section spelling out the need for this particular information and it had therefore not been included in the assessment I’d commissioned. Nor could I see how such information could possibly impact on whether or not the statutory will I had proposed was in Polly’s best interests. I surmised at the time that the question might be relevant for life-time gifts and that I’d just been sent a standardised letter. Having observed the Mrs P hearing, I now realise it is also relevant where a will might give an asset such as a house to one beneficiary and the ‘residue’ of the estate to others as life-time expenditure (related to how long someone lives and their care costs) will impact on the value of the residue. However, this was not relevant to my proposal for Polly’s will.
The request from the OS was also not an easy request to fulfil as no one now seemed willing to make an assessment of Polly’s life-expectancy. But I eventually persuaded Polly’s GP to provide a verbal statement.
I got all the second set of paperwork I had to provide back to the OS by 30th May and then waited. On 18th of August 2022 the OS emailed the court saying there was no intention to do detailed submission – and attaching a 3-page summary of what I’d demonstrated. The OS said the proposed statutory will was in Polly’s best interests and attached a draft order for the judge.
On 23rd September 2022, the Court sent me the ‘approved’ draft will. This was the same as the draft will I’d submitted but with some numbering added and some necessary phrasing added at the beginning and end of the document (see below). The order from District Judge Ellington (made 2nd Sept, issued 23rd Sept 2022) stated that “upon reading the draft statutory will (initialled by District Judge Ellington for the purpose of identification)” and reading other relevant documents she authorised me “to execute a statutory will in the terms of the said draft”.
2.5 Getting the statutory will signed and sealed
At this point it was ‘just’ a question of getting the will signed, witnessed and sealed. The format of the approved will was as follows. The opening lines that had been added to the draft I’d prepared stated: “This is the last will of me POLLY KITZINGER of [her placement address] acting by JENNY KITZINGER the person authorised in that behalf by an order dated the [date] day of [month, year] made under the Mental Capacity Act 2005“.
At the end of the draft statutory will there was the addition of an ‘Attestation” reading: “In witness of which this will is signed by me POLLY (MARGARET) ALEXANDRA KITZINGER acting by JENNY VANESSA KITZINGER under the order mentioned above on [date]“.
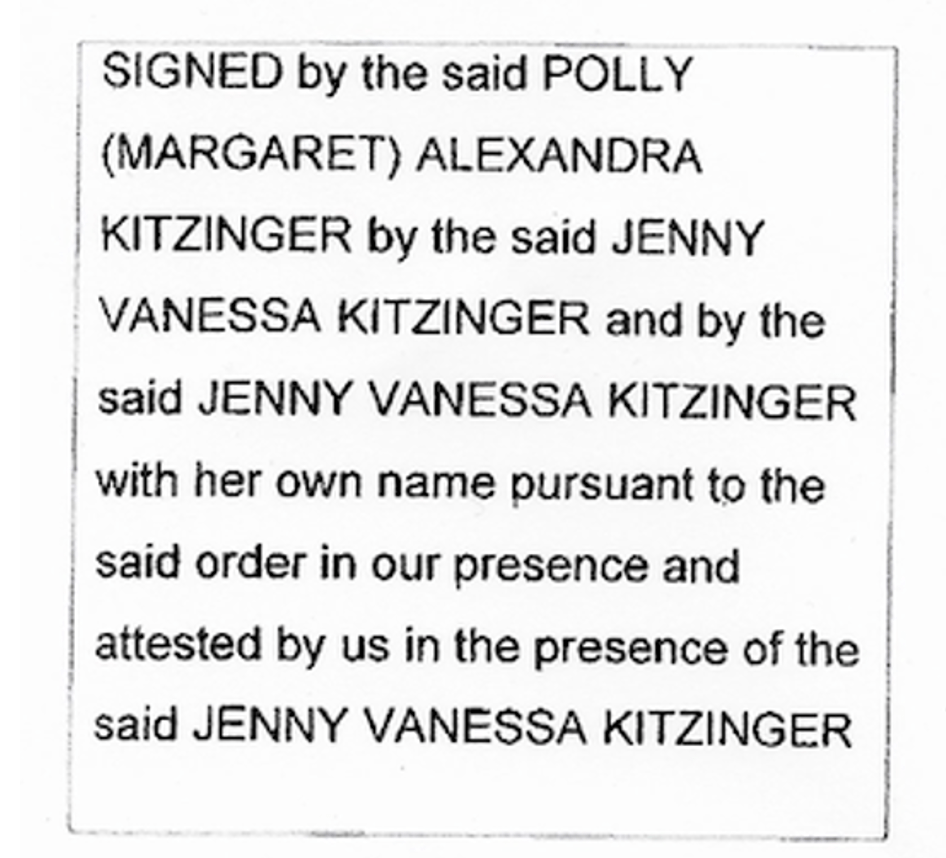
This was followed by a box which read as follows.
I was a bit baffled by some of this phrasing but worked out that I should sign twice (once as if I was Polly, using her name). The two witnesses to my signature then added their signatures (and name, address and occupation). I then added a ‘certificate’ to the end of the will as instructed in the format below – which also had to be signed by me.
“I/We hereby certify that this will is an exact copy of the draft thereof as approved by the Court
Signed………
Dated……..”
I had to have two copies bound (the will was just one page, but signatures took it to two pages long) and sent it for sealing.
Unfortunately, it was subsequently returned unsealed as the copy of the will I used was the approved copy sent to me by the court with the judge’s initials on it. So I was told to redo all the signing and witnessing on a copy without the initials and go through that bit of the whole process again!
The will was finally back with me in November 2022 (about 8 months after I started the process), with the addition of an embossed imprint on the pages and the words “Sealed with the official seal of the Court of Protection 15th November 2022”.
My application was a long drawn-out out process. It’s possible to make an emergency application (e.g. when P is dying), and these can be dealt with amazingly swiftly, although of course there is always the risk of these applications being resolved too late.
Part 3 – Reflections
Statutory wills can involve very complex issues and therefore be challenging to apply for, and to secure. I was lucky in that it was relatively easy for me given the simplicity of Polly’s financial affairs and the lack of any family tensions about what a statutory will should say. Nevertheless, parts of the process were difficult.
Emotional toll: I’m in a family where everyone can talk easily about death (and money) so the subject of will-writing itself was not taboo and we’d lived for a very long time with the expectation of Polly dying. However, the application involved quite a bit of emotional labour.
The need to think about what Polly would have wanted, and try to access her current wishes, is core to what I do as Polly’s deputy but it’s always hard, whatever the decision. This is because her current situation is so far from anything she would have wanted, and because her ability to process, express, (or obtain) what she might currently want is so very limited.
For this particular decision I also had to approach relevant people who no longer had contact with Polly in order to consult, or at least inform them, about the application. This was difficult because I knew that this would cause distress. It clearly upset her ex-partner, for example, who although fully supporting the application also subsequently wrote to say she’d found it traumatic to have to re-engage with anything about Polly. She wrote to say she was sure we would do the right thing in relation to Polly and hoped she could be completely left out of any future consultations and court proceedings.
A part of the application process which was also stressful was the need to seek out up-to-date life-expectancy predictions as requested by the OS for the statutory will application. I was not surprised that it was hard to get anyone to answer this question, nor did it surprise me that her GP eventually responded by confirming that although Polly might die very soon (e.g. from pneumonia) she might also live a normal life span. It was upsetting, never-the-less, not least because it underlined the fact that Polly might outlive her sisters and be left without what little protection and support we’re able to provide.
Ill health and other challenges to come: The emotional context therefore had its challenges but I also remember the application process and paperwork just feeling overwhelming at times. This is surprising in some ways as I had a demanding job and am used to putting together major and very detailed research applications. While writing this blog, I went back and checked the dates and realised I was also beginning to become ill in 2022 with an (at the time) undiagnosed condition which needed major abdominal surgery the following year. Neglecting one’s own health needs is not uncommon among families supporting someone with profound disabilities and my medical condition probably also undermined my resilience and efficiency. Although early 2022 had felt like a good window of opportunity to apply for the statutory will, other pressures also built up during the months that the process dragged on, including problems with Polly’s day-to-day care. Looking back, I can now see why I was so demoralised when the will ‘boomeranged back’ because I’d submitted one which had the judge’s initials on it and another copy (without the judge’s initials) needed to be re-printed, re-signed, witnessed, and returned. This was a relatively simple process, of course, but I’d thought it was all sorted and was desperate to tick off this task among all the other tasks I needed to do.
Death by a thousand papercuts: The general context of administrative burden is also probably relevant. Applying for a statutory will is one more administrative task among a plethora of others – and another one that sits in one’s in-tray for weeks or months (or even years!) as other organisations go through their own processing of the paperwork. Being a deputy (or/and an LPA or an executor) can involve lots of unfamiliar paperwork which, I suspect, can take anyone close to the edge of their own tolerance or competence. I often made mistakes and had to work hard at proof reading and avoiding basic errors. The anthropologist, David Graeber’s, book on ‘The Utopia of Rules’ and his account of ‘structural stupidity’ provides insight into how this happens! A lot of energy went on coping with the everyday frustrations too: printer paper jammed, ink ran out, attachments disappeared, computer glitches thwarted me. In addition, the interface between myself, the OS and CoP did not always go smoothly. Everyone was trying to be helpful but the application system seemed old-fashioned or unclear at times (e.g. the need for a cheque book or the request for word versions of documents at a point when I’d only saved them as pdfs). Interactive forms also didn’t always work e.g. the COP3 form would not accept the capacity assessor’s electronic signature: she’d never had this problem when dealing directly with COP3 forms for lawyers – so maybe they have some magic software. In addition, I had the sense that I was dealing with professionals under a lot of pressure themselves – I was informed that a new case management system was “bedding in” and errors were made at their end (I think) which in turn put a series of micro-anxieties on me e.g. a ‘password-protected’ document arriving without follow-up passwords; a document with a request to sign and submit to the Court that arrived after the deadline for submission had passed, and a letter (the one containing the final sealed will) which was initially delivered to a neighbour’s address as the house number had been mistyped. Also, three years later, I have still not been sent an invoice so that I can pay the Official Solicitor for the work she did on Polly’s case (despite recently receiving an email “enclosing the Final Cost Certificate for your attention” and telling me an invoice would arrive by post “soon”). This makes additional work for me as Polly’s finance deputy – recording the debt in my returns, ensuring I’ve kept funds aside to pay it, awaiting the invoice in the mail every day now and wondering when to chase in case it’s gone to wrong address. In the course of writing this blog I’ve reluctantly come to the conclusion that I’d recommend (if affordable) employing someone to help make an application for a statutory will. I’d recommend this even if it looks like you can do most of it yourself, and would still have to work alongside any professional you employ, and it doesn’t take away all the challenges – at least you’ll have someone who’s done it before, knows the process, has the right software interface and can support at least part of the process.
Surveillance and submission: The added context here is one in which one can sometimes feel powerless in relation to many (hard-pressed) institutions supposed to be supporting one’s vulnerable relative (e.g. health and social care provision) and where the OPG and COP role in safeguarding can sometimes feel like suspicious micro-management and another drain on the family love and energy rather than a supportive protection. Mark Neary has written very powerfully about this, documenting his experience as Finance Deputy for his son. He makes explicit the tensions that can arise between making things work for his son in his role as his father on the one hand and fulfilling the demands of the OPG on the other. He also highlights the impact of ‘micro-management’ and of the ‘tone’ with which the OPG can approach family members. He describes, for example, a conference in Leeds where ‘the top dog in the Property & Affairs Deputyship department at the OPG’ gave a talk which consisted of “anecdote after anecdote of family members ripping off their vulnerable relatives. The hero and villain roles were bluntly cast and all Deputies learn over time that they are not seen as a reliable, loyal Woody, but as a sinister, Stinky Pete, who is ready to sell out his friends for his personal gain at the drop of a stetson.” Mark Neary adds: “My memory of the first few years of deputyship was of a time of constant anxiety; expecting the woman from Leeds to arrive at my door because I mislaid the receipt for The Proclaimers greatest hits CD.” [“Woody Gets A Partner”]
When a system is set up to ‘protect’ P, it needs to not just safeguard against abuses but keep in mind the need to protect (or at least not drain and undermine) any positive support network around P. The devil is in the detail. It has to go beyond reiterations of the so-called ‘overriding objective’ to deal with the matter expeditiously and fairly and at proportionate cost (Civil Procedure Rules 1.1). That can only happen if the bureaucratic process works smoothly.
Was it worth it? A zero-sum game in family energy? Making the application means I have fulfilled my duty in relation to Polly’s best interests around her will. I’m glad the application succeeded and it is one less thing to deal with in the future. But I have regrets. When I started the application process, I did not know that both Tess and I would soon need major surgery, nor that, during that time, there would be a rapid deterioration in Polly’s placement and that Polly would end up in a dementia unit, losing access to specialist neuro input, rapidly followed by losing her CHC funding. I wonder if this cascade of events might not have happened in the same way if our energies had not been so depleted at the time. Did the effort I put into navigating the safeguards put in place to ensure any statutory will was in Polly’s best interests leave her more vulnerable to being at risk of neglect and abuse in her placement? Did my pursuit of an arguably peripheral part of her best interests (what would happen after she died) mean I took my eye off the ball to protect her current best interests, or at least leave me dangerously overstretched and at risk of reduced vigilance (especially once my own health issues kicked in)? Family energy to support any ‘protected party’ is a zero-sum game. Juggling priorities and knowing that sometimes we will fail has become a necessary part of the journey – and sometimes that may mean not pursuing something that, ideally, we should.
In conclusion, I am glad that that the option of creating a statutory will does exist in England and Wales (it doesn’t in Scotland and many other jurisdictions). I endorse the value of statutory wills as part of a 360-degree assessment of best interests – and think they are a valuable tool in some, but not all, circumstances – both for practical and for principled reasons. In Polly’s situation the principle of ‘updating’ her will in line with what we thought she’d want in her changed circumstances was pretty straightforward (and also clearly in her best interests). But I agree with Rosie Harding that there are different issues at stake when the Court of Protection is asked to write a will in the ‘best interests’ of someone who’s never had testamentary capacity, or for a person who has previously had testamentary capacity, but who is intestate.
If you are in a position of making an application to the court for a statutory will, I think the guidance offered on the OPG website is helpful and the forms are generally well-designed. In many ways the system seems to be working well, and there is clearly a judicial commitment to making the process transparent – a commitment reflected in, and contributed to, I hope, by this blog post. In hearings I observed, I’ve seen the Official Solicitor carefully try to navigate a resolution in cases of family conflict (as in the case of Mrs P), and I’ve seen how a judge can quickly and effectively address best interests where there is unresolvable conflict in an emergency situation (as in the case of Mr R, the dying man I wrote about in an earlier blog). I’m also grateful that the judge who assessed my own application concluded that it did not need a hearing and could be decided on the papers – thereby avoiding what could have been an expensive and time-consuming extension to the process. This seems a proportionate and sensible way of approving some uncontested statutory wills without overburdening the court system.
One of my aims when I set out to write this blog was to share my experience to help others understand the process and perhaps feel less daunted by it. In the course of writing it, I have come to realise that another outcome may be to forewarn people entering into the process who may perhaps imagine that it might be be rather more straightforward than it is likely to turn out to be in practice. While encouraging everyone to consider whether they should be applying for a statutory will, I would also warn any lay person against taking on trust that the process is as simple as the initial instructions make it appear. As I hope this blog has illustrated, even a very straightforward application can have its complexities for the person making it and for the other people implicated in the decision. I don’t want this blog to deter anyone from making a statutory will, but I do hope it will help them to pace themselves and be prepared for some of the challenges.
At an institutional level I don’t think I have any big ideas for improvement beyond the general point about the need for efficiency, sensitivity, and minimising any unnecessary requests or disproportionate obstacles – but I would welcome any feedback from those working with the OPG or COP if this blog post prompts any thoughts from their perspective.
[1]For more information about the law on statutory wills see “Statutory wills: A barrister explains”. For practical guidance and access to the relevant forms see the government website: https://www.gov.uk/apply-statutory-will/getting-a-decision (and “Age Space” also gives helpful guidance here). For academic analysis of statutory wills and discussion of case law see: Harding, R 2015, ‘The rise of statutory wills and the limits of best interests decision-making in inheritance’, Modern Law Review, vol. 78, no. 6, pp. 945-970. https://doi.org/10.1111/1468-2230.12156 (Author’s version: click here). Milward K, Curtice M, Harding R. Statutory wills: Doing the right thing under the Mental Capacity Act 2005. BJPsych Advances. 2017;23(1):54-62. doi:10.1192/apt.bp.116.016022
By Matthew Evans and Eleanor Sibley, 7th December 2025
On 20-22 October 2025, the Supreme Court heard a Reference by the Attorney General (AG) for Northern Ireland asking it to re-consider its judgment in Cheshire West.
Its decision, made in the absence of a concrete factual matrix, will have far-reaching and very concrete consequences.
The AIRE Centre is a specialist human rights legal charity, which uses the power of European law to protect individual and collective fundamental rights [The AIRE Centre]. The AIRE Centre intervened in Cheshire West and applied to intervene in the AG’s Reference but was refused permission.
In this blog post, we consider the background to the Reference and some of the principles of European and international law that we hoped to put before the Court.
The AG’s Reference
The subject of the AG for Northern Ireland’s reference was the subjective element of the test for a deprivation of liberty under Article 5 ECHR.
This is one of three parts to the test:
The objective element of being confined in a restricted place for a not negligible length of time (this was the primary focus of the appeal in Cheshire West;)
The subjective element – a lack of valid consent; and
Attributability to the state.
In Cheshire West the subjective element of the test was not in issue. However, the Supreme Court made some observations on it. Based on those observations, it appears to have assumed that if a person lacks mental capacity to consent to an objective confinement, then there can be no valid consent for the purposes of the subjective limb.
It was this assumption that the AG for Northern Ireland asked the Supreme Court to reconsider. She argued that even when a person lacks mental capacity to consent to confinement, valid consent may be given through the expression of wishes and feelings going beyond mere acquiescence.
By the time of the hearing in October 2025, the case had taken on a life of its own, and the Supreme Court heard submissions on whether it should revisit its judgment in Cheshire West in its entirety.
The central issues to be resolved by the court are ones of legal principle, given there is no protected party or concrete factual matrix to consider in this case. Nonetheless, they will have important consequences.
The background to the Reference
The background to this issue is long and complex, but we should start with what Cheshire West decided.
The Supreme Court was primarily concerned with the objective limb of the test for a deprivation of liberty. It sets out what has been described as an ‘acid test’ according to which people who are under continuous supervision and control and not free to leave are subject to objective confinement. The Supreme Court found that this is so even if they seem content or unaware of it. and even if their living arrangements are comfortable and make their life as enjoyable as it could be – memorably described by Lady Hale in her judgment, as a ‘gilded cage is still a cage.’ Lady Hale’s view was that what it means to be deprived of one’s liberty must be the same for everyone, whether disabled or not. [46]
Based on the court’s observations on the subjective limb, it has been widely assumed that where the ‘acid test’ is met, and the confined person lacks mental capacity to consent to their confinement, both the objective and subjective elements of the test for a deprivation of liberty will be met.
A number of criticisms have been raised in response to the court’s decision in Cheshire West, and how this has been applied in practice.
Some of these are set out in various submissions before the UK Supreme Court. See, for example, paragraphs 52 to 55 of the Secretary of State’s written case. They include:
That it is too resource heavy. There are currently a staggering number of Deprivation of Liberty Orders (DoLS), resulting in significant assessment wait periods. This is exacerbated by the fact that where a person moves to a new placement, a new authorization is needed;
That, as a result, people are being unlawfully deprived of their liberty for a very long time, and there is an attendant risk that a number of people will risk being detained inappropriately and/or in circumstances where they have capacity to make decisions about where to live and receive care.
That the interpretation of what Article 5 requires in Cheshire West goes too far (Mr Justice Mostyn has led this charge.)
Elsewhere, in European Court of Human Rights and Mental Health (Eldergill, Evans and Sibley (2024), Bloomsbury Professional, London), Anselm Eldergill set out 17 relevant issues that need to be understood or considered when deciding if someone in a care setting is deprived of liberty.
Eldergill believes the Cheshire West approach does not properly distinguish between capacity, liberty, and autonomy. In his view, one of the relevant factors is what he calls the ‘but for’ test (‘Eldergill test’), where the decision maker must ask, ‘What are the things this person can do and wishes to do (‘wills’) but has not done because we have interfered or are interfering with their freedom to do them?’
Where a person has advanced dementia or a significant brain injury, Eldergill argues that the answer may be nothing or not enough to constitute a deprivation of liberty. The individual’s ability to act autonomously, to be self-directing, has been reduced not by restraints on their freedom imposed by others but by their own reduced abilities. The effect of their increasing dementia ‘is that they are now incapable of doing many of the things which previously they were able to do. Although they may be wholly unable to self-care, and so be under our complete care and supervision, we are not interfering with, limiting, or ‘controlling’their liberty to do anything which they can do. Hopefully, we supervise and control what others do to them or for them but at this stage their own actions are not being controlled by others.’
However, others – including Mencap, Mind and the National Autistic Society, who intervened in the AG’s Reference – are concerned that if ‘deprivation of liberty’ is defined more narrowly, than in Cheshire West, there will be a loss of important procedural protections for people who are vulnerable by reason of disability. In Cheshire West, Lady Hale decided, for similar reasons, that there is a need to err on the side of caution when deciding what constitutes a deprivation of liberty. [§57]
Article 5 in the National Law Context
Deprivation of liberty’ is a phrase that appears in international standards, each time with a different context and emphasis and several international institutions are also concerned with the right to liberty and security of person.
They include most obviously the definition given in Article 5 of the European Convention on Human Rights, which is enforceable in the UK by reason of the Human Rights Act 1998 (HRA 1998). It is also incorporated by section 64(5) Mental Capacity Act 2005 (‘MCA 2005’) which provides that ‘deprivation of liberty’ has the same meaning in domestic law as it has in Article 5 ECHR.
The safeguards against arbitrariness required by Article 5 in the UK mental health Context are also contained in the MCA 2005. This gives authority to deprive a person of their liberty in only three circumstances: first, where the Court of Protection authorises it; second, where it is authorised under the Deprivation of Liberty Safeguards scheme set out in Schedule A1 of the MCA 2005); and third, in certain emergency cases on an interim basis, where an application has been lodged at court, and pending court approval.
These UK law provisions attempt to ensure that deprivations of liberty of people with mental health problems are subject to independent scrutiny in compliance with Article 5(4). They function as an important ‘gateway’ to such scrutiny. This is why it is important to have clarity as to the test for determining when a deprivation of liberty has occurred.
