Other experts who have contributed to this Project’s discussion of the Court of Protection case of An Expectant Mother[2021] EWCOP 33 are not alone in the misunderstanding of the data surrounding home births. This is largely due to the fact that the presentation of the data is influenced by underlying beliefs of those presenting it. There are very few good trials into home birth and the cohort trials are from different parts of the world and not necessarily well controlled or detailed in their information. The meta-analyses are therefore flawed due to the mixture of the case cohorts included as well as coming from different clinical backgrounds.
It is often stated that home birth is safe for the low-risk woman. No birth is safe: safety is not binary, it is a continuum, and it changes over time. Risk is poorly assessed in most cases and is assessed as higher or lower depending on your starting point and your own beliefs. None of us is impartial.
When considering home birth, there are four things to consider:
the underlying risk and the awareness that this may change
the environment where the birth will take place
the difficulties in transferring a woman to hospital if required
the wishes of the mother.
Fundamentally, it is the mother’s decision after she has had fully informative information to help her decide. If a woman with the mental capacity to do so decides on a home birth, then irrespective of the hospital staff views or feelings, there is an obligation to support this and provide midwifery input.
I obviously cannot discuss the specifics of this case, in which I gave expert evidence, but it is fair to say that there were some concerns about obstetric risks to the baby but the emphasis of concerns was on the ability to transfer to hospital. This centred around the mother’s agoraphobia, and the effect it may have on her decision making.
The risks of an incident occurring for any individual birthing at home are not different from the risks of birthing in hospital, apart from the ability to monitor the mother and baby if there are concerns and the ability to transfer if required. So is not the home birth that is the problem, it is what you can do if something goes wrong. In many instances babies are lost or damaged during home birth due to slowness to observe deterioration, slowness to escalate and transfer to allow “rescue” to take place.
The best UK figures on home birth are published here and are used by the NHS website:
For transfers in labour or in the postnatal period, the study showed that 45% of primigravida are transferred: 35% before delivery and 8.9% after. For multiparous women the figures are 6.4% transferred before delivery and 5.2% after delivery. The figures were not much different for women giving birth in Freestanding Units or Alongside Midwifery Units, demonstrating the risk is not home birth per se but primigravida pregnancy. Many of the figures quoted by supporters of home birth do not differentiate between woman having their first baby at home and those having their second or more baby at home. That is why transfer figures are usually quoted as being a lot lower.
Half of the reasons for transfer was failure to progress (17.9 of the 35.1%), then fetal concerns (8.2 of the 35.1%), desired pain relief (2.8 of the 35.1%) and other concerns. After delivery, the reasons were requirement of suturing the perineum (4.4 of the 8.9%), haemorrhage or retained placenta (3 of the 8.9%), baby reasons (0.9 of the 8.9%) and other concerns.
Although emergency (urgent) ambulances were called in 11.5% of all primigravida, a “blue light ambulance” was probably needed in only 1% (my guestimate). The transfer times from decision to transfer to arrival in the obstetric unit was around 49 minutes on average.
The primary perinatal outcome was a composite of perinatal mortality and specific neonatal morbidities: stillbirth after the start of care in labour, early neonatal death, neonatal encephalopathy, meconium aspiration syndrome, brachial plexus injury, fractured humerus, and fractured clavicle. This composite measure was designed to capture outcomes that may be related to the quality of intrapartum care, including morbidities associated with intrapartum asphyxia and birth trauma.
The study showed that when correcting for pre-existing risk, primigravida had a 2.8 increased odds ratio of poor baby outcome (9.5/1000 or 1/100) compared with hospital birth 3.5/1000 or 1/300). This is largely due to the time taken to escalate the problem and transfer the mother. These figures are slightly worse than those quoted in court which were the unadjusted figures.
This is the basis of the figures I used in my evidence as they are the best that are available for the UK and would be relevant in this case.
To emphasise, the risks of home birth is not related to the incidents that occur but to the ability to transfer and rescue.
James Walker is Emeritus Professor in the Department of Obstetrics and Gynaecology at Leeds University and author of Planned home birth. Best Pract Res Clin Obstet Gynaecol, 2017.
“It was on display in the bottom of a locked filing cabinet stuck in a disused lavatory with a sign on the door saying ‘Beware of the Leopard.’”
So reads the infamous line from The Hitchhiker’s Guide to the Galaxy to justify the assertion that the all-important plans had indeed been on public display. I was reminded of this quote as I was traipsing around the Royal Courts of Justice looking for a Committal Hearing that purported to be held in public earlier today.