Article 5 in the International Context
International perspectives can provide insights that may be valuable when formulating the meaning of ‘deprivation of liberty’.
In terms of what amounts to a deprivation of liberty, the ECtHR has indicated that the objective limb of the test in respect of the concept of deprivation of liberty, which was the primary focus of Cheshire West case, is met in respect of “confinement in a particular restricted space for a not negligible length of time (the Storck test, which comes from case of Storck v Germany). This requires consideration of the concrete situation of the person concerned (differentiating between deprivation and merely restricting liberty).
The ECtHR has stated that “the key factor” in determining whether there was a deprivation of liberty in mental health cases is whether the management of the care homes in question exercised complete and effective control over the person’s treatment, care, residence, and movement. (see DD v Lithuania)
There is, however, a relative lack of Strasbourg case law on the factual situation with which the Supreme Court in Cheshire West was concerned, and about the ability of people who lack de facto capacity to make decisions about their care arrangements (i.e. who lack the ability to make such decisions as a matter of fact) to give valid consent.
This may, in part, be because of barriers to people who lack capacity in relevant regards bringing cases before the ECtHR (and domestic courts). Some member states have legal frameworks that prevent those who lack capacity as a matter of law (de jure capacity) from exercising some or all legal rights (see, e.g., ET v Moldova [2024] ECHR 858.) There are also strict time limits for bringing cases before the ECtHR, and which are more difficult for those who lack capacity to meet. The ECtHR’s mandatory representation rules (which require legal representation once a case has been communicated), combined with a lack of any settled policy for providing representation to persons lacking capacity has led, on occasion, to cases being struck out where they may otherwise have proceeded. Finally, litigation concerning the rights under the Convention for those who lack de jure or de facto mental capacity to make certain decisions is still a relatively recent phenomenon.
As well as the ECHR, there are also various other international instruments and bodies which are important in relation to the understanding of contemporary attitudes towards the right to liberty in a mental health context. These include the European Committee for the Prevention of Torture and Inhuman or Degrading Treatment or Punishment (“CPT”), the UN Convention on the Rights of Persons with Disabilities (CRPD), and bodies such theCommittee on the Rights of Persons with Disabilities (the CRPD’s supervisory body, which requires all states to report it every four years on progress towards implementation of the CRPD). The Convention on Human Rights and Biomedicine (the Oviedo Convention) and the Council of Europe’s Resolution 1859 (2012) on protecting human rights and human dignity are also of relevance to the meaning of “valid consent.”
Options open to the Supreme Court and the AIRE Centre’s application to intervene
It is not known whether the Supreme Court will maintain the status quo, moderate the Cheshire West test or reverse it totally. Its decision will have important consequences for large numbers of people who are confined to care homes, hospitals, and other settings, and who may lack capacity to challenge this confinement.
As Peter Mant KC and Nicola Kohn observed in their post on the Attorney General’s reference, it is inevitable that in many cases, the Supreme Court Justices will not have intimate subject-matter knowledge. This is where intervenors, as well as specialist lawyers, can be of value. The AIRE Centre had hoped to assist the court in making this decision by drawing on its expertise in European human rights law, and its international context. We hoped, in particular, to assist by:
Surveying the case law on the importance, and function of Article 5 within the context of the Convention, including:
Its essential purpose of protecting against arbitrary deprivations of liberty;
Its importance within the convention – it, along with Articles 2, 3 and 4, is within the “first rank” of Convention rights), which is of potential relevance to arguments concerning the interplay between Article 5 and 8 rights;
The state’s positive obligations under Article 5, which include taking steps to protect against arbitrary deprivations of liberty of which they know or ought to have known;
Particular obligations towards people who lack (or may lack) capacity to challenge an objective confinement themselves, and the procedural protections that are required as a result. These include, for example, an obligation to ensure that their right of challenge does not depend on the exercise of discretion by a third party, to ensure that they are afforded independent representation, and to make sure that they are not only entitled but enabled to challenge a deprivation of liberty.
Surveying the case law on the subjective limb of Article 5, and examining how this may apply in the domestic law context;
Drawing on relevant principles from the broader, international law context, including:
The approach to valid consent in the Oviedo Convention and Resolution 1859 (2012) on protecting human rights and human dignity; and
Case law that sheds light on the approach to valid consent across Contracting States;
The AIRE Centre was represented in its application to intervene by Peter Mant KC, and Nicola Kohn of 39 Essex Chambers, instructed by Sarah Westoby of Leigh Day, all acting pro bono.
Matthew Evans is Director of the AIRE Centre. Prior to this he was Director of the Prisoners Advice Service and in private practice, where he specialised in mental health, community care and public law. He has been involved in 20 cases before the UK Supreme Court and numerous cases before the ECHR. He is a co-author of European Court of Human Rights and Mental Health published by Bloomsbury in 2024
Eleanor Sibley is a barrister at Garden Court Chambers and the AIRE Centre. Her areas of practice include Court of Protection and related areas of human rights law. She was junior counsel in Re D (A Child) [2019] UKSC 42, which concerned the meaning of ‘deprivation of liberty’ for 16- and 17-year-olds who lack capacity to consent. She is a co-author of European Court of Human Rights and Mental Health.
“It’s his own home”. That’s what the mum of the protected party (I’ll call him “JC”) told the court. JC has been living in his current home for about 10 years, but listening to what was said in this hearing, it didn’t seem much like a “home” to me.
JC has been diagnosed with severe learning difficulties, autism and PTSD, and has significant care needs. He is currently being cared for by a care provider that I can’t name, with care commissioned by a Local Authority (LA) and an Integrated Care Board (ICB) that I can’t name either, due to the reporting restrictions in this case.
And after this hearing he will continue to be cared for by the same provider, because there is no other option. The judge, District Judge Matharu, made it clear to the family that she has no authority to order the LA and ICB to commission a different care provider for JC. And the LA and ICB position is that there is no other available option.
What is particularly shocking about this case is that there is CCTV from August to November 2024 that (according to the LA and ICB) “raised concerns”[1] about JC’s care. These include employment of staff without the relevant expertise, who failed to offer JC appropriate occupation and stimulation, and “the timeliness of interventions when JC soiled himself/the floor, staff sleeping, or inappropriate use of their phones and other matters”. The public bodies say that this has now been investigated, safeguarding referrals completed and changes have been made. The Position Statement for the LA and ICB states “Some staff have been removed from his care package. Others have received final warnings and further training”. These “others” are still caring for JC.
The family, who first raised the concerns on viewing the CCTV, are appalled by what happened and there is a “near breakdown of relations between the care provider and family members”. Both JC’s brother and his mum referred to what they had seen as “abuse”: they wanted a change of care provider.
JC’s brother and his mum wanted the judge to view some of the footage. In trying to persuade the judge to look at it, JC’s brother said, “A picture paints a thousand words and there are thousands of words in the bundle.” His mum added that the “CCTV makes JC human, not just words on a page”. But Adam Fullwood, of 39 Essex Chambers, representing the ICB and LA, argued that the judge didn’t need to look at the footage, because Mark Caulfield, the court appointed Independent Social Worker (ISW), had. He’d had “unfettered access.” The judge initially said that she would look at “a couple of incidents …. with nobody else in the courtroom” because the family had asked her to. In the event, the way the hearing panned out, I don’t think she did. She did, however, acknowledge the gravity of what the CCTV contained.
In an unusual move that I haven’t seen before, the judge, DJ Matharu, arranged for the sealed order to be drawn up immediately, at the end of the hearing, and it was printed out (by the judge herself) for the family. Afterwards, the judge made what she called “final observations”. She said (as best I could capture it):
“That concludes the hearing except for the following …I don’t want comments or responses. ..For the benefit of everyone, this isn’t a win or lose for anyone…. The position the court was in was that there was no alternative option (to staying with the current providers)…. To the credit of those involved in (JC’s) care, after video footage … steps have been established to provide a better environment .. .. As much as (mum and brother) look to the future ..I want the carers to collaborate and make them feel heard (the judge stressed these words). (Mum and brother) have demonstrated throughout …..and Mr Caulfield confirmed ….what loving people they are …(JC) has had a lot of trauma and, it may not be appropriate for me to say, but so have (mum and brother) …. Hopefully the Working Together Agreement and CCTV protocol, by doing what it says on the tin, may restore hopes for (mum and brother)… There can be no doubt that (Mum and brother) are not going away (the judge said loudly and firmly, looking at the public body staff sitting at the back of the courtroom) …. Mediation is a fresh platform …. I’m grateful to you both.” (looking at mum and brother).
But the care provider that I can’t name will remain responsible for JC’s care for the foreseeable future. There is no other current option. Many people would find this shocking, I imagine. Nobody has been held accountable for the abuse, apart from the carers who are no longer caring for JC because they have been suspended or dismissed. And JC’s mum and brother haven’t received an apology for what happened, either from the public bodies or the care providers, as many fair-minded people might think would be the decent thing to do given the circumstances. I saw a family fighting to ensure the best care and environment for their son and brother going forward and a family making compromises to ensure that “trust” – a word used, according to my notes, at least 22 times in this hearing – can be re-established.
I observed this hearing, COP 12683557, in person in Manchester. It was listed to last for three days, from 10th – 12th November 2025, but in the event, for reasons that will become clear, and to the family’s dismay, the hearing was over by 1pm on the second day. On the first day, I sat at the back of the courtroom with a journalist who is interested in this case. She has got to know JC’s mum and brother very well. I learnt that she had observed an earlier hearing that I tried to observe remotely but couldn’t, because the court didn’t provide a link.
It was at that previous hearing, in July 2025, that the Transparency Order (TO) was amended to include restrictions on naming the LA and ICB. This new restriction also means that I can’t cross-reference two previous published judgments in the case or make any explicit connection between those previous judgments and the way the case has evolved over the years. The Position Statement from JC’s Litigation Friend, the Official Solicitor, refers to “…a long and complex history; there are historic and seminal judgments…about JC’s mistreatment and unlawful behaviour of statutory bodies……To a degree, and by way of an observation, the severity of those historic concerns may have caused the family members to continue to mistrust the statutory bodies and care providers”. To provide context to the issues of trust, the LA now is the same LA as in those historic court proceedings (proceedings which are already in the public domain).
The court’s decision to ban me from referring to the previously published judgments poses a very significant obstacle to transparency: it’s a serious infringement on my Article 10 rights to report, and the public’s right to understand, this case in the context of what has previously been reported about this family in Court of Protection proceedings. The effect of the TO is to sever this hearing from the previous proceedings.
I was going to write a fairly short blog post, briefly outlining the hearing. But as I started to write it, I realised that in order to do justice to the hearing, the process and the outcome, I need to describe in detail what happened. This has therefore turned into a very long blog post. I’ve tried to report what people said, typing as quickly as I could. But my notes won’t be entirely accurate as I don’t touch type or use shorthand. I believe the value of approaching the blog in this forensic way is that it shows not only how a Court of Protection judge tried to deal with a situation where her hands are tied, legally, by the absence of options, but also to try to give a flavour of what it was like for the family involved, who had no legal representation and took part as litigants in person. I don’t know whether the journalist will find a way to report on the hearing; the press often want to use names in their reporting and the reporting restrictions in this case are extensive. I think it’s important that there is a record of what happened, and the issues it highlights – that’s why this blog is so long.
I asked Gill Loomes-Quinn[2] to read a draft copy of this blog, to get her perspective. She believes that this hearing is an archetypal case raising two fundamental issues with which the COP is routinely faced: (1) Limitation to “what’s on the table” and the relative impotence of the judge in the formulation of ‘best interests’ decisions where resource implications are engaged (the key authority is N v ACCG & Ors[2017] UKSC 22); and (2) The ‘David and Goliath’ character of the position of litigants in person – especially when these are family members versus public bodies.
After reporting the hearing, I’ll reflect on six aspects: what makes where we live a “home”; establishing a standard of care; the value of an experienced Independent Social Worker; the courtroom environment; judicial review and finally, power.
The Hearing 10th – 11th November 2025
Day 1 – Monday 10th November
The start of the hearing
This was a final hearing, originally listed for three days, so that the judge could hear evidence and make a decision as to what residence and care would be in JC’s best interests. Very early on, though, it became clear that there was going to be a change to that plan.
The listing for the first day, 10th November 2025, appeared like this:
You’ll notice that I’ve had to redact the public listing. That’s because the publicly available listing included the name of the LA, which I’m not allowed to name. It states that the hearing was about where JC should live and authorising his deprivation of liberty. But any possibility of JC moving from his home was only very briefly touched on. The hearing ended up being about a final order authorising JC’s Deprivation of Liberty, a CCTV protocol and a Working Together Agreement. A primary focus for the judge became the issue of re-establishing trust between the family, the public bodies and the care provider.
Those of us who were waiting in the waiting room, including JC’s mum and brother, were shown into the courtroom at 10.40, some 40 minutes after the scheduled start. The judge was already sitting at her bench. But there was a problem as some of the legal team weren’t there, due to a massive queue to enter the building and go through security, because of enhanced security checks (I’d had to wait 30 minutes myself and even had to open my laptop at security). As we waited, the preliminary discussion was whether the judge was going to view the CCTV footage. She eventually agreed to view two incidents during her lunchbreak and the hearing then turned to the substantive issues. By this time, everyone who was due to be in court had arrived. I noticed four females enter and sit on the backrow of the courtroom, alongside the journalist and me. I realised later that these women were from the ICB and LA. Somebody else pulled up a chair from the benches and sat on the far right – this was Mark Caulfield, the ISW. The courtroom was small; apart from the judge’s bench and a clerk’s bench in front of her (which was unoccupied) there were two wooden benches where the legal teams sat and a row of chairs at the back.
There was no opening summary or introductions so I had to figure out quickly who was who and what was going on, as best I could. Adam Fullwood was representing the ICB and LA (so he was wearing two hats) and behind him were two instructing solicitors. Sam Karim KC, of Kings Chambers, was representing JC via his Litigation Friend, the Official Solicitor. (For simplicity, I will refer to him as Counsel for JC). A representative from his instructing solicitor was seated behind him. JC’s mum and brother were on the right of the front bench. The judge, as is common for District Judges, had no court staff to support her in the courtroom. She rang staff outside the courtroom during the hearing, when she needed something, such as asking for water for JC’s brother.
No available options
Attention immediately turned to available options for JC’s care. The only option for commissioning by the LA and ICB was from the care providers already providing JC’s care. Counsel for the applicants put it this way: “You’ve got to grasp the nettle of what you’ve got”. JC’s mum and brother struggled to understand this. They’d thought that, after hearing evidence, the judge would make a decision about whether JC’s care should be transferred to another provider, but as the judge said: “I can only work within those confines”. The judge can’t order public bodies to commission an alternative provider if it isn’t an option on the table. The question arose as to whether the hearing needed to last for three days, and whether all the witnesses should be called, if there was only one outcome possible.
Mum stated that the family wanted the current care provider removed and an Individual Service Fund (ISF)[3] arrangement put in place, with new care providers, rather than being commissioned by the LA, who she said she had “battled with” for 20 years. The LA was committing only to a review of whether an ISF was possible, with a decision by February 2026. The judge said she was “sorry to butt in” and that she was “clear of your position but it is a matter of law and I can’t change….. do you both understand it’s not an option?..…I can only as a matter of law deal with what’s available”. I thought her tone was like the firm tone I used to use as a teacher, when a class discussion needed to move on.
A very short while later, her tone changed dramatically. The judge said to JC’s brother “I’m going to take my judge hat off and ask you personally – are you ok?” The courtroom was exceedingly hot and it became apparent that JC’s brother was feeling ill. The hearing was clearly taking its toll on both JC’s mum and brother. Mum became tearful. She mentioned “abuse” and JC’s brother said, “We know what decent care is and we know what abuse is …sorry judge”. The judge then said “I can see how you are looking and it is a useful reminder for me how this is affecting the family, but my focus is solely on JC.” Mum replied: “We see a paucity of care; it’s not care, it’s provision”. The judge referred to her case management powers and said she was deviating from the court timetable. She said she was worried about a three-day probing process on the family, and the impact on them of this, if the outcome was effectively pre-determined and nothing was going to change. She did say that “people have been suspended and people have been dismissed” but also that “this is only option and is in JC’s best interests that everybody works together.”
She continued, speaking to JC’s mum: “You are a fierce advocate …. I cannot change (the care provider)…I can only change where we go from here ….if I can help today (she stressed) I’m going to be very straight with you; I can’t change mindsets. But the trauma it’s causing you….…three days of court time…..I’ve probed and I’ve considered …that’s what’s going to happen.” She then reflected on whether she should “rise” for a few minutes, to see what could be done with the judge’s “input” – she said she was exercising creative case management. Mediation was mentioned.[4] The judge did add that there was no pressure on the family to agree to the suggestion of a shortened hearing, as there were three days of court time allocated. It was clear to me, though, that the judge really didn’t envisage a three-day hearing anymore.
At that point Counsel for the applicants stood up. He suggested “one further go” at a way forward to see “if any good can come out of this for JC”. He proposed a ‘Working Together Agreement”, later referred to simply as a WTA. The family being “encouraged” (some might say, including me, “pressured”) to move forward from the past was a key feature of this hearing, for the public bodies and the judge.
As there were not going to be decisions about care, remaining issues for the court were the proposed CCTV protocol, the Working Together Agreement and mediation.
The CCTV Protocol: involvement of family
The judge left the courtroom at 11.25, so about 45 minutes after the hearing had started. I noticed Counsel for JC going up to the family and letting them know that they could leave their belongings in the courtroom. We were called back in at 12pm and the judge was already sitting at her bench. I saw her smile at the family as they came in.
Counsel for the applicants addressed the court first. He referred to the working together agreement and raised the “utility” of a fact-finding hearing[5] to establish what had happened in the past – but he argued that wouldn’t be in JC’s best interests: “there is no utility in doing that” and suggested setting out a framework going forward.
Counsel representing JC then made his submissions. He said that he had had a conversation with the ISW and their view was that it would be good to have a conversation with JC’s mum and brother to discuss the benefits of mediation …”regarding care and residence, it is in JC’s best interests to remain there, there is no other option ….even if we have three days of hearings.” He stated that a working together agreement “seems to be agreed” (as a way forward) which would outline the roles and responsibilities of family, carers and the LA. There would also be a CCTV protocol which would cover who was going to be the data controller, who would have the key to the cupboard (where the CCTV is stored, I gathered) and who should be present when the CCTV is viewed every quarter. It was the suggestion of the ISW that there should be confirmation of who has logged on to view the CCTV due to the family’s concerns.
The judge stated that the current proposal with regards to the CCTV footage going forwards was that the family would be excluded from viewing it and they would only get an outline of its contents from the people who viewed it (so from the LA I think). Those people would bring concerns to the family’s attention. This became a point of contention, however. The judge continued: the family “may say that ‘if we hadn’t seen what we have seen …’. I’m saying this for the Official Solicitor ….these are JC’s safeguards. ” The judge seemed to be suggesting that the family would not trust what they were told about the CCTV footage if they hadn’t seen it themselves.
Counsel for JC replied that “The LA have heard what you have said.”
The judge then stated “There is some force in what they (the family) say, that’s why we’ve got here. We are trying to move forward without upset and heartache. I’m trying to deal with what I think they are going to say.” Counsel for JC proposed that “the family can be there when it is viewed” subject to a protocol and the judge replied “That’s what I’m suggesting, to move forward…”
Counsel for the applicants stood up and submitted that a report would be sent to the family unless there were concerns about the standard of care, in which case the family would be told and then brought in to view the footage, so they would not be excluded. He said that mum was visiting regularly (the court had earlier been told that JC’s brother was not visiting regularly due to the distress it caused him). Counsel for the applicants argued that it was not a case of the family being excluded. He then suggested that things “…cannot proceed on the basis that (it is suggested) the care provider and public bodies are going to tamper (with the CCTV footage).” He used the word “micromanage” in terms of the court’s role. He also stated that the ISW was in court, so the court could hear directly from him.
I saw the judge rub her forehead. Addressing the family, she said “I’m trying to find a managed way here …I adjourned for 30 minutes so you could get some fresh air and understand what is happening. You’ve heard about ISF, that’s now going to be looked at, for a realistic update by February so that’s …”. JC’s brother said “progress” and the judge agreed. She then said “We have to have something in place for the CCTV protocol”.
A Working Together Agreement
Mum then spoke. She said it was “a step forward. With regards to the Working Together Agreement, she said “We’ve always tried to work together. We have viewed horrendous, despicable footage” and some staff are still there (caring for JC).
The judge then asked mum how she thought a working together agreement would work. Mum said that she would try and work together. But she was worried. She told the court she has taken “an audio recording in to try and protect myself.” She explained: “I’m an older woman…..there are three six-foot-tall guys…it shouldn’t be like that …it’s JC’s home ….it shouldn’t be like that ….”. She indicated she felt intimidated. Mum is in her late sixties.
JC’s mum continued, saying that there is a female carer (whom I will give the pseudonym Mary) that she trusts and who was due to give evidence. She is a “whistle-blower” and should be protected, according to JC’s mum. Mum was concerned Mary would be laid off by the care providers for being a “whistle-blower”. About the proposal to exclude family from viewing future CCTV footage, she said “Our concern is that they will determine what is abuse ….I don’t trust the social worker to identify what is abuse.”
The judge summarised: “So, to break it down, you are going to work with…” (the carers) and mum replied: “I’ve always been polite.”
The judge then gave her views on the CCTV protocol, taking into account the two reports written by the ISW. She thought it was important the family were involved. She said, “I can’t build trust on your behalf” and “I can’t give you the gift of trust.”
She continued: “I’m trying to be neutral but ……….the CCTV is going to remain in place, it is part of JC’s life to protect him …and if things happen, you are going to be told and will see it …and for your worries and concerns that it will be tampered with or removed, I will speak further to (counsel for the applicants) and I’m satisfied that there is a safe mechanism. That’s the best I can do, isn’t it?”
Mum replied that it was about safeguarding JC.
At this point, Counsel for the applicant made a new proposal. He suggested that an independent IMCA[6] be appointed by the LA, who would be present at the CCTV viewing, and who would be “really independent.” The judge found that “helpful” and added that “the IMCA will be there on behalf of JC on a long-term basis.” JC’s brother said that it was a way forward.
The judge then moved to the subject of “Mary”. She addressed Counsel for the applicants:
“….Mr Fullwood, it may be out with my jurisdiction …I was (told about Mary) …I’m treading carefully but being open ….she (Mary) has a great attachment to JC, because she was going to come to court …she might feel some sort of employment risk or intimidation…I’m choosing my words carefully …out with my jurisdiction …..”.
Counsel for the applicants replied that “She is an employee of (care provider)… I have no evidence she’s been threatened in any way …judge can check …she would have come to court …but we don’t understand there is any impediment to her coming to court …it is a serious allegation to make ..she is not an employee of the LA.”
Dogs
The judge then brought up the subject of dogs. “I know I shouldn’t micro manage, but I may have to be practical in my role today…mum has two dogs and I have read in the witness statements that JC likes dogs …I’ve read that some staff don’t feel comfortable with dogs ….I’m not interested in their comfort ….If JC likes dogs …..”
Counsel for the applicants stated that these were “large dogs potentially running amok in a property” and making a mess. “We are hearing from the care provider that this is a problem, and the dogs are not being controlled as they should be” and that wasn’t to the benefit of JC. The judge replied, “I am not making findings….the dogs are retrievers (mum confirms they are two labradors, so hardly XL Bullies, I think to myself) and if JC wants to see those dogs he should be allowed to.”
Counsel for the applicant responded, “I take the court’s point ..as much as can be done, should be.” And the judge replied, “That’s all I’m asking for.”
There is case law about dogs and people who lack capacity. According to Ian Brownhill, the most famous dog in the Court of Protection is “Bobby the Dog”: (Mrs P v Rochdale Borough Council & Others, [2016] EWCOP B1). Ian says in a webinar[7] that the judge in that case was “clearly an animal lover” and she recognised the importance of pets to people who lack capacity. Paragraph 29 from the judgment reads as follows: “It may seem to those not well rehearsed in the needs of a person who owns a pet, in this case a person who no longer has capacity to make decisions about various matters, what the importance of a pet is in their life. The deputy only has to read any single reference in reports, assessments or statements of Mrs P of how important Bobby is to her. Her Social Worker says in her witness statement to the court that:- “I would recommend that of single most importance in her life is her dog and having some form of contact with her dog in the future if possible.” The judge in that case? It was DJ Matharu!
The judge continued. She said “The IMCA is a useful tool” which she was sure the Official Solicitor would support. “Mr Karim, there has been progress on the Working Together report, the CCTV protocol will be refined….have I overlooked anything on behalf of JC?”
Counsel for JC outlined some issues to be clarified and then moved to mediation: “It seems on behalf of the Official Solicitor that the recommendation made by the ISW is a good one ..JC has complex needs ….and (has been) looked at by the court for 15 years ….perhaps (we can) find a way in which the public bodies and family can work together on behalf of JC’s best interests.”
The judge asked more about mediation, whether it would be now or in the future and Counsel for JC replied something about depending on a “change of commission and provider…. ..mediation ..if there have been mistakes…” at which the judge cut in and said:
“You are being polite – there have been mistakes.” (Judge’s emphasis).
The judge then summarised the position, addressing the family:
“I don’t want you to think that I don’t want the three days (for the hearing)…I don’t have the jurisdiction to (give you what you want ) ….I’m not removing responsibility for either of you but somebody independent (the IMCA would become involved) …you heard what I said about Mary, and the dogs …..I can ask you, but I can’t compel you,…. but mediation would be something …I think it can be a very good thing …looking again at the notes I took…this is not a criticism or berating you, but when you’ve been through everything….. when you are saying what you feel…”
My reading was that the judge didn’t want to put the family through what she saw as a demanding process for them if there would be no change of care provider, and she was trying to work through what could be achieved.
Mum replied. She said that friendships are so important for JC, the care is rigid…it does not allow for flexibility and friendship: “He’s living in his own home, it’s got to be a home …(they, the care provider) are trying to treat JC’s home like another supported living place ..it’s his own home …he has human rights, to develop a friendship ..there is no creativity (re care)”.
The judge had her hand resting on her jaw as she looked at JC’s mum and brother, listening intently.
JC’s brother said the carers were systematically removing…..and encroaching….removing things he loves …the care providers had goalposts but (they) have moved back, to restrict his life.
Hearing the views of the Independent Social Worker
The judge then made a proposal. She suggested asking the ISW to give his views, to comment and “tell me what this judge should do.” About the CCTV protocol, for example.
Counsel for the applicants said he agreed with the judge’s proposal to hear from the ISW but that family wanting to view the CCTV footage “……has come back to a lack of trust.”
I heard mum sigh loudly.
The judge said to the family “I need to hear from somebody independent, to you, to (the LA)…. I want to try to future-proof JC’s care. That applies to everybody, the two of you, the two of me (by which I think she means the OS and her) and the LA” (raising her voice).
The ISW went to the witness box and was sworn in by the judge, as she had no clerk.
The judge stated that it had been “a curious route” for him to be in the witness box. She continued: “You have heard heartfelt views (from the family about JC’s care) ….the hurt they feel on JC’s behalf …you’ve viewed the footage, met the family …the reason I have put you in the witness box is to understand why a new approach from everybody is required and how that can be workable ….I’ve been involved with the family for a number of years …”.
The ISW said he will do his best to assist the court. The judge asked him about the appointment of an IMCA and he thought that was an excellent idea which will enable a “greater degree of accountability and transparency.” The judge stated that it takes “transparency to build trust” and asked “How does one build trust in this sort of situation?”
The ISW said that the family hadn’t been invited to meetings and that “happens with the Court of Protection….I have no vested interest.. the family are the most dedicated I’ve ever come across …I have met professionals who want the same …I worry ..not worry …I’m trying to choose my words carefully …the difference between professionals and the family …they have different views about how to achieve goals but all want the same goal …I didn’t get a sense that nobody didn’t want that”. That’s why he suggested mediation and talked about “some slack in the system”. He thought the situation was more rigid but “solutions have been found …sorry judge, I don’t want to ramble…but I think they had a degree of faith in my independence and, I might be wrong, but in your independence.”
The judge then said that she may be “putting a label on it but – are we at make or break?”
The ISW replied “Regardless of what happens today, things are going to change in JC’s care, but when people (are in the same room) and can compromise, things can change.”
It was then Counsel for the applicants’ turn to ask the ISW questions. He started by saying that he was going to ask about what can be done to improve trust. He asked if it is the ISW’s professional view that a Working Together Agreement can improve relationships and the ISW replied yes, if it’s adhered to. Counsel then turned to the issue of the CCTV protocol and the appointment of an IMCA. The ISW replied yes (to the suggestion of the IMCA) because of their independence, and that the suggestion has been put forward by the public body to increase accountability and transparency.
Counsel for the applicants then turned to mediation: “Can you say why, and be clear to the court, why it would be a benefit for (mum and brother)?”
The ISW replied that the family “have a long history of not being listened to” and that he understood their position. “But you never know what is going to happen until you get in that room…impartial person in the room…and mum and brother would say they want a social worker they can have trust in, that would be their ultimate goal..”
Counsel for the applicants then stated that the LA is “inviting the court to make an order that JC will receive care provided by (current care provider)” and what the ISW’s view was on whether they can meet JC’s needs. The ISW replied that there is a “disparity in terms of evidence and degree of certainty” but he “is satisfied the care plans will meet JC’s needs for the next 12 months.”
Counsel for JC via the OS asked the ISW about the CCTV protocol, and the advantages and disadvantages of the family being present when the CCTV footage is viewed. The ISW replied that there was the advantage of the family not being there in that there would be no “interference”. But there would be a disadvantage too. The family know JC particularly well, including his “…idiosyncrasies”. JC shows distress that the family can identify that the professionals wouldn’t spot (even if there was lack of agreement about what is abuse or not). Counsel for JC then stated that a disadvantage of them being present would be exacerbating a lack of trust. The ISW responded by saying that there was a possibility of increasing conflict when viewing (together) but it may be a way of developing relationships. “I did not specifically explore that with the LA (viewing with family present) ..but I support family being present…if It’s a regular review I don’t anticipate it being a challenge”. Counsel for JC asked if a quarterly review would be ok and the ISW replied “yes, if concerns are dealt with judiciously”. He mentioned “activities”, “faeces” and “urine”.
Counsel for JC then asked the ISW: “Are JC’s needs being met in current placement?” and the reply from the ISW was “yes”. “And in the future, if there were to be a change of provider, what would you recommend regarding better relationships between family and professionals?” The ISW mentioned co-working and involvement of the family, hence the suggestion of ISF. “Mum and brother don’t feel listened to……there are polarised views on care and I see that continuing (without a change of provider)”. But he said that he has seen some improvements. He said “Concerns were raised in 2023, 2024…difficult to make argument that care needs are being met ..but to provide balance, I am satisfied…. finely balanced on the basis of probabilities, that JC’s needs are being met …..the family have greater control and the ICB and LA can ensure that JC’s needs are being met.”
There was a brief exchange about how contact between JC and his brother could be facilitated and the discussion turned back to mediation as a way of improving relationships. The ISW said “When people have concerns about care …especially as a social worker, I have seen improvements even with the same providers.”
The judge then asked mum if she had anything to say.
Mum asked the judge if she could stay sitting down. The ISW and mum smiled at each other and she called him Mark. She started talking; talking about trauma and how she feels the need for a new start ..that’s why talk of ISF gave her hope……..
The judge asked her to ask the ISW a question.
Mum asked him, “How do you justify his needs are being met when he can’t go out in his car?” The ISW asked for guidance from the judge, as he was being challenged to answer something anecdotal in court. The judge replied, saying that both Counsel had asked him if the “package was meeting JC’s care needs, and mum is saying that they don’t; she doesn’t understand how you could say that, in the round, if he doesn’t have access to a car.”
The ISW replied by saying that there are always occasions when there are absences (of a driver)…mum and brother are saying that it is endemic and if that is the case, then that is a significant part of his care …”and when I spoke to the care provider, they said a car was a part of his routine and P used (going out in the car) for self-regulating …P can’t access the community any other way, so a driver is a significant part of his care plan…but the absence (of a driver) would need to be systematic.”
Mum mentioned about looking at the car through the “lens of P’s care” and the judge said she would deal with it.
Mum carried on. She said that ISF would be a fresh start. But I could see that she was finding it hard to speak. “..I want to clarify ..sorry judge, I had so many questions …trying to put a question .. Catalyst provider ..I want it clarified who Skills for Care really is … I’m sorry judge, I’m not phrasing properly “. The judge asked mum to pause and addressed the ISW: “The LA have said they are going to look into it. So, if they have “got the wrong end of the stick”, if I can put it like that … that would come out in the wash, wouldn’t it?
The ISW replied “Yes.”
The judge continued, saying that the LA say they will come back by Feb…as an interim stage, they will do their homework (about the possibility of ISF).
Mum then said: “I’m not a lawyer, I’m just a mum …care isn’t about being perfect, it’s about being good.”
The judge summarised her position. “What I’m trying to do is provide some progress with the only tools I am given …I asked the ISW to provide evidence about building trust up …Mr Fullwood, you are going to have to take instructions on this…I am minded to direct, so far as I am able, mediation …it is not an arbitrary, nebulous concept …I’m going to be prescriptive ….about who should be there, otherwise it is not going to work, and perhaps an agenda of sorts , using what Mr Caulfield has had to say …to next mediation meetings and achievable targets ….first item is P’s car…difficulties with agency workers … I’m not asking the ISW to deal with (all the issues in his report …(my aim) is to try and see how we can work together going forward.”
A leap of faith
The judge accepted that the morning had not proceeded in the way the plan for the hearing had been put together but she said she was trying to work towards “a new start and provide the engagement of everybody”.
She then addressed the family. She said I have to (express myself) myself in legal language even though you aren’t represented …..”mediation requires a leap of faith …the LA are going to provide (the means) but it also requires the two of you …what does “leap of faith” mean? It means going in with an open mind … I can only direct it, if you two will give it a go.”
The judge was asking the family to agree to mediation and to consider it over lunch. The judge reiterated the view of the ISW, after a comment by mum about hearing more evidence (I think): “He has said this is not the best (care provider) but it’s all we have … at this moment in time, these are the only care staff available …so I can probe, but it is the only care team available.”(judge’s emphasis)
The judge also wanted mum to understand that, by offering the appointment of an IMCA, the LA were also making a compromise, after mum stated that the family have compromised, and are willing to compromise in the future.
At that point, at 1.30pm, the court rose for an hour.
Discussions between the parties took place before everyone came back into court. The Local Authority proposed one organisation to act as mediators and the judge wanted to find out what the family thought. She said again: “I can’t compel mediation …are you prepared …to explore (mediation) …to take a “leap of faith?” JC ‘s brother replied yes, although “it’s going to be hard for us, (this) has taken its toll on us.”
The judge replied, “We aren’t going to leapfrog into …(there are) certain tweaks I want to make …but the fact that you are prepared to give it a go is a great thing for me.”
Making a decision about who views future CCTV footage
The judge then suggested to Counsel for the applicants that there was something he might want to seek instruction on; the ISW has said that he doesn’t see why the family can’t be at the CCTV footage reviews.
Counsel for the applicants said that he didn’t have a chance to question the ISW on that, but the purpose was safeguarding and that’s the LA’s responsibility and not the family; “Mum says she just wants to be a mum ….there are practicalities …..it could make relationships worse …but can I say this? If you decide this is what should happen or give an indication…..”
The judge replied: “I have to tread carefully …if I give indications….”. Counsel for the applicants suggested that she could ask the OS what her view was. The judge replied “I’m trying to do this collaboratively …do you want to ask the ISW?”
To this suggestion, Counsel for the applicant said that the ISW (looking at him) “would say the responsibility is the public body and he is nodding …..but if the OS has a clear recommendation, I will take that into account.”
As Counsel for the OS doesn’t have instructions on that particular point, his solicitor leaves the court to find out what the instructions would be.
The Judge then made a decision. “I haven’t made findings because of the possibility of making a rift bigger” and she doesn’t want to set things up to fail … “when I look at the expectations… it might it be advisable not to have the manager (who was named[9]), but a client manager trying to manage the new relationship…”.
Counsel for the applicants said: “We can make enquiries …(the named manager) would be the obvious choice.” He said the concern was that the LA could come up with somebody else who would be opposed (by the family).
The judge said, “If we could do that today, that would be very helpful”. She then talked to the family and asked them if they could suggest anybody ….the family suggested a compliance officer who they have some faith in.
The judge recognised that she was micromanaging, “which people say isn’t the role of the court, but some cases demand it, and this is one of them”.
Counsel for the applicants referred to the “WTA” and the judge stated that she was trying to find somebody the family could trust to be a client manager. Counsel for the applicant asserted that the “key is communication …the mediation process starts with building blocks, so the focus could be how to improve communication with everybody …to avoid “misunderstandings” and the judge responded by saying she agreed with “incremental improvement.”
The judge said, “ I hate this expression but a “meet and greet of the IMCA”, part of WTA, Working Together Agreement, such as a rota of activities, because that is such a big thing. And part of that is JC and his car” so there would be …”achievable markers”.
Counsel for the applicants stated that the “…background needs to be disclosed (to the IMCA) but not enough to colour the chances of success.” The judge agreed that everyone needed to be concerned about JC’s privacy.” She asked the family if they understood what was happening at the moment. Mum started speaking ….. “I think an apology is in order ..but enough is enough, I want to move forward, it is sad where it has got to, but we are ready to move on.”
The judge thanked the ISW: “Your input has been very useful; you have seen the fruits (of your work).”
The ISW replied: “For me, what would assist, as an addition to the formal mediation, are friends and family in the community being part of JC’s life, managers coming together with family ….greater (care provider) presence …having a JC day, training days, using expertise about the best ways to work with JC – that seems to have been lost in this conflict …a training day, with an independent facilitator to input into a PBS[10] process, an undertaking from mum and brother….part of mediation.. if I’m allowed to say this, the local authority won’t fund mediation indefinitely and there are meetings that mum and brother should be a central part of …I realise this is disputed but with (previous carers), there was a relationship, and the best care packages (have good relationships) as long as they are within boundaries and professional guidance.”
Counsel for the applicant responded, “I don’t think anybody would disagree with what you’ve said.” He asked the ISW to confirm that mediation would give greater reassurance that the package of care was in JC’s best interests. The ISW confirmed his view that it would.
Counsel for the applicants continued, asking about the family sitting in on future CCTV viewings: “Would you agree that (viewing CCTV) is to review the quality of care and that is the responsibility of the LA …and there are consequences if the family sit in?”
The ISW responded that it was a challenge “…and I don’t think I said this as a disadvantage …but there has to be a framework …for example, if mum raises a concern and it is not reviewed…it would need to be triangulated (evidence) …(it’s about) building trust and transparency, as long as it does not interfere……”
Counsel for the applicants responded by saying that one of the difficulties was about building trust, and is it an indication that the family don’t trust (the process) if they are there …what if an independent IMCA is there?
The ISW replied that it “is a compromise ….and subject to review”. I notice that the judge isn’t writing notes at this point but is looking at the ISW as he’s speaking.
Counsel for the applicants stated that the court was still awaiting instructions from the OS, but was it his view that an IMCA would satisfy regarding the fairness of the system? The ISW replied “Yes”.
Counsel for JC then questioned the ISW. He asked the ISW “Is it still your view that the gold standard is family involvement and, in their absence, an IMCA is an acceptable option”, which the ISW confirmed was his view.
Counsel for JC then asked the ISW about mediation and the family viewing CCTV. He took his time to answer. His reply was “I don’t think it is a prerequisite to mediation, but it would be helpful (to provide trust) – I think – CCTV being available.”
The judge then asked the ISW: “I think there is a risk of a degree of separation if the family aren’t involved (in viewing CCTV)?”
The ISW replied yes, but it depended on the challenges of family being present …”.it is difficult to say, judge …everyone on an equal footing ..steps should be made to allow family input”
The judge continued. And the independent IMCA, it is going to take some time for that trust to be established between the family and the IMCA? The ISW agreed.
The judge went further: If they never get to see what their son and brother (is doing) ….“How do you think that fits in with this degree of trust we are trying to build?”. The ISW replied, stating that a different contact for them within the care provider, somebody they had more trust in, would help negate them not being there to view the CCTV footage.
The judge observed: “So some creative thinking…….but that would still be your preferred option?”
The ISW replied “Mum goes in every single day; no professional has that degree of contact …and sometimes what she observes doesn’t tally with what she hears, so it is difficult to square the circle, and I would be the same ….so for example, concerns have arisen because mum has seen faeces and urine, and she doesn’t trust the staff, because they haven’t always been accurate …..and that’s why my preferred option is 1) family and 2) IMCA.”
The judge turned to the family and asked if there was anything that arose from the questions she’d asked the ISW, or that they thought she hadn’t asked. JC’s brother replied no and said that the questions had been “poignant.” Mum added that there was a duty of candour, that she wanted openness and transparency and that she wanted to move forward.
Counsel for the applicants then spoke, saying “In the spirit of being candid, and on behalf of my client, people being there is not to find fault”, and he raises “practical arrangements”. (He refers to practical difficulties which arose to do with the ISW viewing the previous CCTV footage). He suggested that the data controller gave everybody 4 weeks’ notice of the review of the CCTV footage.
The judge asked “And you are proposing that this meeting is everybody?”
Counsel for the applicants replied: “I’ve made my submissions on behalf of my two clients …I’m trying to anticipate difficulties …it’s a small point but can be an important point”. He mentioned …”4 weeks’ notice” and that it doesn’t have to be both family members, for example JC’s brother has work commitments.
At this point, Counsel for JC informed the court that the OS supported, for transparency and good working relationships, that either JC’s brother or mum should be there (to review the CCTV) in JC’s best interests.
The judge then turned to the family, and said: “You’ve heard, one or other of you must be able to attend and if perhaps if one or other of you couldn’t make it”….(the IMCA could be there). The family agreed. Counsel for the applicants then stated that perhaps the IMCA should be there for every meeting and there was a discussion as to who should be there for the care provider, and the judge stated that the detail needed to be pulled together and used the term “least worst option”. She brought the discussion to a close, saying “that deals with the CCTV protocol and the WTA client manager”.
Agreeing the Court Order
The judge’s attention moved to the court order. She suggested a 6 month for a review of the Deprivation of Liberty authorisation “and to see how it’s going. You’re going to say the court doesn’t have the authority……but a review earlier than 12 months might be better.” The judge was giving a clear indication that she wanted a review after 6 months. After the instructing solicitor looked at the people from the public bodies, Counsel for the applicants agreed on 6 months. The judge explained to the family that judges can’t “hang onto cases” if a final order is issued and she suggested a 6-month review was possible and if all is going well, she thought that they could have a hearing “on the papers”, that is, without anybody attending.
The judge then goes through the detail of the order, the family are asked to look at the website of the organisation the LA will fund for mediation, to make sure they don’t have any objections. After the judge went through the detail of the order, at a little before 4pm, the judge rose. Counsel for the applicant had to draft the agreed order. The plan was that the order would be approved the same day.
But mum was still thinking about the process. After about half an hour, we went back into the courtroom. Mum had spoken to Counsel for JC during the break. She still wants Mary to give evidence. Mum asked the judge: “What’s your advice? I’m not a lawyer.”
The judge replied: “I can’t give advice ….a 3 day final hearing was listed, so that I could explore and probe what care JC was receiving …and to explore that, you were going to call witnesses and I was going to spend 3 days exploring …and Mr Fullwood said, to help people who weren’t represented, he said that you can explore but there is no other option …the evidence is in the bundle ….but there won’t be cross examination ….there are things that need improvement …I aired worries about Mary in open court …but as to what happens to her evidence, I don’t hear from them, but I have read their evidence …3 days of challenges to you and the care company, when the outcome is going to be exactly the same. We are trying to have a different way ahead …would that have been the same after 3 days of acrimony and resentment on both sides? …I have no jurisdiction to change the care team …I could have said that I’ve looked at the video and Mr Caulfield has looked at the videos …..and they accept that there does need to be a different approach, a different programme of care, and of you not being made to feel welcome and treading on egg shells …what is that going to achieve when I can’t change anything? …What I’m hoping for, with this collaborative approach …I’ve never seen JC’s brother look so ill….I’m weighing up, and that’s not my role, what is the best outcome for JC, because I can’t remove the care company …..we move two steps forward and fifteen steps backwards ..We have a document that works for everything …I just want what’s best for JC …..what would (witnesses) have achieved? I’m looking for a period of time when, in 6 months’ time ….so for people who aren’t represented, does that provide any clarity?”
JC’s brother confirmed that it had. JC’s mum said that they needed to read the order. The judge said that she would print the order when it was ready so they could read it. We left the courtroom again. My impression is that the court’s preference was for the family to agree to the order and accompanying documents (the CCTV Protocol and the WTA) before the end of the day, so nobody would have to return the next day.
The lawyers spent time drafting the order in a consultation room as the rest of us, including JC’s mum and brother, waited in the waiting area. We were called back in at 5pm. Counsel for the applicants had emailed the order to the judge, and she left the courtroom to print it out.
My notes at this point record: I wonder why the barristers can’t explain it to the family as we are waiting ….we are all sitting in silence now. It feels like a very long day.
The judge came back with the printed papers, and we all left the courtroom again. JC’s mum and brother went into a consultation room to read them. Counsel for JC joined them. At 5.30pm we headed back into the courtroom. JC’s mum and brother look very tired.
JC’s brother told the judge that “Sam (Karim) has politely talked us through the order”. But the family were not happy with the wording of the Working Together Agreement. They felt that the wording was slanted against the family, and the judge said she also had some concerns. She added “It’s been a long day and I’m sorry”. JC’s brother said that if they are moving forward and building trust, the way the document is phrased (raises issues). The judge said that it was “not based on any findings….but there are a couple of tweaks I want to make (too).” It was agreed that the parties would arrive for further discussions at 9.30am the next day, with the second day of the hearing due to start at 10.30am.
The judge thanked the family, and the hearing was finished for the day. It was approaching 6pm and Manchester Civil Justice Centre was virtually empty as we all left.
Day 2 Tuesday 11th November
Initial discussions
The next day, we were called into the courtroom at 10.45 and the judge was already sitting at her bench. Counsel for the applicants had his two instructing solicitors again and today there are three rather than four ladies from the public bodies sitting in the back row. Counsel for JC is accompanied by his instructing solicitor. JC’s mum and brother are on the front row. I sit on the back row behind them. Today neither the ISW nor the journalist are there. The journalist had told me the previous day that she couldn’t be there as she had other commitments.
Counsel for the applicants told the judge that the parties “have been busy”. The draft order was agreed but there were issues with the Working Together Agreement. He thought, being optimistic, that they needed 20 minutes more. The judge asked the family if they wanted her to deal with the CCTV protocol then, but JC’s brother says they wanted everything to be dealt with in one go.
Counsel for JC told the court that the Official Solicitor was neutral on the WTA and that it was not drafted in a way that was implying that a party had “done something”. The judge wanted “everyone treated the same way.” She suggested that in the preamble to the WTA, it was written that the recorded provisions “are not based on findings or culpability on any findings” because I haven’t made any comments …I don’t want to use word appease…”. JC’s brother suggested the word “alleviate” and the judge thanked him. Counsel for the applicants then suggested a form of words but was speaking so quickly I couldn’t note them. The judge liked the wording and said it was “clearer and more precise”.
The judge then stated “for openness, the journalist approached me yesterday to ask for the approved order…….she’s not here today”
Counsel for the applicants then said something about “yesterday’s news” and smiling, he looked at the public bodies staff sitting behind him on the back row. The judge smiled too.
JC’s mum asked if some evidence from JC’s two GPs could be considered (they had sent her an email overnight). Counsel for the applicants said he thought they had looked at all the evidence and were “looking forward to the future.” Mum replied that it was looking forward. The GPs wanted to put forward to the court how important it is for JC to have the family as advocates in his life. The GPs have known JC since he was 4. The judge asked whether the GPs are supporting family involvement and mum replied that it’s about the best model of care that JC should be receiving from a clinical, emotional and social level, and she is confused about why they (the GPs) have not been brought in and their advice not sought. The judge asked if it is a medical issue and mum replies that it is a holistic issue…they are writing it in the best interests of JC. They sent it in an email to her as “he doesn’t know how to submit (it), I just got it last night, it is not supporting the family, it’s to give a view of the medics of what’s best for JC.”
Counsel for JC stated that it “might be best to see it” and the judge agreed. Counsel for the applicants said that he couldn’t say anything until he has seen it. The judge commented that she didn’t know what impact it would have on the Working Together Agreement.
We left the courtroom again at 10.55, so that the parties could have further discussions. We are called back in at 11.45.
Working Together Agreement – Back to the dogs, and “items”
Counsel for the applicants told the court that there is “good news and bad news.” The parties had agreed the order and the CCTV protocol. They had agreed everything in the WTA except one substantive issue (the dogs having access to the paddling pool in the garden) and one clarification (about bringing items into the property).
Counsel for JC stated that the paddling pool issue was a difficult one. The family say JC enjoys seeing the dogs and “My learned friend says he doesn’t enjoy it”: the Official Solicitor had “no strong view”.
The nub of the issue was that the care provider say the dogs shouldn’t go in the paddling pool because it isn’t hygenic. JC’s brother explained what happens. The dogs go into the kitchen as their main area, and they are let off their leads. They then play in the garden and will inevitably go in the paddling pool, not in the spa which is in the house. JC sometimes gets in the pool after running around without shoes on, and has played in the pool with the dogs. Mum adds that since he was a small child, his dad created a pool and he has always gone in a pool with the dogs. He has always had dogs in his life, he has been brought up with them. The family don’t want restrictions on the dogs. If the dogs aren’t allowed into the garden, they will only be allowed in the kitchen.
The judge asked about the type of pool, and JC’s mum explained that they are blow up paddling pools, he stands in them, and only his feet are in them. Counsel for the applicants said that he has heard the evidence, it is JC’s paddling pool, it is not the dogs’ paddling pool, it is not the family’s paddling pool…the staff have to make it clean and hygienic for JC…this is all focussed around JC’s needs, JC won’t go into the pool if he sees the dogs have gone in there ….we don’t understand why the emphasis is being put on the dogs when its JC’s to use; it is in the care plan.
The judge asked how burdensome it is to clean a plastic paddling pool for the care staff and Counsel for the applicants replied that it “is another job that can be avoided”. The judge added “And when you said that the evidence is that JC doesn’t enjoy the dogs as his mum and brother say …where is the evidence? Counsel for the applicants replied that it is “what I’m told. I can call the social worker …?” The judge says, “And mum will say….”. Counsel for the Applicants said that he was reporting back what the carers on the ground say. After a discussion about the nature of the pool, and a suggestion from Counsel for JC that maybe the family could clean the pool, the judge asked mum “May I ask one more question….is it onerous for you to pick up a hose pipe and clean the paddling pool?” and mum replied “Not at all.”
The judge made a decision. She was not supporting the position of the care provider: “Much of yesterday has been about working collaboratively …mum and brother need to be involved …that’s what yesterday’s hearing was about …JC will indicate if he isn’t happy ….mum and brother have been involved in JC’s life …I am not endorsing an unmanageable provision …mum needs to feel relaxed when she goes to see JC with the dogs …could make her feel tense or unhappy …and JC could sense that …..and when I’m told that it is another job can be avoided …Mr Karim suggested a compromise …mum is happy to clean it”. They all agree on the wording for the WTA about the dogs.
Counsel for the applicants then raised the issue of notice being given to replace items. He said it is “forwards looking” and is in JC’s best interests. Counsel for JC supported the amendment and agreed that not everything needed to go through a formal best interests decision. The judge asked the family what their issue was with the wording. JC’s brother explained that the wording doesn’t say furnishing and fittings, it says “’items’ ….that could be a KitKat. What if the trampoline busts or breaks, we would expect to replace that, not go through a best interests process.” The judge clarified: “You are talking about a like for like; that goes without saying.” JC’s brother replied: “I don’t think it does, judge.” The judge asked Counsel for the Applicants about the “like for like” wording and that was agreed. The judge also suggested that if new people come in, like for like applies to equipment such as sofas, bird tables or similar. The family thanked her for the clarification. The judge added that where there is disagreement, there will be a best interests decision involving the IMCA, and the family are happy about working collaboratively with the IMCA.
There is then a discussion about tidying up the agreed version of the Working Together Agreement. JC’s brother asked for a punctuation change relating to potential future carers, if an ISF model of funding is agreed after review from the Local Authority. He apologised to the judge: “Sorry, it’s a small point” to which the judge replied: “it’s not a small point.” The family confirmed that they are happy with the organisation proposed by the Local Authority for mediation.
Counsel for the Applicants then stated that proceedings were concluded even if it is a 6-month order and a COP9 would be completed if a hearing was needed. The judge said that she wanted to pick up on that: “I had my own note…I need to explain the meaning of that to brother and mum…all that I think needs to go in, Mr Fullwood, and I will explain what concluding means.”
The judge addressed the family: “Brother and mum, what that means is that as a consequence of how things have panned out yesterday and today….looking forward, for all the reasons I gave yesterday, the issues have been resolved by the court order, the WTA and the CCTV protocol …I’m trying to use words that won’t upset you…. so ‘wrapped up’; but you are concerned with ISF …that’s the only bit that is really live at the moment – home and the care provider is finished. If the ISF model is not commissioned, that is something you will have to follow up …by judicial review ..that’s an admin court.”
Ending the hearing
Counsel for the Applicants proposed that the family had approved court documents printed that they could take away with them. The judge had to arrange this herself, phoning the Court of Protection office to let them know they would be receiving some documents that they had to seal immediately, because she had unrepresented parties. She told them she would deal with printing them in her “retiring room”. The judge explained to the family that she wanted them to have the documents when they left.
As the court was waiting, Counsel for JC brought up the issue of the email from the GP. Counsel for the applicants said that he hadn’t had a chance to read it and he didn’t know what the purpose of the email was. The judge said that she would read it so that she could say she’d read “everything”. She read it. Then she addressed JC’s mum and brother: “You can relay to the GPs that I’ve read their medical overview …there is nothing new to what is in the ISW’s report …stability…family relationships are a fundamental aspect …(of JC’s) social and emotional needs …the email has been provided to the LA and it can also be provided to the care provider as part of the WTA. There is nothing there that criticises anyone.” Mum mentioned an addendum, and the use of agency staff, and “that is the concern of the GPs.”
The judge replied (after dealing with a confidentiality schedule for the order, as the order is being sent to the press): “You are putting me in a difficult position in this way – I cannot dictate or compel the care team to use certain staff or do certain tasks …however JC needs consistency …so anybody with an ounce of common sense can see that he needs stable staff …but if there are shifts, or staff are not available….would you rather nobody was there?” Mum replied “no”.
The judge continued: “Mr Caufield, his work is a very important piece of work …the GP reports don’t contradict (that) ….. it reaffirms (what’s in the ISW report)”. JC’s brother used the word “ratify”. The judge then indicated that she would be making some observations once the order had been printed.
The judge then left the courtroom to do her administration tasks and print the order. The rest of us stayed in the courtroom, waiting. At first there was silence, except for the noise of computer keyboards. It was very hot. JC’s brother drank some water and Counsel for JC suggested he step out of the room to get some fresh air. JC’s brother asked if he iwas allowed to. Counsel for JC said yes, and JC’s brother left.
At 12.40, Counsel for the applicants said to the public body staff that they could step outside to stretch their legs as he had just sent something to the judge, but they stayed in the courtroom. Counsel for the applicant started talking to his legal team, discussing hotels I think ……he said something about coming back in 6 months. At 12.43 JC’s brother came back in, and he wasn’t wearing his tie. Counsel for the applicants started talking to his solicitor about high taxpayers moving to Malta and reasons why …and talking about his children. I’m not sure he realised, but his voice carried in the small, otherwise silent courtroom. I remember thinking of the family, sitting and listening.
At 12.50 the judge came back in, gave the printed, sealed order to JC’s mum and brother (Counsel having confirmed they didn’t need hard copies) and made her closing observations, which I have already included at the start of this blog. And with those final words from the judge, the hearing ended.
Reflections
I will focus on a few key points: the meaning of “home”; establishing a standard of care; the ISW; the courtroom; the idea of judicial review; and the concept of power.
Home as a place to do as you please
For many of us “home’[11] is a space where we make personal choices about what we do and how we live. A place to be free to express our identity. To decide for ourselves about all the small and important details of our lives. This includes pets.
To anyone who doesn’t like dogs or who has never been brought up with dogs, it can be hard to understand the focus on dogs in this case. But anyone who has been brought up with dogs will understand how important they are to family life – and to providing a home rather than just a house. I’ve got two labradors myself, so I perfectly understand why JC’s mum and brother were not prepared to concede to the demands of the LA. I was pleased that the judge recognised how important allowing the dogs to access the garden was for this family. Having later learned about the Bobby the dog case, her decision is not surprising to me.
Establishing a standard of care
Highlighted in bold in §5 of the LA and ICB Position Statement are the following words, about case law they have used: “Here, the court’s task was to select the best practical outcome that was realistically available, even though all the options were, to say the least, imperfect. It was beyond the powers to eliminate risk or make A’s many problems go away.”
Mum isn’t looking for gold-plated, perfect care. She said during the hearing “Care isn’t about being perfect, it’s about being good.”
Observing this hearing does make me wonder what counts as “good care”.
The Independent Social Worker
It was clear that both the family and the public bodies recognised Mark Caulfield as an independent voice in this case. And the judge certainly valued his input, both his reports and his contribution during the hearing. It is an excellent example of what an important role Independent Social Workers can have in Court of Protection proceedings. He came up with what seemed to me to be important suggestions and ideas for the future, such as having a JC day and training days. I hope his ideas are taken forward.
The Courtroom
The courtroom is a space that is very familiar to legal teams. I’m sure they feel at home in that space. But I think it’s important to recognise that it can be an alien space for families and especially Litigants in Person. Apart from me (and the journalist and ISW on the first day), everybody in the courtroom was associated with the parties to the case, other than JC’s mum and brother. There were seven people associated with the public bodies and two associated with the legal team for JC. Plus the judge. I imagine it can feel lonely for a family representing themselves in that sort of situation.
The oppressive nature was added to in this hearing by the very hot temperature inside the courtroom. At one point JC’s brother asked if he could take his tie off and the judge replied that he could even take his jacket off (he didn’t) and that “the courtroom has no temperature regulator, it is either freezing cold or boiling hot”. I was pleased that the judge noticed how JC’s brother was not on tip top form and reacted to that. Legal teams need to be conscious that families don’t know what they can and can’t do, even asking for water. And in a small courtroom like this was, being conscious of how sound carries is important too. Even small things can help alleviate the trauma of going through a Court of Protection process.
Judicial appeal came up in the recent Assisted Dying debate, with ex-judge Nicolas Mostyn suggesting that it is an easy process for Litigants in Person to do (speaking to Illora Finlay). I wonder how true this is, an opinion reflected by a reaction on X:
Gill Loomes -Quinn explained to me that there are practical barriers in going to judicial review for lay people, that legal professionals may not be aware of, or give due consideration. Not least that there’s usually a requirement to exhaust other options such as internal complaints procedures, which require that a) You are able to access the complaints procedure (this isn’t typically covered by the scope of Care Act advocacy, even if you qualify for one of those.) b) The Local Authority responds to a complaint. The problem is that if they don’t, the next step would be complaining to the Ombudsman – but they require a copy of the outcome of the internal complaint. Which if the LA hasn’t done anything with your complaint, you don’t have. A catch 22 situation.
Power
According to Gill Loomes-Quinn, power imbalances abound in this case. She writes: “Most constrained seem to be the family members/LiPs, who are at a disadvantage in the unfamiliar, formal legal setting of the court room and who rely on the public bodies and care providers to meet the needs of their loved one (and who risk being characterised as ‘difficult’ if they fail to ‘toe the line’). The judge is constrained by the limits of her jurisdiction and is required to accept the scope of the options presented to her. It seems like (in this sort of case) things are weighted in favour of the public body – access to funding for legal teams, power to decide what options are ‘on the table’, as well as the bottom line that P needs care, and alternatives available are limited (Direct Payments / ISFs present an illusion of ‘choice’ based on market principles, but this relies on there being options to choose from and in lots of areas this isn’t the case).”
Gill believes that this case highlights well the limited scope of the MCA 2005: “The Act provides a statutory framework for decision-making on behalf of those deemed to lack capacity but to talk of it ‘protecting’ P seems erroneous. To ‘protect’ someone in this P’s position would be to take steps to keep him safe and provide him with care that meets his needs – and it would be to ensure that he and his family are not expected to engage with care providers they don’t trust who have failed him in the past. Likewise, these things would be in his ‘best interests’. What the Act seems to protect and reinforce are existing power imbalances and social (dis)orders – all the ‘sweeping under the carpet’ of “moving forwards” and “looking to the future” in this case. Along with the failure of ‘professionals’ to realise that no matter how it is worded, the very enforcement of a WTA is suggestive of a finding of fault on the part of the family – otherwise why create one? They’re not enforced ‘as standard’. And it’s not much of an ‘agreement’ when it’s compelled?[12]But what other options does P’s family have? What happens if they refuse to agree? Or to participate in mediation?”
Gill continues: “It also strikes me that there is typically a failure on the part of ‘professionals’ to recognise the cumulative nature of the trauma experienced by disabled people or family members – or anyone who is a ‘service user’. So often, suggestions are made glibly – “Go to Judicial Review” – and (notwithstanding the inaccessibility and impenetrability of such mechanisms) these are made to sound so simple. There may be some recognition of the difficulties of inaccessibility for those unfamiliar with ‘the system’, but what I don’t really see is acknowledgement of the ‘burn out’ that occurs with years of such ‘battles’. Each failure of ‘the system’ to deliver results in a kind of fatigue (“Here we go again”) – along with an erosion of trust and a loss of hope – making even the genuinely simplest of administrative tasks feel insurmountable. I don’t think ‘professionals’ like to acknowledge how intensely adversarial and damaging the systems of which they are a part can seem to those they profess to help.
This case alludes to one of the phenomena that I think contributes to such ‘burn out’ – the ‘Tightrope’ that ‘service users’ (or family members etc) are required to negotiate: The need to advocate robustly for oneself (or loved one) while at the same time keeping the ‘professionals’ onside and avoiding being characterised as ‘difficult’ in a way that can impact the treatment received. The egos of service providers and public bodies can be very fragile.”
Moving Forwards
All in all, I left this hearing reflecting on many things. About the power imbalance between the carers, the care provider, the public bodies, the court and the family. About the focus on moving forwards, as if what had happened in the past could be swept away. About the onus on JC’s mum and brother to have “trust” in the organisation responsible for the care of their son and brother, an organisation that everyone agreed had made mistakes in the past. Mistakes that the family uncovered. About the fact that there was no accountability from the public bodies responsible for commissioning such poor care, public bodies that the court has decided can’t even be named. I left this hearing thinking about how much the court was really protecting P, despite all the Deprivation of Liberty Safeguards in place. I really hope that JC’s house can become a proper home for him, and that he does receive good care moving forwards. It’s what he deserves and what his mother and brother dearly want.
Amanda Hill is a PhD student at the School of Journalism, Media and Culture at Cardiff University. Her research focuses on the Court of Protection, exploring family experiences, media representations and social media activism. She is a core team member of OJCOP. She is also a daughter of a P in a Court of Protection case and has been a Litigant in Person. She is on LinkedIn (here), and also on X as (@AmandaAPHill) and on Bluesky (@AmandaAPHill.bsky.social).
[1] I have received two anonymised position statements, from the LA and ICB jointly, and the OS, as well as the approved court order. I have used information in those to write this blog post, as well as my own observations.
[2] Gill is a disabled scholar-activist and ‘service user’. Her PhD focused on the ‘Voice’ of disabled people in practices relating to the Mental Capacity Act 2005 (particularly in the Court of Protection). Gill co-directs the Open Justice Court of Protection Project.
[3] From here: An Individual Service Fund (ISF) is an arrangement where the budget for a person’s care and support arrangements is transferred from a Local Authority, directly to a support provider of the person’s choice. This enables the person to be in control of how their support is designed and delivered.
[4] The OS PS states that mum and brother were being asked to “ reconsider their rejection to engage in mediation; independent mediation between the family, the public bodies and the care provider can only be considered to be in JC’s best interests.
[5] This recent judgment from October 2025 provides useful information about fact finding hearings: [2025] EWCOP 37 (T3)
[6] An IMCA is an Independent Mental Capacity Advocate
On 13th November 2025, District Judge Davies (sitting remotely at Derby Family Court) authorised the deprivation of liberty of P, a young man who lives at home, for a period of six months. This authorisation came three years after the initial application in this case (COP 13670825).
I’ve observed two thirds of the hearings in this case: one on 10th April 2025 (“the April hearing”), and one on 13th November 2025 (“the November hearing”). As far as I can tell, there has only been one other hearing (in December 2024).
Derby City Council, the applicant local authority, is represented by Alison Bush, a solicitor employed by the Council itself. P is represented by his mother, acting as his litigation friend[i]. She was joined by P’s father at the April hearing but he was not present at the November hearing.
Here’s how this blog is organised:
In the first section of this blog, I’ll set out the background to the case.
In the second section, I discuss the support plans, and some disagreement about whether or not it should be written in the first person.
In the third section, I explain the hunt for an appropriate 1.2 representative.
Finally, I’ll explain the educational provision for P, and why the uncertainty around this has caused delays in the judge authorising a deprivation of liberty.
Background
Counsel for the local authority explained in a very helpful opening summary at the November 2025 hearing that this case “has a long but not overly complicated history”.
In October 2021, a judge sitting in the Court of Protection authorised P’s deprivation of liberty under the Re X streamlined procedure. As Eleanor Tallon has explained in her blog, the Re X procedure was established following the Supreme Court’s judgment in Cheshire West. It was intended “to provide a more speedy and manageable response for non -contentious community DoL application”
At that stage, P’s mother was appointed to act as P’s Rule 1.2 representative. As Eleanor explained in her blog, the role of a Rule 1.2 representative is “to make a statement to the court outlining the representative’s views on whether the arrangements are in the person’s best interests, without which the application cannot proceed.”.
A further application to authorise a deprivation of liberty was made in September 2022. At the November 2025 hearing, Counsel for the local authority explained (in a very detailed opening summary) that “in the intervening time [i.e. between October 2021 and September 2022], the courts generally had a change of heart [about] appointing family members providing care who are also 1.2 rep.”.
As a result, the judge considering the renewed application (Tribunal Judge Hornes) directed that a Court of Protection Special Visitor visit P and produce a report of his wishes and feelings. The proceedings were stayed until that report was filed, which happened in October 2024.
At that stage, P was out of school, and that was causing “issues” (I don’t know what but it sounded like the change in circumstances was causing distress to P). As a result, the judge removed the case from the streamlined procedure. At the April 2025 hearing, DJ Davies explained that this was “because the judge – Tribunal Judge Hornes – wasn’t happy to rubberstamp it, [and] that’s why it has come to the local court for further investigation”.
The case therefore was listed before DJ Davies in December 2024. Since then, he has also heard the case in April 2025 and November 2025.
Before getting into the substance of the hearings I observed, I’d like to pay testament to DJ Davies’s handling of this case. At various points he asked P’s mother if she had any questions, and answered them in a way that was crystal clear but not condescending. He repeatedly recognised the knowledge of P’s parents – including acknowledging the fact they have represented P at a SEN Tribunal.
In addition, at the start of the April hearing, at the request of P’s parents, he explained the role of observers in Court of Protection proceedings. He also asked if they had any objections to the presence of an observer[ii] (which they did not).
I’m glad that the judge dealt with that request for explanation in a fair and concise way but it is a shame that nobody had thought to explain the role of observers beforehand. I imagine that could be because P’s parents were not represented (indeed, P’s mother was representing P). For the lawyers reading this, may I suggest that you do make every effort to explain to family members that observers could be present at a hearing and direct them to our website for further information.
2. The support plan
At the December 2024 hearing (which I did not observe), the judge had directed that an up-to-date Care Act assessment and support plan be filed with the court in time for the next hearing. That hadn’t happened by the time of the April hearing, and he wanted to know why not.
According to Counsel for the local authority, the support plan hadn’t been prepared, “because that has taken a little longer – a lot longer – to discuss [the contents] with [parents], and the to–ing and fro–ining about what is to be included…The social worker visited on Monday and I understand that, on Monday, [P’s mother] has finally agreed the contents of the review assessment and also the new support plan”.
The judge wasn’t satisfied with that –
Judge:When was it actually agreed?
Counsel for LA:Monday, as far as I can understand.
Judge:So why haven’t I got it for today?
Counsel for LA:Because I don’t – I do apologise but I don’t have it yet. I was notified on either Tuesday evening or on Wednesday that [P’s parents] had agreed it. I don’t work on Wednesdays so I’m not in a position to have sent it to you before today.
Judge:But we would have made more progress if I’d had it today. I’m not sitting tomorrow so I can only review it on Monday.
It struck me that there was an under-current of blame-shifting. In particular, the blame for the delay was being laid squarely at the doors of P’s parents. However, P’s mother later told the court that both of them were unwell in February, and so had limited time to discuss the support plan – not quite the parental procrastination that counsel had made it sound like.
In her submissions to the court, P’s mother raised the issue that his support plan has been written in the first person. His previous support plans had not been written in the first person, but with a new social worker came a new approach.
The problem, P’s mother told the court, was a fairly simple one: “it indicates by putting it in first person that he’s written it. And I’ve said it shouldn’t be written like that….it would indicate he has fully written it and that he has capacity to join in the meeting, to be able to advocate himself…If you say ‘I’, it means I have taken part – P can’t take part”.
This wasn’t the first time that P’s mother was raising concerns about the use of the first person; she told the court that she had told the social worker about her misgivings. However, “it [third person] was removed because, in her [Social Worker’s] words, ‘I don’t like it so I’m changing it to the first person…For [Social Worker] her life moves on but they [support plans] stay with [P] for the rest of his life.”
In a similar way, P’s mother was also concerned that this new support plan made no reference to P’s diagnosis. Again, I want to quote directly from my notes of what she told the court: “[P]’s diagnosis has been removed from the support plan and I asked for it to be put back in. I was told it’s not necessary and irrelevant. To me, to remove it is to take away from all the importance of what we’re fighting for”.
I agree. The simple fact is that P would not be a subject of Court of Protection proceedings, and his parents would not have to fight for him to access education, if not for his diagnosis of an impairment of mind or brain (and the effect of that on his decision-making ability). To remove reference to it is to remove part of him from the support plan – somewhat ironic given that it’s written in first person.
The judge told P’s mother that he had seen many support plans written in the first person, including in his capacity as a Family Court judge. However, this wasn’t the most important part of the support plan: “I am more interested in substance over form” – that is to say, the court was more interested in what the plan said rather than how it said it. Nevertheless, he recognised the concerns, and said to the local authority counsel: “I want to hear why it’s in those terms and why – given [the] objections….why can’t it be re-written?”
Counsel responded that she will discuss this with the social worker, and take instructions on the point. She pointed out that this “might affect whether I can get the support plan to you for tomorrow”, to which the judge gently reminded her that he would not be at work until Monday. In fact, as the hearing came to a close, he directed (without asking if it was a workable timeframe) that the draft order and support plan be filed with him by Monday.
This issue was not raised again at the November hearing, which I assume means that the issue was satisfactorily resolved.
3. An appropriate 1.2 rep
As explained in the background section of this blog, the issue of identifying an appropriate 1.2 representative had caused considerable delay in this case.
During the April 2025 hearing, the judge had explained to P’s family why there may be a problem with those providing care also acting as a 1.2 rep: “The role of a litigation friend is to make decisions in proceedings. But a rule 1.2 rep is to be the voice of [P], advocating for what he wants. Sometimes, it doesn’t always happen, there can be a conflict of the roles – I’ve said it’s nuanced – and sometimes it’s better to have the 1.2 rep as somebody entirely independent. There are cases where someone can, and does, wear both hats. In my experience, in a Re X where we have deprivation of liberty in the community, even if there are no safeguarding concerns it’s sometimes better to have somebody else….[there is a] hypothetical potential for conflict of interest. Is there anybody else who can adopt that role or is it your case that you feel you can?”
P’s mother seemed understanding of the position. She told the court that she’d already asked another family member if she would take up the role but, as she also provided P with some support, she had come to realise (I think as the judge was speaking) that she couldn’t do it either. That left “the only other person who doesn’t have a caring role [which] is his eldest brother, and I didn’t realise it was an issue [meaning he hadn’t yet been asked] so therefore the only person I could ask is his brother”.
At this stage, the judge gave directions that the order would make provision for another Special Visitor’s report “but if somebody is prepared to come forward then we can simply vary the order and not do the report”.
By the time of the November 2025 hearing, P’s brother had indeed agreed to take up the role. Counsel for the local authority told the court that there had been some difficulty in acquiring a witness statement, detailing the brother’s views on P’s support plan and his care arrangements. It sounded as though P’s brother had filed the witness statement in April 2025 (so shortly after the last hearing) but this hadn’t made its way to the hands of the local authority until the Tuesday before this hearing (so two days before).
Counsel explained that, “the local authority’s position before we had received that was for the court to consider removing [P’s brother] as 1.2 rep”. At this point, the judge said what sounded like “not an option,” but counsel hadn’t realised the judge was speaking and had continued speaking herself. She told the judge that, as they had now seen the witness statement, the Council’s position was that the brother should remain as 1.2 rep.
The overlap between the judge and Counsel meant I can’t be sure that’s what the judge did say. However, I’m fairly confident that’s what the judge did say because, later in the hearing, he described the brother’s statement as setting out his views in a way “perhaps only a family member could – that’s been helpful”.
The final order, authorising P’s deprivation of liberty, was to be sent to P’s brother in his capacity as 1.2 rep.
4. Educational provision
At the April hearing, P’s parents wanted P to attend his College for a further year, funded by an EHCP[iii]. At that stage, it had not been agreed by the SEN team in the Council. The decision should have been communicated by the end of March but, come April, they were still waiting.
The question of whether P would receive educational provision has been relevant not only to the support P will receive but what the deprivation of liberty that the judge was authorising would look like. If P was not to receive education for a further year, there would need to be a “Plan B”.
At the November hearing, it was confirmed that P has been approved for further time at College. Unfortunately, there were more problems.
As it stood, the Council’s SEN team had said that P can stay at the College for another academic year (and indeed had already started). However, the College hadn’t confirmed that they were prepared to offer a place to P beyond December.
The judge asked P’s mother whether she had “any straws in the wind” as to whether P could remain past December. She told the court that it seemed the delay was purely administrative, and that the College would be offering another year to P. She told the court that the delay in confirmation came down to the fact that, at an in-person review at the College, Derby City Council had been invited to (but ultimately didn’t) attend. The College then didn’t know the funding had been confirmed for the full academic year, meaning they couldn’t confirm that P could stay beyond December.
The judge seemed content with this. He asked P’s mother to explain what the plan was after the end of the academic year, when P would no longer be attending education. P’s mother gave the court a great deal of detail about the service provision she had been looking into. It would be unnecessarily intrusive for me to describe what that was but, in the words of P’s mother, they all converged on the aim that “[P] will have a fulfilled life which is what he needs and deserves”.
The judge therefore identified that the support plan will need to change around the middle of 2026, meaning the care arrangements (that amount to a deprivation of liberty and therefore require court authorisation) will change then. After canvassing the views of P’s mother and Counsel for the local authority, he confirmed that he’ll authorise the deprivation of liberty for six months. At that point, the council will need to re-apply to the court for a further authorisation – though this might not need a hearing, and may well be approved by the streamlined procedure. In the meantime, if the College say P cannot stay beyond December, “the matter needs to be brought back, and my door is always open”.
The judge concluded the hearing by addressing P’s mother: “We might meet again [P’s mother] but, if not, I wish you, [P], and the rest of the family well”.
Daniel Clark is a member of the core team of the Open Justice Court of Protection Project. He is a PhD student in the Department of Politics & International Relations at the University of Sheffield. His research considers Iris Marion Young’s claim that older people are an oppressed social group. It is funded by WRoCAH. He is on LinkedIn, X @DanielClark132 and Bluesky @clarkdaniel.bsky.social.
[i]As far as I am aware, this is the only blog published by the Open Justice Court of Protection Project where a family member has acted as P’s litigation friend.
[ii]Any party or interested person is entitled to object to the presence of observers. In such an event, it’s for the judge to decide whether observers will be permitted to attend or whether the case should be heard in private (see Court of Protection Rules 4.1-4.4). For a report of a hearing where the protected party objected to the presence of an observer, and the judge ruled that the case should therefore be heard in private, see: Balancing open justice and P’s right to privacy: A protected party says NO to a public observer “and her voice shall be heard” by Eleanor Tallon. These decisions are case-specific: P (or their family) cannot veto public observers or insist on private hearings.
[iii]The UK government website explains what an EHCP is: “An education, health and care (EHC) plan is for children and young people aged up to 25 who need more support than is available through special educational needs support. EHC plans identify educational, health and social needs and set out the additional support to meet those needs.” BBC’s Panorama have produced a documentary that explores the difficulties that families face when trying to acquire an EHCP and specialist educational provision: Kellie Bright – Autism, School and Families on the Edge
The protected party is a man in his 40s, with Down Syndrome and learning disabilities. In 2022, he was diagnosed with ‘significant renal problems’. They’ve been difficult to monitor because P’s father, with whom he lives, is said to believe that doctors intend to harm his son.
At the hearings we observed in 2024, the applicant Trust (the Royal Free NHS Trust in London) said that Ps life might be in danger. The Trust was seeking authorisation to remove P from his home (by force if necessary) to hospital so that further tests could be carried out and decisions made about treatment in his best interests.
After P was assessed in hospital in October 2024, he was discharged home. A final court order of 24th November 2024 allowed P to be discharged home on the condition that his father would take him for out-patient dialysis three times a week. Proceedings concluded at that point. There is no published judgment.
This blog reports on a hybrid (in person and remote) hearing before Mr Justice McKendrick at the Royal Courts of Justice on Wednesday 8th October 2025, which re-opened the proceedings. A new application had made on 1st October 2025 by the same NHS Trust (Royal Free London Hospital Trust) concerning the same patient. I attended the hearing in person.
In the blog I will detail the new application before the court, report on the hearing and in particular the judge’s frustration with Barnet’s non-compliance with previous court orders to commission and file a psychologist’s report, and end with some reflections on non-compliance in the Court of Protection.
New Application
The Trust says that, over the past year P has increasingly been missing his dialysis sessions at hospital. In June 2025, P was admitted to hospital for dialysis for three days, following some missed sessions. Since then (up to mid-September 2025) the Trust says that P has missed 11 out of 40 dialysis sessions and has not stayed for the full 4 hours on more than half of the sessions, and that they could not persuade P’s father to allow P to stay for the full treatment period. Further concerns have been raised by the Trust that P is not taking his medication as prescribed or eating the right diet (resulting in high phosphate levels). The position of the Trust (represented by Victoria Butler-Cole KC) is: “P is at risk of very serious complications as a result of under-dialysis including sudden death from an electrolyte abnormality, fluid accumulation leading to difficulty breathing and pressure on the heart, chronic damage of blood vessels, and the development of calciphylaxis, a painful and sometimes fatal ulcerating skin condition.”
This application also asks the court to ‘fully investigate’ the option of removing P from his father’s care. He has lived with his father all his life, so this would be a draconian step for the court to authorise.
The parties are:
the applicant – Royal Free London Hospital Trust with counsel Victoria Butler-Cole KC (who was on a remote link)
P – via his Litigation Friend the Official Solicitor with counsel Sophia Roper KC (also on a remote link)
P’s father – who is unrepresented at present (also on a remote link, accompanied by P, from his hospital where he was having dialysis)
the Local Authority (London Borough of Barnet) with counsel Kate Round (who was in court in person)
The Trust was asking the court to order (again) the appointment of an expert psychologist to consider the following (reproduced from the Position Statement of the applicant Trust):
What further steps, if any, might be effective in persuading [his father] to take P to dialysis for every session, and to stay there for the full 4 hours.
What further steps, if any, could be taken to ensure that P receives his prescribed medication while living with [his father].
What options the expert psychologist considers are in P’s best interests.
The impact on P of moving to live apart from his father;
The feasibility and impact of the imposition of any restrictions on contact between P and his father;
What steps, if any, could be taken to mitigate the negative impact of such arrangements;
The Trust also asked the court to ‘remind’ P’s father of ‘the importance of full compliance with P’s dialysis schedule’ and also to gather information (via witness evidence) from the Local Authority regarding compliance with allowing carers to see and work with P, giving him his medication and the care he is said to need. And additional residence options from the LA ‘in the event he did not live with [his father]’
The Hearing
The hearing was in Court 35 at the Royal Courts of Justice. The courtroom is large, and I was able to sit at the side of the court, in the press bench, rather than at the back where observers usually sit. This is because I (and my co-observer and OJCOP team member, Amanda Hill) asked the court usher if we could sit in the press bench to make the hearing more accessible: sitting at the side means that you can see everyone’s faces (the judge and counsel and people attending for parties, who face the judge). I have a hearing impairment and even with hearing aids, sitting behind people talking makes it tricky to understand what they are saying. So, this was a welcome permission from the court. I was also very pleased to be attending in person, since hybrid hearings are often hard to hear (much more so than fully remote ones).
It was evident at the start of the hearing that P and his father were behind a cubicle curtain on a hospital ward, and although P’s father was wearing headphones (so the court was not audible to anyone else), anything P’s father said would be heard by other people on the ward. The judge asked whether a private room in the hospital could be provided, and counsel for the Trust said “we did ask but there was not enough notice of the hearing date to arrange this: it could be possible in future”. So, the hearing went ahead on that basis, with P and his father taking part from his hospital cubicle.
After introducing the new application and current situation, counsel for the Trust raised the further issue regarding a psychologist report which the judge had ordered (on 26th November 2024) that the Local Authority (London Borough of Barnet) must submit in the previous proceedings . The Local Authority had never submitted it.
The approved Order from this hearing (8th October 2025) states that the Local Authority had been: ‘… directed to file a report by a psychologist by 7 February 2025 which was not complied with, and no application was made to vary or discharge that order before the proceedings stood dismissed on 20February 2025’.
It transpired that the psychologist’s report was intended to inform the court (amongst other things) about the potential impact on P of being removed from living with his father. But the court did not have the advantage of this previously-ordered report at these new proceedings. The judge was not happy:
Counsel for the Trust: Given the risks this really needs to be looked at with the most careful scrutiny to decide what to do.
Judge: I am very much in agreement. That’s why the Local Authority was ORDERED to produce a report from a clinical psychologist so that what has come to pass [i.e. P’s father not taking him for treatment] would not come to pass [in future]. Notwithstanding the careful orders made, we are in October 2025 with no identified expert until February 2026 and I am told he’s at risk of sudden death. I am struggling to understand why the Local Authority are not first of all apologising for ignoring an order of the court and, secondly, why a clinical psychologist [hasn’t been instructed]. I am struggling with why it’s necessary to make directions to follow an order already made – here we are almost a year down the line – to sanction a single joint expert.
And later:
Judge: Despite the father’s promises – which he made to me in court – none of that has come to pass. It was ordered that there would already be a clinical psychology report to assist me. I am not in that position and now we face significant delay which might put P at risk.
It did sound (from what counsel for the Trust said) as though a psychologist had tried, earlier this year, to meet with P, but “wasn’t able to engage his father or P in a meeting” (counsel for the Trust). That psychologist had apparently been connected to the Local Authority and the parties were now proposing an independent psychologist in the hope that someone clearly independent might be more successful.
Counsel for the London Borough of Barnet (Kate Round) said: “My Lord, technically it would have been better if we had notified the court that we couldn’t get that report and why. It is with regret that we don’t have it. We had identified someone – at the moment it’s a perennial problem. Either we can’t identify anyone or it’s not good enough and then we have to go to an independent expert. We do apologise.“
The judge responded like this: “It’s no good apologising to me …. you’re putting P at risk. I’ve got a bee in my bonnet this week. I have had cases with public bodies and the court makes orders and the public bodies don’t comply. If I did have that clinical psychology report I COULD have listed the hearing for a short hearing.”[judge’s emphasis]
The judge, understandably, was concerned about the urgency, given that he was being told that P’s life was at risk. Counsel for the Trust said: “It’s not urgent, not the next fortnight. After the last hearing in November 2024 there was a period of full compliance for a number of months. We want an order to say that he [P’s father] must take P every Monday, Wednesday and Friday and must stay for the four hours. We are hopeful that the court reminding [P’s father] of that might help, while we are gathering evidence. Previously, he said he hadn’t agreed that it was in P’s best interests to receive dialysis. Certainly, if a psychology expert can be found to report in a shorter time-scale I don’t think I am instructed to ask the court to make provision more urgently than that.”
Then there was an interesting, brief exchange between the judge and counsel for the Trust, about penal notices:
Judge: The draft order doesn’t include any penal notices. Is that deliberate?
Counsel for the Trust: It is. The Trust recognises that P’s father IS bringing him and he is attending to a degree. They are keen to encourage that to continue, and I have no instructions to attach a penal notice. [Counsel’s emphasis]
So, despite the fact that P’s father was in breach of court orders in relation to facilitating and not impeding P’s care and medical treatment, the Trust had decided not to seek to penalise him for this. The judge then spoke to P’s father and P:
Judge: I hope you have been able to follow. What I am going to do is list this matter for a hearing between now and December and I am going to have a clinical psychologist instructed to assess the impact on [P] of living apart from you and that’s because, for a large part of this year, he’s not received the dialysis to keep him healthy. And that’s ONE option to live apart from you to be assisted by support workers. I am also being asked again to make an order on you to facilitate his dialysis: you take him, don’t interfere and call 999 if there are any significant difficulties and you follow advice from the dietician. We went through this in 2024 and you PROMISED me …. [judge’s emphasis]
Father: [interrupting] … which I did … 4 hours he is ill, all this has been happening …. [difficult to understand via video link] complicated …. So that’s the reason …. I am looking after my son for 44 years, I know what he’s able …. 4 hours is [missed] 3 hours is much better, he says he’s better. (I think P’s father was saying that 4 hours of dialysis makes P feel more ill and that he prefers 3 hours, but we didn’t hear from him what P says about his treatment, or why his father believes this might be the case).
Judge: What I am going to do [name of P’s father] is to direct the public bodies to explain the reasons for P to have dialysis [in the way they advise] and to find out what you think the impact on P would be of living apart from you, and to explain [why you have been doing what you have been doing]. I’m going to direct you to file a detailed witness statement, saying if you believe in dialysis, what you think the impact on P would be if he lived in supported living. You may need to give evidence at the hearing in December. In the meantime, I am going to make an order like the one in November….are you going to comply with it?
Father: Yes, I … accept anything …. [difficult to understand] the entire case …. I …
Judge: Yes well [name of P’s father] it’s very important that when you take P to hospital you stay for 4 hours, and 3 hours is not enough.
Father: OK and if anything happens to my son after 3 hours, who is responsible?
Judge: I’m sure that he’s in the hands of experienced clinicians at the hospital.
Father: [talking loudly – but I can’t understand what he’s saying at this point]
Judge: Have you seen the Position Statements and the evidence for today’s hearing?
Father: [unclear answer] I call the 99 …
Judge: [addressing P’s father by name] It’s very important you read the documents please. The evidence before me is that P is at risk of serious complications and at risk of dying from electrolyte abnormalities. You’re his father and I am asking you to please comply.
Father: Can P speak?
Judge: I will speak to P. Good morning [P], this is the judge. Do you remember speaking to me at the end of last year?
P: I do
Judge: You were smartly dressed at that time. It’s important [P] that you come to hospital for appointments.
P: Which I do.
Judge: Sometimes it’s difficult and boring?
P: It is
Judge: But you must keep coming to hospital
P: [inaudible]
Judge: Okay, just keep coming to hospital with your father. Are you still going to football matches. Which team is yours?
P: Yes …Arsenal.
Judge: I hope they are playing well.
P: They are actually!
Sophia Roper KC, acting for P on behalf of the Official Solicitor, addressed the question of who should be instructed to complete the psychological assessment and report to the court. She informed the judge that the proposed independent expert psychologist had been contacted the day before and “what we have NOW been told is that he will not be able to report until February 2026. Five other independent psychologists and psychiatrists have been contacted. It’s up to the LA to decide if they can provide an in-house psychologist. They would likely be more amenable to be directed to provide a report [earlier] than an independent expert.” [counsel’s emphasis]
The judge expressed his frustration again, at the predictable situation:
“I am going to adjourn for 30 minutes this morning to allow for discussion and phone calls to be made. Given what I have been told about the medical situation, it’s essential to have a report by the end of the day. The previous order entirely envisaged the situation in front of you.”
There was then a break of half an hour to allow counsel to establish the timescales within which a psychologist could report back to court.
Despite the earlier suggestion that a psychologist independent from the Local Authority would be preferable, in terms of P and his father’s likely engagement, counsel for the LA said:
“If there were an independent expert available we would prefer that. However, we have got the lead clinical psychologist – [name] – she has confirmed she can do a report by the end of November 2025. […] We have flagged with her about working from [P’s] home… she has said if clinically appropriate or she could see him at the hospital. We hope she would be able to see P and his father at their home for the assessment. […] It’s important for the court to understand the potential damage to P from taking him away from his father. The best way of getting to that is by way of this report, so we really hope the father will allow this work.”
The Local Authority also agreed to pay for the clinical psychology report, whether it ended up being an independent expert or not.
When the judge spoke to P’s father to inform him of the plan for the psychologist assessment, his father said “I am happy to do so, for my son” and that he “is a human being with human rights”. P’s father also said “it is very important to protect my son’s life from everyone, I lost my wife”. I wondered at this point whether P’s father was fearful of healthcare professionals and of medical interventions, because he linked the conversation to the loss of his wife. When we first reported this case it was said that P’s father believed doctors were harming his son. It made me wonder about any experiences with doctors in his wife’s care.
The judge strongly encouraged P’s father to seek representation in time for the next hearing, warning, “I will not look favourably on an application to adjourn a final hearing on the basis that you can’t find a solicitor”. He replied, “Okay, yes”.
My co-observer’s notes say (but I didn’t record this) that Sophia Roper KC then made a point about non-compliance with orders, to which the judge replied: “I’ve vented my spleen on non-compliance with orders and I won’t be reading any other correspondence (about that)”.
The next hearings are currently listed as Pre-trial review at 2pm on Thursday 4th December 2025 and a final hearing on Wednesday 17th and Thursday 18th December 2025 in person at the Royal Courts of Justice.
P’s father has been ordered by the court to attend in person and to arrange for someone else to accompany P to hospital if it is one of his dialysis days.
Reflections on non-compliance
I have observed many hearings where parties have not complied with orders of the court: sometimes public bodies and sometimes family members.
In this case, there’s non-compliance with court orders from both a family member (the protected party’s father) and from a public body (the London Borough of Barnet).
Non-compliance from the family member is currently being dealt with by education (the public bodies are to explain to him why dialysis is so important for his son, and the judge asks him to read the documentation about this) and “encouragement” (with an order, and with something that might be experienced by him as a threat that the possible alternative to compliance might be removal of his son from the home). There is no penal notice attached to the order.
I have never observed a penalty of any kind, other than judicial reprimand, being directed at a public body for non-compliance (otherwise known as contempt of court). It’s made me wonder whether penalties for non-compliance are ever given to public bodies, and if so, what kinds of penalties are possible.
“A failure to comply with the mandatory injunction set out at paragraph 5 of the order of his Honour Judge Keyser QC, on the basis that the Defendant did not as of 7 January 2022 and still has not completed future placement planning for the Claimant.”
“The Defendant has also failed to comply with paragraph 6(a) of that order in that no sworn affidavit has been filed by the relevant director of the Defendant explaining the breach of the injunction.”
The judge was clear:
“Contempt proceedings may be brought against a public body for a failure to act in accordance with an order of the court. In proceedings in the Administrative Court, it is not the usual practice to include a penal notice on an order against a defendant public body. In R (JM) v Croydon London Borough Council [2009] EWHC 2474 (Admin), Collins J held that a penal notice is not necessary to enable the court to deal with public bodies by means of proceedings for contempt as public bodies would seldom find themselves in the position where committal would be contemplated. Collins J observed at [12]: “Accordingly, I do not think that a penal notice is necessary in orders made against a public body. A failure to comply with an order can be dealt with by an application to the court for a finding of contempt and, if necessary, a further mandatory order which may contain an indication of what might happen should there be any further failure to comply. Adverse findings coupled with what would probably be an order to pay indemnity costs should suffice since it is to be expected that a public body would not deliberately flout an order of the court. Were that to happen, the contemnor could be brought before the court and, were he to threaten to persist in his refusal, an order could be made which made it clear that if he did he would be liable to imprisonment or a fine.” ((§56, JS (by his litigation friend) v Cardiff City Council [2022] EWHC 707 (Admin))
This judgment states clearly that, should a public body ‘deliberately flout’ a court order, imprisonment (though ‘seldom’ used) or a fine are options for the court. But, I wonder, who would be imprisoned? And a fine would disadvantage further the citizens who rely on that public body (as Munby J says below).
The case against Cardiff City Council found the council to be in contempt of court but does not detail the penalty imposed. Instead, the judgment states:
‘I bear in mind that in R (Bempoa) v London Borough of Southwark [2002] EWHC 153 (Admin), Munby J concluded that the gravity of that local authority’s contempt could be adequately marked by the delivery of the court’s judgment in public. The “public humiliation” of a judgment the contents of which publicly shamed the local authority was a greater penalty than the exaction of a financial penalty which could only be to the financial disadvantage of the inhabitants of the local authority area, and those who rely upon the authority for the services it provides, without providing any corresponding financial benefit for the claimant.The contents of this judgment shame Cardiff City Council. Whether any further penalty is appropriate in this case is likely to depend, amongst other matters, on whether an apology is forthcoming and on the strenuousness of the efforts the Council now makes to comply with the mandatory order which remains in effect.’ (§94-95 JS (by his litigation friend) v Cardiff City Council [2022] EWHC 707 (Admin))
I would be interested to know whether the penalty of ‘public humiliation’ is ever considered sufficient for family members who do not comply with court orders in the Court of Protection, as opposed to fines or prison sentences (or other sanctions). Although this is not (as far as I know) stated by the judge as an intended penalty in his decision to name Philip Esper (who was found to have committed contempt of court but given no penalty), it’s clear from the fact that Mr Esper appealed the decision to name him that he experienced simply being publicly named as a penalty in and of itself (Esper v NHS NW London ICB (Appeal: Anonymity in committal proceedings) [2023] EWCOP 29).
In the case I’m reporting on here, non-compliance from the public body was dealt with by judicial expressions of incomprehension (“I’m struggling to understand…”) about the Local Authority’s failure to act and about their failure to apologise for not doing so.
This led to an acknowledgement of (some) fault by Barnet (they admitted that “technically” they should have let the court know about the difficulties they were having), and to an expression of regret and an apology – which was not really accepted by the judge (“It’s no good apologising to me…”).
It was notable that, given a half hour break in proceedings to focus on dealing with the issue, it seems they were able to solve the problem and work out how to commission a psychologist’s report (albeit not an independent one) by the end of November. Court proceedings do seem to focus minds and galvanise action. A court hearing is, however, rather an expensive and unwieldy method for prompting actions that should properly have taken place in any event. It’s very common though – due here to what counsel described as the “perennial problem” of getting adequate reports on time.
As described in an earlier blog post (Non-compliance: What happens when public bodies don’t obey court orders?): ‘There’s a lot of non-compliance from public bodies evident in Court of Protection hearings every day. It’s routine to hear apologies tendered to the judge for not having submitted reports in time or complied with other directions and orders – pleading staff sickness, failures to respond to an enquiry further down the line, and administrative errors. Mostly judges seem resigned to it. It’s no secret that health and social services (like HMCTS) is underfunded, under-resourced and struggling to deliver basic services.’
Senior Judge Hilder sets aside one day each month for hearings to deal with non-compliant public bodies – but if they then comply not less than seven days before the date of the listed non-compliance hearing, it’s vacated. Celia Kitzinger reflects that, in five years of observing Court of Protection hearings, she has never before observed a ‘non-compliance’ hearing and, as the blog notes: ‘Apparently this is because the effect of listing them is rapid compliance, meaning that case never appears in the public listings’.
I find this quite astonishing – either something can be done or it can’t. Public bodies shouldn’t need to wait for the equivalent of a ticking off by the headteacher to do what they should (and can) be doing. Hearings in court cost (a lot) of money and, I would argue, shouldn’t be used for this purpose.
Claire Martin is a Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a member of the core team of the Open Justice Court of Protection Project and has published dozens of blog posts for the Project about hearings she’s observed (e.g. here and here). She is on X as @DocCMartin, on LinkedIn and on BlueSky as @doccmartin.bsky.social
Contact is a recurring issue in Court of Protection proceedings. I have been working in this area for eight years and my rough estimate would be that a dispute around contact (justified or otherwise) has arisen in around 30-40% of the cases I work on.
Where an adult lacks capacity to make their own decisions about who they see and how often, disagreements can arise between families and professionals about what contact is appropriate, safe, or sustainable. For families, restrictions on contact (e.g. limited hours of contact, contact only via phone or video-link, supervised contact only) can feel abrupt and disproportionate. It can also be interpreted as a ‘punishment’ for querying or complaining about their relative’s care.
This post explains how the Court approaches these cases, what the legal framework actually requires, and how evidence is scrutinised.
Where I have referred to ‘public bodies,’ this means the Local Authority, Integrated Care Board (ICB) or Health Board; whoever is the Supervising Authority that makes decisions about (and sometimes funds) a vulnerable person’s residence and care arrangements.
Capacity to make decisions about contact
Before the Court can make any decision about contact, it must determine whether the person (“P”) has capacity to make such decisions themselves. This cannot be assumed on the basis of assessments regarding capacity in other areas e.g. residence.
Capacity must be assessed for the specific decision, and sometimes the specific person, in question. I have seen cases where P is deemed to have capacity to determine contact generally, but lacks capacity regarding one individual. This may be where P has been particularly reliant on that person for a prolonged period of time and is unable to weigh up the impact of seeing that person on their wellbeing.
If P has capacity, P makes the decision, even if professionals disagree or would make a different choice. If P lacks capacity, the Court can then consider what contact is in P’s best interests. This is, of course, subject to the agreement of the person with whom contact is being considered – the Court cannot force a person to have contact with P if they do not consent, nor will they insist that P have contact if that is not what they want.
Best interests decisions are P-focused
If P lacks capacity to decide on contact, the Mental Capacity Act (s4) requires that decisions are made in P’s best interests. This means the decision must be centred on what is best for P – not what family members want, and not what is easiest for care providers.
Under s4(6) of the Mental Capacity Act 2005, the Court is required to consider, so far as is reasonably ascertainable:
(a) the person’s past and present wishes and feelings (and, in particular, any relevant written statement made by him when he had capacity),
(b) the beliefs and values that would be likely to influence his decision if he had capacity, and
(c) the other factors that he would be likely to consider if he were able to do so.
S4(7) of the Mental Capacity Act requires the views of of family, carers and professionals to be taken into account, if it is appropriate and practical to consult them. This does not necessarily mean considering what that person (e.g. a relative) wants to happen, but rather utilising their knowledge of P to help inform what P would decide.
The final decision must always be based only on what is best for P.
Care home rules vs Court-ordered restrictions
Restrictions on contact can occur in one of three ways:
The placement can impose their own rules;
The Local Authority/Health Board/ICB can apply to Court to restrict contact; or
The Court can order restrictions without such application.
I will look at each of these in turn, and then consider what evidence is required to authorise such restrictions and how this can be challenged.
Placement-imposed restrictions
Regulation 9A of the Health and Social Care Act 2008 (Regulated Activities) Regulations and the associated CQC guidance (link here) states that ‘Unless there are exceptional circumstances, service users whose care or treatment involves an overnight stay or the provision of accommodation in a care home, hospital or hospice, must be facilitated to receive visits at those premises.’
The starting position is therefore that contact should be facilitated. However, 9A4 states that ‘Nothing in this regulation requires a service user to receive a visit, take a visit out of a care home or be accompanied… where the service user lacks the capacity to give consent, where it would not be in the service user’s best interests.’
There is no specific definition as to what constitutes ‘exceptional circumstances,’ however it is suggested this may include, ‘to protect the person using the service, other people using the service, staff or people visiting, where there is a significant risk to their health, safety or welfare.’
Placements are therefore able to restrict contact if it is deemed in P’s best interests. However, the following is contained within the guidance to the Regulations:
‘Where a risk has been identified we expect providers to implement appropriate precautions to enable a visit to happen safely, rather than prevent visiting altogether.’
‘This should always follow the preferences of the person using the service, wherever possible, and their assessed needs. ‘
‘Providers must consider that any restriction to a person’s right to receive visitors is lawful, has a legitimate aim and is proportionate. ‘Proportionate’ means that there is the least restriction possible to achieve the aim.’
‘If there is a need for additional precautions or a restriction to be put in place, the provider should apply the most proportionate and least restrictive option.’
‘Providers should not apply blanket decisions or long-term restrictions. They should review decisions to restrict visiting regularly by working together with the people involved.’
In essence, if there are concerns about contact, then restricting contact should be a last resort and alternative measures should be considered.
Contact Agreements
An alternative measure may be agreeing a Contract of Expectations for both staff and the family, setting out what each party understands to be expected of them.
In Re RK (Capacity: Contact: Inherent Jurisdiction) (2023), the judge declined to authorise a specified contact arrangement as he deemed RK had capacity and did not want contact with her family, but he did recommend that a ‘supportive framework’ be implemented, as follows:
‘I do not feel it right that I should prescribe the precise terms of the supportive framework; it should nonetheless incorporate – so far as possible – the essential points raised by each of the parties.’
These included, although were not limited to:
R to be asked about contact with the family at key events in the calendar – birthdays / Christmas / Easter;
R will be supported by the key worker to integrate with her friends outside of the placement;
Updates to be provided to the family at intervals (three monthly) about progress with attempts to encourage R to have contact; and
A key worker shall be appointed to spend time with R and ensure that her family remain alive in her mind and that she is encouraged to think about her future involving them in her life.
If contact restrictions are implemented, the public body should be informed and consideration given to seeking Court authorisation.
Public Body and Court-imposed restrictions
The Local Authority/ICB/Health Board is able to restrict contact between P and their family (if P lacks capacity), but they should make an application to the Court of Protection to authorise any restrictions. The Court will be very critical if the public body does not make that application promptly.
The public body has a duty to consider how meaningful contact can be promoted if in P’s best interests. As above, the starting point will always be that P should be able to see the people important to them in as natural a way as possible.
When restrictions on contact may be justified
Article 8 of the European Convention on Human Rights protects the right to respect for private and family life. However, this right can be lawfully restricted if necessary and proportionate to protect the rights and freedoms of others – in this context, P. This means that Article 8 is not breached if limiting contact is necessary to protect P.
For example, in Re G (Court of Protection: Injunction) [2022] EWCOP 25, an injunction that restricted the family’s contact with P (amongst other things) was held to be lawful on the basis of evidence from numerous witnesses stating that P’s father had been hostile and intimidating to staff, and had tampered with medical equipment.
See also MB v PB [2022[ EWCOP 14, blogged about here. In this case, face-to-face contact between P and her husband had been prohibited, following allegations (and subsequently ‘findings’ – see below) of controlling and coercive behaviour.
The Court must consider Article 8 carefully, but a justified and proportionate restriction will not necessarily breach it.
Contact restrictions can take different forms: frequency restrictions, supervised contact, limits on location, or suspension of contact entirely. They may be justified in a range of situations, including:
Where contact causes distress or destabilisation For some people, particularly those with significant cognitive impairment, contact can lead to confusion, agitation, or behavioural deterioration afterwards. In A Local Authority v PB (2011), the Court permitted night-time restrictions because evidence showed P became more confused and unsettled following overnight contact.
Where contact undermines P’s stability or placement If family members are alleged to make significantly negative comments to P about the placement, this may cause P to demonstrate challenging behaviour, leading to the placement not being able to meet their needs. A move to a new placement, especially if unplanned, is a significant risk in itself. This may also apply where family members are said to be aggressive or hostile to staff, causing P distress and affecting the staff’s ability to meet their needs. See Luba Macpherson and her concerns regarding the care of her daughter.
Where there are concerns about physical risk This could relate to ignoring essential dietary rules, not following medical instructions, or behaviour which puts P or others at physical risk.
By contrast, in SR v A Local Authority & Anor (2018) EWCOP 36 , the Court refused restrictions on a husband’s contact where there was no evidence that contact posed a risk. The Local Authority were concerned that the husband had made comments that indicated he was in support of euthanasia and exhibited ‘distorted or grotesque thinking,’ (§18) but did not allege that the husband concretely intended to end P’s life. P had remained safe during extensive previous unsupervised contact. It was held by HHJ Buckingham that: ‘Whilst I accept that JR’s comments have given rise to legitimate anxiety on the part of the professionals, I do not consider that there was adequate investigation into the reasons why JR has made such comments and what he understands by the notion of supporting euthanasia, which from his evidence related to the right to self-determination and dignity… I have reached the conclusion that the restriction sought by A Local Authority is neither justifiable, proportionate or necessary.’ (§44 & §46)
Occasionally, assertions are made that P’s family are demonstrating ‘coercive or controlling’ behaviour and this can be promoted as a justification for restricting contact. The Family Procedure Rules 2010 in Practice Direction 12J define coercive behaviour as ‘being an act or a pattern of acts of assault, threats, humiliation and intimidation or other abuse that is used to harm, punish, or frighten the victim.’ A recent example is Caroline Grady, who was found to have acted abusively towards her mother – see previous blog here.
Unfortunately, terms like ‘coercive behaviour’ are sometimes used by public bodies in a vague context when family members believe they are simply being protective. Such allegations (and all others) should be properly particularised (i.e. details of specific events provided) and their meanings clarified.
Restrictions must always be in P’s best interests – and the Court will examine their basis
Contact limitations can sometimes arise where providers (e.g., a care home) misinterpret a family raising concern as hostility or risk or adopt a defensive or risk-averse position. This frequently feels like a punishment directed towards the relatives for raising concerns about the care that their loved one receives.
However, when the Court becomes involved, it will examine the actual basis for the restrictions. The Court will not impose or uphold limits as a punitive measure. Any restriction must be justified by reference to preventing harm to P, and must be proportionate to the level of risk. Where the evidence does not support restrictions, the Court will not endorse them and will remove or relax them.
Evidence and scrutiny
A restriction must be capable of being justified by evidence. Evidence might include:
care home records
incident logs
behavioural charts
phone, message or call logs
CCTV
medical records.
Sometimes decisions are made rapidly when concerns arise, before full evidence is obtained. The Court may agree to short-term protective measures while records, CCTV, call logs or incident reports are reviewed, but with the understanding that these are short-term only. Permanent or long-term restrictions will require proper evidence. There is no set form that this evidence should take, but it may involve the records set out above, witness statements, expert reports, etc.
Family members who are parties to proceedings will almost always be able to file their own witness statements and attach evidence to those, if required. The Court order will provide a set date for these to be provided. Family members who are not parties may also be allowed to provide a statement, but this is subject to the Court’s discretion and permission for this must also be contained within an order.
Evidence that can be filed by family members often includes correspondence with the public bodies that demonstrates reasons for lifting contact e.g. birthday cards showing an ongoing, loving relationship, examples of positive contact, etc.
Records
Families (and all other parties) are entitled to ask the Court to order that these records are disclosed in proceedings. They may assist in determining, for example, whether P truly demonstrates challenging behaviour after contact or whether there may be a different trigger. A care home or placement would need an exceptional reason for refusing to release records into proceedings, although it can be agreed for some parts to be redacted if necessary (e.g. if there are references to another resident).
The Court may determine that some records are not appropriate for involved family members to see, and this will be considered in each case. Sometimes an order is drafted that allows only P’s solicitor to see the records. This is almost always the case (in order, it is said, to promote P’s dignity and privacy) but this can be challenged by family members and reasons requested.
If concerns arise around the accuracy of the records, this can be challenged by raising the issues within a witness statement (which parties are generally required to provide at set intervals,, requesting additional records from a different organisation or by asking the Court to order that the author of the records provide a witness statement to explain any inconsistencies or errors. This is subject to the Court’s discretion and reasons/evidence must be provided as to why these courses of action are necessary.
Finding of Fact Hearings
The Court of Protection is also able to order a ‘Finding of Fact’ hearing. This is a relatively lengthy hearing where the Court will hear from relevant witnesses who will be questioned by the other parties. This allows the Court to decide ‘on the balance of probabilities’ (i.e. whether an event is more likely than not to have happened, often simplified to a likelihood of 51% or higher) whether a certain thing happened or not. This is different to, and much lower than, the criminal burden of proof which is ‘beyond reasonable doubt.’
For example, they may make a finding that a relative did or did not financially abuse P, or withhold their medication, etc. The allegation is then either accepted by the Court as fact or, if the finding was not made, the allegation cannot be relied upon further (see Abuse and coercive control? A fact-finding hearing and exoneration, where a relative was exonerated from the allegations made against her by public bodies.)
In essence, the Court may order a Finding of Fact Hearing if the disputed issues of fact are relevant to the decision as to what is in P’s best interests.
In essence, a Fact Finding hearing may be ordered where the issues in dispute are relevant to the decision regarding what would be in P’s best interests.
These hearings are quite rare in the Court of Protection when compared to Child Care proceedings and are only implemented when ‘necessary and proportionate.’ In Nottingham City Council v SV & Anor [2025] EWCOP 37, Lieven J stated as follows:
55. The facts which are sought to be found must have a direct impact on the welfare decisions that need to be made in respect of P. The fact finding must be “necessary” for the determination of those welfare decisions. The fact finding exercise must be proportionate to the issues that need to be determined. In determining proportionality, the likely cost to public funds, the time taken and the impact of delay on P are all relevant considerations.
In that case, it was deemed that it was not necessary or proportionate for a Finding of Fact hearing to take place, as all parties (including P) were in agreement with a proposed plan involving a Contact Plan and a gradual build-up of contact. It was also noted that (1) P would be fully protected by this plan, (2) a hearing would take two days of ‘the very limited time available for Court of Protection hearingsat Tier 2 level,’ and (3) the cost to public funds would be ‘disproportionate’, given all parties were publicly funded.
P’s Representative
Where P is a party to the proceedings, P will have their own solicitor. If there is a paid advocate, Relevant Person’s Representative (RPR) or Independent Mental Capacity Advocate (IMCA), usually the solicitor is contacted and instructed by them, after consulting with P if appropriate. Alternatively, if proceedings are started and there is no person fulfilling the role of Litigation Friend, the Official Solicitor (an independent organisation whose role is solely to promote the best interests of vulnerable parties) will instruct a solicitor themselves.
P’s representative is not instructed by any of the public bodies or the care provider, and is able to raise queries, test assertions, and obtain disclosure. Any evidence is therefore tested and evaluated by a person who has no ties to the public bodies, as well as the Court.
Dependent on the nature of the proceedings (i.e. under which section of the Mental Capacity Act 2005 they have been issued), P may be entitled to non-means tested Legal Aid, regardless of their financial circumstances. In other situations, their eligibility may be dependent on their income, capital and assets.
P’s wishes and feelings are also incredibly important. The Court is able to override these wishes, but they will always be considered under s4(6) of the Mental Capacity Act 2005. P’s views will be obtained by their own representative who is appointed for this reason and they will file a statement setting out their experience and interactions with P. If relatives disagree that P’s views are truly as set out in the statement, they will be able to explain in witness evidence why they feel this and how the accuracy could be improved e.g. if the visit took place without an interpreter present, which resulted in a language barrier.
What families can do if they disagree with contact restrictions
If family members believe a restriction is not justified or is disproportionate, they can:
ask the placement to provide written reasons
ask that relevant records are disclosed
keep a record of visits and their impact
request that concerns are put before the Court for determination
make an application to the Court directly.
Family members are not entitled to see the records of any P who is an adult, regardless of their relationship to P, unless there is a Deputyship or Lasting Power of Attorney for Health & Welfare in place or P has capacity to consent to this. The person in the role of the Relevant Person’s Representative (RPR) is expected to review the Care Plans, but other records are protected. As above, the Court can order disclosure of these records.
If the matter is not before the Court of Protection already, then, subject to Court permission, family members who are not fulfilling the role of RPR, Deputy or Attorney can make applications – they’re not wholly dependent on waiting for the LA or others with formal roles to make an application.
Legal Aid may be available for family members in Court of Protection proceedings about contact and welfare, although this is subject to means testing and examination of the merits of the case.
Conclusion
Contact decisions are complex because P’s Article 8 rights must be balanced with their safety and often it is not entirely clear at the outset of proceedings what is in their best interests.
The Court’s role is to step in when there is disagreement, assess evidence, and determine what arrangements genuinely promote P’s welfare. Restrictions must be necessary, proportionate, and justified. Where they are not, the Court can (and does) refuse or remove them.
For many people, that question evokes an instant answer. The man at this centre of this case, A, is no different. For him, home is Spain, where he lived for approximately 33 years.
The problem is that he currently lives in a care home in Wales. Despite the fact that a circuit judge has found that A is habitually resident in Spain, and despite the fact that he clearly wants to return to Spain, that may not be an option for him.
Whether that’s an option, and how the legal complexities should be addressed, is an issue for Mrs Justice Morgan. On Tuesday 7 October 2025, I observed a remote directions hearing in this case (COP 20009483). Representing the local authority, Neath Port Talbot County Borough Council, was Victoria Butler-Cole KC. Representing A, via his litigation friend, was Ian Brownhill, who was also joined by Jake Thorold.
In this blog, I’ll explain the background to this case, and draw heavily on a previously published judgment in this case to explain what habitual residence means and why a judge concluded that A is habitually resident in Spain.
Next, I’ll explain some of the legal and practical complexities that Morgan J will need to deal with it at the next hearing.
Finally, I’ll share some personal reflections on what Morgan J described as “the well- recognised emotional human basic wish to go home”.
In this section, the references to other pieces of case law are lifted from the published judgment.
In his judgment, the judge explains that A was born in Wales but lived in Spain for approximately 33 years. He achieved residency there, which is due to expire in 2031. His wife, B, remains in Spain. His son, C, lives in South Wales.
In April 2024, C flew to Spain and A returned to Wales with him. C is unable to care for A at home, who now resides at D Care Home. He is unhappy there and wants to return to Spain.
The question for the court at this stage was to determine A’s habitual residence. At §8 of the judgment, the judge explains that “habitual residence is a question of fact to be determined by a wide range of circumstances of the particular case. It is not a legal concept”.
Knowles J, in Health Service Executive of Ireland v IM & Anor, set out seven key principles for determining habitual residence at §29 of her judgment. These principles include identifying the appropriate legal test as habitual residence being the “place which reflects some degree of integration by the child [and in this context adult] in a social and family environment”, the importance of the person’s state of mind, and the stability (rather than permanence) of the residence.
b)The expression “degree of integration” is an overarching summary or question rather than the sole, or even necessarily the primary factor in the determination of habitual residence. The court’s focus should not be narrowed to this issue alone as a question of fact [68] and [72].
Importantly, “the court must look not only at the terms of the authority conferred upon the person taking the decision [to move someone who lacks capacity] but also at their motives for taking that decision” (§32). In addition, the fact that the person thinks it is in P’s best interests “may not suffice to prevent the move from being wrongful”.
Schedule 3 of the Mental Capacity Act 2005only makes provision for the Court of Protection to exercise its power if an adult is habitually resident in England and Wales, if the adult has property there, the matter is urgent, or the protective measures are temporary or limited in effect to England and Wales. An adult will be treated as habitually resident in England and Wales if their habitual residence cannot be ascertained, they are a refugee, or they have been displaced as a result of disturbance in the country of his habitual residence.
Taken in the round, HHJ Richard Miller concluded that A’s habitual residence is in Spain (see §13 of the judgment). The judge considered that A did not have any intention to return to live in Wales when he had capacity, was integrated into life in Spain and had chosen to live there, he owned property in Spain, had a business and bank accounts in Spain, received healthcare in Spain, had obtained residency in Spain, and did not choose to leave Spain.
This meant that B and C “had no lawful authority to move A to Wales. He had refused to sign a lasting power of attorney […] His permanent removal from Spain was likely to be contrary to his wishes” (§14). However, and for the avoidance of doubt, “B and C did not act in bad faith” (§15).
In concluding the judgment, the judge commented that “consideration should be given to the appropriate Tier of judiciary to which this case should be allocated in future”.
Clearly consideration had been given to this because, when I observed the hearing in October, the case had been allocated to Mrs Justice Morgan (a Tier 3 judge).
2. The October hearing: Legal complexities and fitness to fly
Matters had moved on since the judgment. Counsel for the local authority told the court that enquiries have been made as to what options are available to A in Spain: “although he is said to be fit to fly with assistance there are no viable options from in Spain because he wouldn’t be able to afford privately funded care and the process for him to access publicly funded care is expensive …. It seems to us there isn’t any realistic way of him going back to Spain and unfortunately there aren’t any other care homes in the vicinity or close to his son. He is going to have to stay in his present care home even though he objects”.
This raises tricky technical and legal questions but, at this stage, the judge did not want to be side-tracked by this. She recalled a previous hearing (which I didn’t observe) in which the family had spoken about the situation in a “very affecting way….that is familiar to anyone in a family who found themselves navigating their way through inevitable deteriorating dementia…I would not want to be lost in what you [Counsel for the local authority] correctly identify as the technical and practical complexities.”
One of those complexities is under what legal mechanism the Court of Protection can authorise A’s deprivation of liberty in the care home. Another is that A has expressed a wish to go home to Spain but has also told his legal representatives that he does not want to return to Spain for an assessment or even to live in a care home. He wants to return to live at his previous home (somewhere that his wife told the court he has not lived for some years).
The judge was also keen to get into the issue of whether A is actually fit to fly. Counsel for A told the court that, “[C, A’s son] [says] his father can’t navigate through an airport, can’t navigate onto an aircraft…I think the medics have taken a narrow view on the concept of fitness [to fly] and one concern is the emotional impact of this man going onto an aircraft”. In other words, A may be medically fit to fly, but that doesn’t necessarily mean that the process of flying would be safe or in his best interests.
The judge therefore directed that further evidence about this matter be filed in time for a hearing in the first week of December. At this same hearing, the court will consider the legal complexities, and (hopefully) come to a conclusion as to A’s best interests.
3. The wish to go home
It seemed to me that this hearing was always intended to be a brief directions hearing. Indeed, given that the parties seemed to be in broad agreement as to the way forward, I got the impression that Morgan J had kept it in the list so she could reassure A’s wife and son that she was ‘keeping an eye on things’.
However, I was quite struck by the way that the judge addressed A’s expressed wish to go home. Here’s a brief exchange from my notes (we’re not allowed to record hearings so this is unlikely to be verbatim).
Judge: May I just ask you [Counsel for A] this. I don’t think I’m conscious of having seen a note of the visit yesterday. I wanted just to canvas this with you. The situation about wanting to go to Spain as expressed, and very firmly not wanting to go throughthe process of going to Spain for the purpose of being assessed for something that is not wanted – I put that inelegantly – is not a straightforward linear process for somebody whose thought processes, as I read the evidence, are affected by his illness. Are you able to help me with the link that [A] made in his head with the consequence of not wanting the process, if he still wanted the end result that is only possible by that process?
Counsel for A:My Lady I can’t and I don’t want to give evidence or offer a clinical opinion…I wonder whether it’s that straightforward desire to return home as we see so often in people with dementia. [A]’s home is Spain and I do wonder whether that’s at the core of what he’s saying…the level of his distress has not been as consistent but he has always been consistent about his wishes and feelings
Judge: And you’re not inviting me to make any further or other directions. I should safely treat it as the well-recognised emotional human basic wish to go home, in circumstances where home is understood and recognised as Spain?
Counsel for A: That’s right.
This has lingered in my mind far beyond the conclusion of the hearing.
What I mean when I say “home” can be contextual. When I was in Amsterdam for a few days in October, and I said at the end of our first day “let’s go home”, I didn’t mean back to the UK. I meant the apartment in which we were staying.
At the end of our visit, and when we were waiting in the airport, I said something like “I want to go home”. In that context, I did mean that I wanted to go back to the UK. In fact, I meant my own home, where I live. But as anybody who has ever flown into Manchester Airport will know, the process isn’t quite as fast as you’d hope, and getting to my own home was going to take some time.
This shifting meaning of home need not be contextual. I still refer to my parents’ house as home even though I haven’t lived there for years. In that instance, home isn’t the place that I live but a place with strong emotional connection (and I’m lucky enough that those emotions are positive ones).
If, hopefully a long time in the future, I find myself diagnosed with dementia and living in a care home, I rather suspect that any request to go home will have two meanings. In the first instance, it’ll probably mean wherever it is that I’ve made my home. But there’s a strong possibility that it’ll also mean my childhood home, where I lived for eighteen years, and where I first felt both physically and emotionally safe.
This strength of emotion has also been picked up on by the travel writer Jan Morris. At the very end of Trieste and the Meaning of Nowhere (my favourite of her prodigious output), she writes movingly about the places that have meant the most to her: “As for me, when my clock moves on for the last time, the angel having returned to Heaven, the angler having packed it in for the night and gone to the pub, I shall happily haunt the two places that have most happily haunted me. Most of the after-time I shall be wandering with my beloved along the banks of the Dwyfor; but now and then you may find me in a boat below the walls of Miramar, watching the nightingales swarm”.
Home is a physical place but can also be understood as a physical representation of emotion. In A Room of One’s own[ii], the political theorist Iris Marion Young makes the point explicit. Home, she says, is not just a place where we dwell “among things” but it is also a preservation of those things and those meanings. While it need not be a whole building (and here she was specifically concerned with nursing home) there is a need for “some individuated dwelling space […] a space in which one dwells among personally meaningful things”.
For many people with dementia, the emotional connection with home remains long after the dwindling of the memory that the physical space is no longer accessible. It can be distressing when care staff do not understand or are perceived of obstructing attempts to return to that place. But none of this changes the desire to be home, and none of this changes the possibility that the care home can become a place that one might see as home.
I know I’ll be unable to observe this hearing when it returns to court in the week commencing 1st December 2025. It sounds like A will not be able to go to the home he desires. But I do hope something can be done to turn wherever he is living into somewhere he might consider a home.
Daniel Clark is a member of the core team of the Open Justice Court of Protection Project. He is a PhD student in the Department of Politics & International Relations at the University of Sheffield. His research considers Iris Marion Young’s claim that older people are an oppressed social group. It is funded by WRoCAH. He is on LinkedIn, X @DanielClark132 and Bluesky @clarkdaniel.bsky.social.
[i]At §11 of HHJ Richard Miller’s judgment, this case is given the neutral citation number [2014] EWCOP 4. That is incorrect. The actual neutral citation number is [2014] EWCOP 43.
[ii]This is my favourite of Young’s essays, and in some ways can be seen as a continuation of House and Home (another essay by Young). Here she agrees with other feminist theorists that home is often constructed at women’s expense because of an expectation that they nurture the home so their children and husbands can develop their own goals and subjectivities. Home can also be a locus for violence. But she nevertheless disagrees that home cannot be a useful and meaningful concept. In both essays she suffuses philosophy with personal experience (in House and Home she discusses being removed from her mother’s care; in A Room of One’s Own she discusses her father-in-law’s move to a nursing home following a stroke).
The protected party (P) is a man with autism and a hoarding disorder. The Local Authority has deemed his property in need of urgent clearance and attempts to achieve this previously have not been successful because P has remained at the property and ‘progress was too slow to be meaningful. He resisted the removal of certain items and progress was extremely limited.’ At a hearing last month, the judge was asked to authorise P’s removal from his home – either by agreement or by force – to enable them to clear the property, assess the amount of work that is required to make the place habitable, and complete any necessary remedial works. At that hearing, the local authority made an application for a two-stage order: the first stage was for P to be “encouraged” to leave the property. Stage 2, contingent on Stage 1 being unsuccessful, was for authorisation of removal with restraint. The judge authorised only Stage 1 at the last hearing. (see Hoarding and best interests challenges for the Court of Protection by Claire Martin).
There was one feature of the 7th October 2025 hearing which was (intentionally) omitted in Claire Martin’s report of it and which we feel is important to report on now. There were actually two different versions of the judge’s order of 7th October 2025 – one for the public bodies (which referred to Stage 2) and one for P and his brother (which did not mention Stage 2). Both versions were discussed in a public hearing, and there was nothing in the Transparency Order preventing the observer from reporting this. Since the creation of two different versions of the order was clearly an attempt to withhold certain information from P (and his family), Claire (the observer) and Celia Kitzinger (the blog editor) decided together to wait until after P had moved – or been moved – out of his house to report on this. Celia says: “In effect, the court relied on us being responsible court reporters – but it would be wise to bear in mind in future that with an observer present in a public hearing, and no reporting restrictions to prevent disclosure, there is always a risk that information might be published and discovered by P and his family, contrary to the intentions of the court. I urge the court to amend the Transparency Order in cases like these”. She also comments: “I am not sure how the ‘two versions’ of the order really works in any event, given that orders from public hearings are themselves public documents (COP Rule 5.9). I would previously have advised family members that (unless they are specifically told otherwise) an order from a public hearing would be complete and accurate – but now I have to contemplate the possibility of redactions, even in orders from public hearings. I’m not sure this was properly thought through”.
Following the hearing observed by Claire, Stage 1 “persuasion” was attempted, but P refused to leave his home. Subsequently, Stage 2 was approved, on 14th October 2025 (we think without a publicly listed hearing). However, in the event, P left his home on the 20th October 2025 without the use of the authorised restraint plan.
The next hearing we saw publicly listed was on Monday 17th November 2025 (a bit sooner than had been anticipated, according to Claire Martin’s blog post). It was at 11am before Tribunal Judge Kaufman, and that is the one I observed and report on below.
Hearing of 17th November 2025
At the hearing, P was present, in the same room and on the same screen as counsel representing him (via the Official Solicitor), Mary-Rachel McCabe. The Local Authority (London Borough of Brent) was represented by Alexander Campbell. (P’s brother appeared not to be present at this hearing.)
For the benefit of those observing, the Local Authority provided an updated background since the previous hearing when the order for removal with restraint was approved.
On 20th October 2025, P moved out of his home without the use of restraint, and into a hotel in the local area (for the purposes of this post, let us call it Hotel A), which he was familiar with from a previous stay. This move had gone well – which, as the Judge clearly expressed toward the end of the hearing, was the result of the consideration and time put into the process in the previous two hearings.
However, the placement at Hotel A has had to come to an end. The reasons for this were not made entirely clear, the Local Authority referred only to ‘insurmountable logistical difficulties’ regarding payment.
As a result, P has had to move again, into another local hotel (I will call it Hotel B) at his own expense. The Local Authority has been searching for a suitable property since then and has now found a flat available for P’s use – but it is some distance away in another area of London. They have kitted this out with towels, pillows, a microwave and other items to make it habitable, and it has been available since 6th November 2025.
The Local Authority wants an order to move P into that flat, with the same transition plan in place as previously authorised. This includes the multi-stage order from verbal encouragement at first, progressing to restraint subsequently.
The Official Solicitor opposed this application as the flat is not in P’s local area, and he would find such a move destabilising. In addition, the property only has a shower, and P’s particular needs require use of a bath. Additionally, the Official Solicitor opposed the use of restraint for this move as disproportionate.
The Local Authority offered a number of arguments for why this move, although not ideal, would be in the best interests of P:
This accommodation is preferable to that of a hotel as it is more secure, particularly as P is currently self-funding at Hotel B. There is, therefore, a risk of a financial need to end the stay, or a risk that the property will become fully booked requiring P to leave at very short notice. At that stage and urgency, the Local Authority may find it difficult to find any suitable accommodation, or to purchase needed items to make the accommodation acceptable for P. The Local Authority is seeking more reliable accommodation.
There are also benefits to the specific property the LA has located. As a private dwelling, it is a more personal setting than that of a hotel. It will allow P to live independently as it has better facilities, such as a food preparation area and microwave.
If the Court agrees to order the move to the flat, the Local Authority will continue looking for a more suitable property in P’s local area. The Local Authority did recognise that for P it would be preferable to avoid multiple moves but stated that this is unavoidable as there is nothing better currently available.
The Judge asked Counsel to specifically address the evidence from the Mental Health NHS Trust (although not represented at this hearing, they were involved previously and both the Judge and Counsel for the Official Solicitor referred to and quoted from a written report provided by them) which stated that P’s specific needs meant moving out of the local area would be challenging.
LA: ‘If we had found somewhere in his local area, that would be what we were asking the Court to authorise today. But there was nothing suitable in the area. The evidence provided by the Trust recognises the benefits of P remaining in his local area, and whilst the Local Authority would not dispute these, the evidence does not suggest that living in a different part of London would be an absolute barrier to receiving the ongoing support and care. It may be more difficult but, in my submissions, those do not outweigh the benefits of more secure accommodation.’ [Counsel for the Local Authority]
The Local Authority emphasised that if P had to move out of Hotel B urgently, the accommodation found at that point may be even less convenient: this was a significant risk they wished to avoid.
Then the Official Solicitor provided the following reasons for why the move is unsuitable for P:
The primary reason is location. The property is a signficant distance from P’s local area. In fact, when looked up by the Official Solicitor, it is over an hour and 15 minutes on public transport – depending on the route – requiring two or three changes. P relies on local individuals, shopkeepers and his GP. He requires the stability brought by consistent routines. He has lived in the local area for most of his life.
Multiple moves are not advisable for P. Counsel for P stated: ‘P requires stability as much as is realistically possible. That position also reflects the conclusions of the doctor who diagnosed him, who stated a need for ‘scaffolding and structure.’ In other words, stability is important.’ The move from his home to Hotel A was possible due to his clear involvement in the process, careful planning and the fact the Hotel A was already known to him and in his local area. This is not true of the other property.
Additionally, whilst this is a less important factor, P has been unable to tolerate having a shower throughout his life and requires a bath.
The Official Solicitor recognised that asking the Court to effectively authorise the continued payment of Hotel B out of the pocket of P was an ‘unusual’ one, but pending the identification of more suitable accommodation, this was preferred. The Local Authority would then have to continue to search, and it was requested that the order include a particular responsibility of the Local Authority to update and communicate regularly with the Official Solicitor about available accommodation to ensure P could be involved in this process.
Additionally, the Official Solicitor was keen to request that restraint be removed from the order as an option for removal. The use of restraint had been discussed at length with regard to removing P from his own property urgently. However, Counsel described it as ‘disproportionate’ outside of that urgent and particularly difficult context. The proposed move from Hotel B is significantly different, and as it is a private hotel, there are some limits to the authority the secure ambulance service has to force entry, which had not been properly considered by the Local Authority.
Judgment
The Judge apologised to P for the disjointed and unsettled process of moving him out of his property. She expressed concern that these circumstances would not be putting him in a positive position to move forward from the clearance of his property. However, beyond answering yes or no to a question asked by the Judge regarding his planned attendance at an upcoming important appointment, P did not make any oral contributions expressing his own views at any point in the hearing.
The Judge also re-emphasised how unfortunate additional or gratuitous moves are for P and recognised that whilst hotel accommodation is deficient in many ways and it is concerning to think P will ‘remain in hotel accommodation for a long time’, the Local Authority plan itself involves possible further moves beyond the flat now under consideration, if a more suitable property is found.
The judge found, in conclusion, that the risks of residing in a hotel were not particularly weighty and she did not authorise the move to the property proposed by the Local Authority.
The Judge did order that the Local Authority file evidence about the continuing search for an appropriate property and must keep the Official Solicitor updated as to the efforts and outcomes of the search. This will be discussed at the next hearing.
Costs application against the Local Authority
Additionally, the Official Solicitor had made a costs application in the week prior to the hearing, for the costs arising from the additional work resulting from the failure of the placement at Hotel A.
Timelines for the Local Authority to respond to this cost application were set in the course of the hearing. The Local Authority wanted until the morning of Friday 21stNovember to respond to the application (over a week), on the basis that the individual who had received it was out of office at the time and their legal and social work teams were to be focused on finding accommodation for P. The Official Solicitor requested the Local Authority response and evidence at the end of the working day on Thursday 20th November. As stated by the Official Solicitor, these additional few hours would be important to ensuring they could respond fully. The Judge gave the Local Authority the timeline they requested, with the explicit direction that she did so to provide them additional time to make ‘extensive effort’ to find suitable local accommodation for P.
The application is set to be discussed in full at the next hearing, which was last confirmed to be listed for 11:00am on 25 November 2025.
Virginia Gough is a student at City Law School, currently studying the Bar Vocational Course following completion of the Graduate Diploma in Law. She is pursuing a practice in Family Law and Court of Protection. Her interest in mental capacity law and the specific challenges of advocacy for vulnerable individuals stems from her volunteer work as a Social Security Tribunal Representative, where she represents clients appealing decisions on disability benefits. She is a new contributor to the Open Justice Court of Protection Project, and this is her first blog post. You can connect with her on LinkedIn.
By Sandra and Joe Preston, Lorraine Currie, Alison Golding, Eleanor Tallon, Hilary Paxton, Mary Kadzirange, and Lucy Series (with an introduction by Daniel Clark), 21st November 2025
We’ll publish more about the case once the judgment is handed down, but that’s unlikely to be before early 2026 at least. While we wait, we thought it would be interesting to hear what people who had watched the live-stream or the recordings would decide if they were a Supreme Court judge. Shortly after the hearing, we issued an open call for contributions to answer that very question.
The answers we received to this question have been presented in no particular order, though I have tried to directly juxtapose responses that stand in contrast to one another. This approach brings to the fore how much variety there is. That’s to be expected because of the considerable diversity of people who have contributed. Where there are similarities, that’s entirely coincidental.
Open justice means that members of the public have access to courts and can watch hearings. That means the observers form opinions about what they see, opinions informed by their own unique expertise and knowledge base (professional and personal).
The question before the Supreme Court was whether the proposal from the Attorney General for Northern Ireland was compliant with the Strasbourg jurisprudence concerning the proper interpretation of Article 5 of the European Convention on Human Rights. For the most part, the contributors to this blog have chosen not to answer this question, and instead tend to focus on the broader issue of what they do (and don’t) want to change about DOLS.
First, Sandra and Joe Preston explain their view that the current approach to DOLS should change because, contrary to the view expressed by the Charities, repeated DOLS assessments are intrusive.
Second, Lorraine Currie says that she would “ease” the impact of Cheshire West but that, in her view, this ought to be done by a change to the Code of Practice rather than in the Act itself.
Third, Alison Golding engages in close interpretation of Article 5, and makes the case that there should be a high bar for assessing a person’s “contentment” with their living arrangements but a low bar for identifying an objection.
Fourth, Eleanor Tallon considers the Convention on the Rights of Persons with Disabilities. She thinks that the acid test should remain as-is but nevertheless thinks that the question of what being free (or not) to leave means in the context of the person living in their own private home or with family.
Fifth, Hilary Paxton considers the role of external scrutiny, with a particular focus on the role of visitors.
Sixth, Mary Kadzirange discusses the relationship between safeguarding and deprivations of liberty.
Seventh, Lucy Series reflects on the passage of time since the hearing in Cheshire West (which she observed). Ultimately, she thinks that the robust safeguards needed for valid consent should be provided through legislation.
1. DOLS and intrusive assessments
By Sandra and Joe Preston
Three charities (Mind, Mencap and the National Autistic Society) acted as interveners in the Supreme Court case, represented by Victoria Butler Cole KC. At one point, in response to the Secretary of State’s observation that families find repeated DOLS assessments intrusive, the advocate said that the charities she represents “had not found this to be an issue”. This has certainly been an issue for us.
Joe’s mother has Alzheimer’s. Until recently, she’s been living in a care home where she’s been safe, cared for and generally content. Some of her behaviour was treated as “objecting” including saying she wanted to go “home” (she meant to the town where she lived as a small child), and occasionally banging on windows and doors (out of frustration at having to wait for staff to escort her inside and out). We both believed her objections were to the situation she found herself in – with diminishing cognition, and she was generally happy. The only thing that caused her real distress was the Deprivation of Liberty process itself – when someone from the Supervisory Body took it upon themselves to interrogate her as to where she would like to live. This could unsettle her for days at a time.
The first DOLS authorisation was issued in May 2021, valid only for three months “to ascertain whether P’s behaviour constituted an active and consistent objection to her placement”. This was the beginning of a period of short-term DOLS assessments involving 23 visits from 16 different officials and a s.21A court hearing, before remaining in her placement was determined to be in her best interests. We wrote about this in our previous blog post (A court hearing and 23 visits from 16 officials: Family doubt that ‘Deprivation of liberty’ is working in the public interest). We hoped that, after this court hearing, and a carefully worded order from the judge, that would be an end to repeated and disruptive short-term DOLS assessments and authorisations for her. Sadly this was not to be.
Joe’s mum has recently been admitted to hospital following a series of falls and is still there as her previous care home would not have her back. The hospital brokerage team has finally identified a nursing home that will take her and provide 1:1 support which she is currently assessed as needing because of her falls risk, dementia and delirium. On the DOLS front, the one that was extended at the CoP in June is now void and the Court Order which refers to her former care home is not quite the document it was in June. The hospital has put their own DOLS in place to cover her lengthy stay there, and as soon as she is discharged to the new nursing home she will require another DOLS being authorised. She is being placed there under the D2A process, so possibly only for 4-6 weeks, but it is too soon to second guess whether she will then need another DOLS or not.
We are leaning towards the AGNI/DHSC view and would question whether those with advanced dementia are actually deprived of their liberty under Article 5 – surely it is their illness that has deprived them of their liberty and if they require 1:1 care to keep them safe from harm and have no alternatives but to live in nursing placements identified for them by an Integrated Care Board do they need as many authorisations as Joe’s mum is now facing? She finds them distressing and intrusive, and as for us, we certainly don’t want our last days/weeks/months together taken up with DOLS bureaucracy, but instead to spend what precious time we may have left with her at the end of her life. In our view, DOLS for Joe’s mum is not just a waste of public money, it also actively causes harm and diminishes the quality of our family life.
Joe and Sandra Preston are the son and daughter-in-law of a P who was involved in Court of Protection proceedings. They can be contacted through the project email on openjustice@yahoo.com.
2. “I do not see how I could reach a decision”
By Lorraine Currie
I’ve been asked the question what would I decide to do if I was a Supreme Court judge in the Northern Ireland reference about valid consent.
From observation of the hearings, and putting myself in their shoes, rather than my own, I simply wouldn’t have enough information on which to decide anything. So many options were presented beyond the original reference e.g. Cheshire West was re-examined but not in any great detail, the question of valid consent inferred by the persons wishes and feelings was discussed, but so many relevant players were not represented. We heard nothing from the Dementia charities, we heard nothing from the likes of Social Care futures or a Gloriously Ordinary life who may have had a different take. We didn’t hear actual case studies of those negatively impacted by the repetition of DoLS and we didn’t hear from local Councils or DoLS Leads who could explain the burden of DoLS not only on systems but on the people at the heart.
Without a full and complete re-examination of DoLS in 2025 I do not see how I would reach a decision.
I sense that some of the Judges were definitely inclined to limit the impact of Cheshire West whilst others were totally oblivious to its reach and I would be one of those who would like to limit its reach.
I would probably allow the interpretation as requested by the Attorney General for Northern Ireland but in doing so, by in fact allowing a policy change in the Code not in the Act, I would be fully aware that this would open the doors to further challenges reaching the Supreme Court in regard to this interpretation.
I would also be concerned that (as a Judge) I would have no role in ensuring the necessary safeguards were in place. I would however see this as an opportunity to promote rights but I would then want to be fully involved in setting up a system of safeguards (in my normal role). It then might be that the easing of Cheshire West offered by the interpretation actually results in a second parallel and complex process of alternate safeguards.
Lorraine Currie is now a freelance Mental Capacity Consultant. She has over 30 years Local Authority experience, is a qualified social worker and in 2021 received the LGC Award for Outstanding Individual Contribution. Lorraine provides extensive training and is an Associate for the West Midlands Association of Directors of Adult Social Services (WMADASS) working on DoLS. Lorraine is on Bluesky as @lorrainecurrie.bsky.social.
3. Interpreting Article5
by Alison Golding
Firstly, Article 5(1)(e) does not apply to a person who is unable to make any expression of wishes through any means, such as a person in a persistent vegetative state, as their situation does not reach the criteria set out in the universal test in Guzzardi for there to be a deprivation of liberty: the tests in Guzzardi depend on the recognition by the subject that they have, even if only at a most minimal level, either bodily autonomy or the right of bodily autonomy. (Only a mental element is relevant here: a person with e.g. locked-in syndrome who is able to communicate has the ability to recognise and consent or object to their living circumstances and so be subject to restraint.)
Secondly, Article 5(1)(e) only applies if a person is “of unsound mind”: a person who has legal capacity to consent, or not to consent, to their living arrangements is not of unsound mind for the. purposes of Article 5(1)(e). This analysis explains Storck, Stanev and Mihailovs: a valid refusal or lack of consent excludes any lawful power for national authorities to confine in accordance with Article 5(1)(e), confirmed by the use by ECtHR of the legal term “consent”.
The test for whether a person can validly grant or refusal consent so as to take them outside the scope of Article 5(1)(e) is separate from a general test as to whether a person is “of unsound mind”, and depends on that person’s living arrangements and on whether they are consenting or refusing. A child living at home with caring parents, on reaching adulthood, may be able to relatively easily express by their manner and expressions that they are validly consenting to that arrangement. (In Cheshire West, the manner and expressions of MIG, living contentedly in the closest available arrangement to a caring parental home, might be taken to meet this standard.) The barrier for a person in an institutional arrangement expressing contentment to that arrangement is likely to be subject to a higher barrier for that expression to be treated as consent, and the barrier for their expression of objection to be valid lower.
Where the above analysis leads to a person not being within the safeguards of Article 5(1)(e):
(a) they are protected from DOL by the application to them of the safeguards of Article 5 as a whole,
(b) they still have the benefit of the protections in Articles 2 to 4 and 6 to 12, for which national protections other than DOL procedures may be required.
Alison Golding qualified as a Solicitor in local government. She then worked as a legal adviser in various UK Government Departments for 25 years until early retirement.
4. Valid Consent to Confinement through Wishes and Feelings: What Would You Decide?
By Eleanor Tallon
The requirement to provide information to enable a person to make an informed decision is a definitive characteristic of consent. The person’s right to withdraw consent without adverse consequences is another key factor. Therefore, my initial concern would be that changing the meaning of valid consent (in the context of confinement) risks placing health and social care providers in a state of uncertainty about the meaning of consent.
This could also erode responsibilities to support decision-making and gain informed consent for care and treatment. Further complexities, against a backdrop of uncertainties and misapplication of the MCA and DoL processes, would not be helpful.
The Attorney General claims that accepting positive wishes and feelings as valid consent would support the principle of Article 12, Convention on the Rights of Persons with Disabilities (CRPD), the right to enjoy legal capacity on an equal basis. Yet, the person’s wishes and feelings would only be accepted as valid consent if they agree to the arrangements. If the person subsequently objects, they would not be free to withdraw consent; they would remain objectively confined and deprived of their liberty.
To truly promote legal capacity, the person’s will and preferences would determine the decision, as far as that is practically achievable. This would apply in all areas of the person’s life so that their home and daily experiences reflect who they are and what they want, regardless of decision-making capacity. It’s not about constructing a fantasy that the person has legal agency to consent to their confinement, while removing that as soon as the person acts in opposition to those who really hold the power.
While I absolutely support the aim to embed the CRPD on the domestic level, it seems to me that this can be done in more effective ways than changing the definition of valid consent to confinement, such as through legislative reform, and incorporating human rights into practice cultures (focusing on the Reach Standards, Social Care Future and Gloriously Ordinary Lives as guiding initiatives is a good starting point).
Secondly, I would question how valid consent to confinement can be given by wishes and feelings. The person’s happiness in relation to their confinement would be difficult to quantify, and there are real risks of misinterpretation, susceptibility, coercion, and misrepresentation by those responsible for the person’s care. If the safeguards are removed because the person is deemed to be ‘happy’, as it stands, there is no clarity on what alternative safeguards would be available and no guarantee that the individual’s right to liberty would be protected by any other means.
It is not uncommon for the presumption of capacity to be used defensively by services and professionals to divert responsibilities. Similarly, the person’s proclaimed ‘happiness’ could be used as a mechanism to avoid the additional administrative and resource burdens for providers and authorities, which are warranted when the person meets the threshold for Deprivation of Liberty (DoL).
In terms of the acid test for confinement, as defined in the ‘Cheshire West’ judgment (2014), I would advocate that this remains. It provides clarity for care providers when identifying a confinement. If both arms of the acid test are met and there is no valid consent, this would trigger a referral for assessment under DoLS or the judicial authorisation process. A more nuanced evaluation will then be carried out by the Best Interest Assessor or the Court of Protection, while considering the concrete factors outlined in Guzzardi v Italy (1980) to establish whether a person is objectively confined.
However, I would urge more consideration around the second arm of the acid test, which is often misinterpreted. Not being free to leave is conflated with restrictions on leaving in the immediate sense (i.e., locked doors). Yet such restrictions would fall within the scope of continuous supervision and control. The relevant question to determine the second arm of the acid test is whether the person is unable to leave permanently, to live elsewhere.
Often, care arrangements within institutional-type settings will satisfy the objective test for confinement. Many people in care homes or hospitals are not free to live elsewhere because their care and residence are inextricable. If that is considered the legitimate, least restrictive option to meet their needs, then it can be deduced that they are not free to leave. Yet there needs to be a comprehensive appraisal of whether a person who lives in their own private home or with family is not free to live elsewhere. This type of scenario is the most disconcerting when considering the acid test for confinement, and I think it’s worth more thought around what being free to leave means in these contexts.
Eleanor Tallon is an Independent Social Worker, Expert Witness, and Best Interests Assessor. Eleanor is also an ESRC-funded Doctoral Training Pathway (DTP) student at the University of Birmingham. Her research focuses on the application of the Mental Capacity Act (2005) in private brain injury case management. Eleanor can be contacted via email eleanor@mcaprofessional.co.uk or through her website mcaprofessional.co.uk and found on LinkedIn or X(Twitter) @Eleanor_Tallon and Bluesky @eleanor24.bsky.social.
5.Looking forward to LPS
By Hilary Paxton
Where care and support works best, the provider would not be acting unilaterally. Any arrangements should be part of a care and support plan and be developed in the best interests of the person, based on a needs assessment and their preferred outcomes, and their wishes and feelings on how best to achieve the outcomes.
Whilst LPS is not yet in place and may be subject to further development, I support its aim to embed consideration of liberty and any arrangements that might affect it within a well-thought through response to needs etc. We will of course have debates about skill levels and capacity, but that aim should mean that the provider is only one agent in all this. This is about promoting wellbeing, including the prevention of abuse and neglect. External scrutiny is crucial to ensure there is then no abuse of power by an organisation or individual staff. External visitors (family, advocates, other professionals, clergy, visitors with pat dogs, theatre groups, singers, etc) to settings where care and support are provided all have a part to play to speak up if they see anything that appears untoward. This is not limited to people who may have an authorised deprivation of liberty. It is particularly important for people who do not have any visitors.
We of course, want to get the DoLS and the Court of Protection authorisation bit right, but this is only part of the story for people affected.
Hilary Paxton is a senior advisor at the Local Government Association.
6. Reflections on the post-Cheshire West landscape
By Mary Kadzirange
UKSC/2025/0042 has profoundly underscored the difficult and often uncomfortable tension that persists in the post-Cheshire West landscape. Whilst Cheshire West was grounded in the protective intent of Article 5 of the European Convention on Human Rights (ECHR), seeking to safeguard individuals from arbitrary deprivation of liberty, it has simultaneously placed professionals, families, and the state in an enduring ethical and practical dilemma. It sharpened the focus on protecting vulnerable individuals, yet in doing so, it expanded the scope of what constitutes a deprivation of liberty to such an extent that the boundary between necessary protection and unjustified restriction has become increasingly blurred. This tension is not merely theoretical; it is felt daily by practitioners striving to uphold both autonomy and safety, often within complex and emotionally charged situations.
AGNI highlights the continuing struggle to draw principled and workable boundaries between the state’s duty to protect and the individual’s right to self-determination, privacy, and family life. It raises difficult questions about what true liberty means for people living in care settings, and whether the systems designed to safeguard them have become too rigid or bureaucratic to respond compassionately and proportionately to real-life circumstances.
In practice, the challenge is striking a balance that neither leaves people unprotected nor subjects them to unnecessary intrusion or control. Safeguarding systems must evolve beyond compliance and formality to reflect nuanced human realities. If deprivations of liberty within homes or community settings are not properly authorised, people remain vulnerable; yet excessively procedural approaches risk alienating families and exhausting professional goodwill. Perhaps the path forward lies in proportionate reform, that ensures flexibility, transparency, and humanity, guided by holistic person-centred safeguarding legislation and processes that are further informed by future judicial clarifications, such as the anticipated 2025 Supreme Court deliberations, to recalibrate the delicate equilibrium between autonomy, protection, and proportionality.
Mary Kadzirange is a Registered Mental Health Nurse and a practising Best Interests Assessor She is the Mental Capacity Act lead within West Yorkshire Integrated Care Board’s safeguarding team, and is also Chair of the West Yorkshire ICB Race Equality Network.
7.Being careful what you wish for
By Lucy Series
Twelve years ago, on a grey October day in 2013, I listened to the first day of the Cheshire West Supreme Court and hearing (P (by his litigation friend the Official Solicitor) v Cheshire West and Chester Council & Anor). The courtroom was full of familiar faces from the world of the Mental Capacity Act 2005. The hearing was, as a barrister later commented, like a seminar with the brightest minds on one of the most challenging questions in mental capacity law: when is a person, who is not confined in a traditional ‘institution’, deprived of their liberty?
I enjoyed watching Lady Hale interject to correct barristers when they had misunderstood some aspects of mental capacity law and the underlying issues. I enjoyed conversations in the lunch break about what would convince the court that the current situation was untenable, that it was unacceptable that a man who had broken down the door of his care home to try and escape it, a woman who had capacity and was asking to live in her own home, and people like MEG and P in Cheshire West, who were being physically restrained and given sedating medications, were not considered deprived of their liberty when their behaviours indicated they were resisting aspects of their care.
Five months later I sat in my office with my friend and colleague at Cardiff University, Professor Phil Fennell[i], reading the Supreme Court’s judgment. We read Lady Hale’s ‘acid test’ of deprivation of liberty: a person is deprived of their liberty if they are subject to continuous supervision and control, and they are not free to leave, regardless of whether it is ‘normal’ for a person with their disability, or whether it is in their ‘best interests’. ‘A gilded cage is still a cage’. Deprivation of liberty must have the same meaning for a disabled person as a person without a disability, because this is the essence of universal human rights. To say otherwise would be to discriminate and deny safeguards that others would be entitled to in their situation. Phil turned to me and said ‘it’s a case of be careful what you wish for’.
Phil has always been wiser than me. This is what I wished for, more or less. I had worked in the kinds of places that P and MEG were being cared for, and some of what I saw was horrifying. I worked with an autistic man with learning disabilities, whose carers took him for walks with a rope around his waist – yet there seemed to be no ‘alarm bell’ that we could ring. The regulator had brought it up in reports, his social worker must have known, and yet it continued. People were confined to their rooms. Sedation, restraint and violence were routine, and went both ways between staff and residents, and between some of the residents themselves. Many residents seemed unhappy, even if they could not clearly articulate this because they did not use words to communicate. Not everywhere was like this, but when I read about P and MEG, this resonated.
So, what did I wish for when the Supreme Court revisited Cheshire West in Re Attorney General’s Reference? That the justices would have the level of understanding of mental capacity law, of the realities of social care, and the egalitarian human rights values that Lady Hale and other justices brought to Cheshire West. I would say that what I saw of the hearing – the first day, online – did not fill me confidence that this is the case. I feel quite worried, if I am honest, about how this will end. I was part of a brilliant WhatsApp group organised by the Court of Protection Open Justice Project – we watched the hearing together and have continued to discuss it. We share an anxiety that this ruling will leave people without the meagre safeguards the law currently entitles them to. Safeguards against inappropriate placements, excessively restrictive practices within settings, measures that restrict the rights and freedoms people could and should be entitled to. And anxiety about the way these populations were being constructed in some comments – not as bearers of rights, but as populations without the capacity for rights.
In the best-case scenario, what would I wish for? I stand by what I wrote (summarised here) that if we take seriously that people have a will, a meaningful subjective experience of the world, then this should be able to make a difference in terms of whether they are categorised as deprived of their liberty or not. The very concept of liberty only makes sense for beings with a ‘will’ – we don’t speak of depriving a rock, or a table or a teapot of their liberty.
I do not agree with the submissions from the Department of Health and Social Care that their subjective perspective is part of the ‘objective’ limb of deprivation of liberty. Logically, subjective experience must go to the subjective aspect of deprivation of liberty, because it is subjective. Objective is what is going on around the person, subjective is what is going on for them.
It is the subjective element that transforms confinement into deprivation of liberty. In everyday life people agree to things that could otherwise objectively amount to a deprivation of liberty, from the mundane (getting on a train, when you can’t get off until the next stop) to the experiences where the point is to be locked in (Escape Rooms). But they are not detained: they have consented.
I think the law should recognise that in some cases people’s subjective experience is of living in the place where they want to live, and being happy with their care arrangements (including any restrictions or supervision to keep them safe). This seems to have been the case for MIG, and for some others caught up under the ‘deprivation of liberty’ label at the moment. I believe we should create a legal framework that can recognise this as a legally valid consent for the purposes of Article 5 ECHR. If we do not, we risk reinforcing the same ableist stereotypes that allow others to say that ‘these people have no will, and therefore no liberty to lose’.
My biggest fear, however, is that ‘valid consent’ will be used as a shortcut, to avoid ‘formal’ assessments and independent checks on the person’s situation. One way this might happen is by treating subjective experience as part of the ‘objective’ limb of article 5. Care providers could treat someone nodding off in an armchair under heavy sedation, or someone cowed and institutionalised, as ‘happy’, and there would be no requirement to submit that judgement for external scrutiny. Nobody would check in on that, and the person and their family may not have the resources afforded by Article 5 to challenge this. That would be worse than where we are now. It would also insert new interpretive chaos into the system, we will be back to the days of councils having different rates of DoLS applications by several orders of magnitude.
Because of the weighty issues at stake here – the right to liberty – and because these are populations whose will is sometimes unclear or contested, there needs to be robust safeguards around valid consent in connection with article 5. My preference is that the Supreme Court says that these safeguards could only be provided through legislation (primary or secondary), properly developed and consulted on with stakeholders. That where a person lacks capacity there needs to be a robust regulatory framework for consent to be valid.
This reflects the requirements of article 12 of the UN Convention on the Rights of Persons with Disabilities, which recognises that everyone – no matter what their ‘mental capacity’ – should be supported and enabled to exercise legal capacity (make legally valid decisions). However, Article 12(4) also says that this must be subject to ‘appropriate and effective safeguards to prevent abuse in accordance with international human rights law… [ensuring] that measures relating to the exercise of legal capacity respect the rights, will and preferences of the person, are free of conflict of interest and undue influence, are proportional and tailored to the person’s circumstances’.
My view is that safeguards for valid consent should – at a minimum – require consultation with the person, and those who know the person well, and there should be a layer of independent oversight and regular review. It will require robust guidance on factors and indicators that preclude valid consent being given (e.g. restraint and sedation as part of care planning, guidance on how to interpret ‘challenging behaviours’). This could (I think) easily be built into the LPS processes and a revised Code of Practice. The system – after all – is supposed to be about protecting liberty, not just authorising taking it away.
Lucy Series is an Associate Professor in the School for Policy Studies at the University of Bristol. She researches and teaches mental capacity, disability rights and adult social care law and policy. She blogs at The Small Places. You can read her book – Deprivation of Liberty in the Shadows of the Institution – free of charge here (hyperlinked) or on Kindle. She is on Bluesky @thesmallplaces.bsky.social.
[i]Professor Phil Fennell is now an Emeritus Professor at Cardiff University. Before retirement he was a Professor of Mental Health Law. We worked together on a Nuffield funded research project on welfare cases in the Court of Protection. He is the author of Treatment Without Consent.