The proceedings had been advertised by the Open Justice Court of Protection Project, which advocates for public observation and scrutiny of the Court of Protection. Once described in 2006 as ‘shadowy’ and ‘the most secretive court in Britain’ by The Telegraph, great efforts have been made by the group to encourage members of the public (including health and social care professionals, law students, disability rights activists, academics, and families caught up in COP proceedings themselves) to witness and report on what they see.
What caught my eye was that this was a Committal hearing, proceedings described by Macdonald J as ‘essentially criminal in nature’ (Para 9) which can lead to the imprisonment of the alleged contemnor – a serious exercise of power by the court and worthy of public scrutiny.
The general rule as laid out in the Practice Direction on Committal for Contempt of Court in Open Court (“PD’s”) states at 5(1): “All committal hearings, whether on application or otherwise and whether for contempt in the face of the court or any other form of contempt, shall be listed and heard in public.
Such is the importance of Open Justice to this exercise of power that whilst the court does have Jurisdiction to sit in private, at the conclusion of a successful committal application the court must sit in public and give its reasons (PD’s at Para 13(1)). Para 13(2) states in no uncertain terms:
“There are no exceptions to these requirements. There are never any circumstances in which any one may be committed to custody or made subject to a suspended committal order without these matters being stated by the court sitting in public.“
The cause list showed this hearing as being held over MS Teams. However it transpired that it was in fact ‘attended’ and the parties would be sitting in court at 2pm. With that knowledge in mind, I doffed my face mask and made my way to Central London.
Unfortunately, upon arrival, the printed cause list on display at the RCJ still showed the case as being heard online. I enquired at the aptly named enquiries desk and was given a phone number for the Family Division who I was assured would assist me with my request. My phone tells me that the number was called a total of 8 times, going to voicemail after ringing out. Re-enquiring at the enquiries desk led to the advice “They’re normally held in the Queens Building”… and off I went.
Arriving there I was very conscious of the time. 13.58. Two minutes before I’d miss the start. I could see Court 40 was sitting, could this be the one? I peeked through the glass window on the door and googled the judge I was expecting (Hayden, J) so I could find an image to compare. No, not him.
I took the lift to floor 1M and enquired at my second enquiry desk of the day. “I’m here to observe the following case” I said handing over my notebook with the case number written on it. A few moments passed while she tapped at her computer – “Yes this one’s being heard on MS teams” she said. Ah. I explained the situation and she disappeared round the corner to seek advice. I look at my watch. The seconds are ticking by. She reappears. “Court 45 on Level 1”. I get back in the lift.
One final hurdle of the day – no, not a sign saying “Beware of the Leopard”, but one equally off-putting fixed within a permanent Perspex plaque.
“NO ENTRY TO THE PUBLIC SAVE FOR ACCREDITED PRESS/MEDIA REPRESENTATIVES”
With mortifying visions of proceedings being halted whilst I’m ejected, I catch the usher’s eye through the door and was helpfully directed to the public gallery at the back of the court.
The time was 14.07. The first time I have ever been late to a hearing.
I had as it turns out arrived at the half-way point – it finished some 8-minutes later.
“The threat of committal had achieved its objectives” said Mr Justice Hayden, describing it “as absolutely the last resort”. I had heard enough over the remaining eight minutes to speculate what may have occurred but certainly not enough to satisfy the requirements that reports should be accurate and fair.
An inaccurate cause list, two enquiry desks, a phone that never answered and a sign that said No Entry. I wonder if Arthur Dent would have been impressed?
Daniel Cloake is a blogger and news gatherer with a keen interest in law and the justice system. This post was originally published on his own site, “The Mouse in the Courtroom” (where you can read his many other blog posts). He tweets @MouseInTheCourt
Image by Dennis van Zuijlekom from Ermelo, The Netherlands, CC BY-SA 2.0, via Wikimedia Commons
By Katharine Shipley, 8th June 2021 (with additional material from P’s mother via Celia Kitzinger)
Editorial Note: A published judgment should appear on BAILII in the near future and we will link to it from this blog post when it does.
This three-day hearing (COP 13401563, before HHJ Tindal in Worcester) concerns a woman in her late thirties (“NW”), who has profound learning disabilities, severely restricted mobility and complex physical health needs, including epilepsy. The issue before the court is whether it is in her best interests to continue to live in a care home or to return home to her mother.
There were two previous hearings about this case that I did not observe. NW’s mother has written about them in her own blog post. She also contributed her views to this blog (via conversations with Celia Kitzinger).
I was drawn to this hearing for several reasons, not least because Celia Kitzinger tweeted that NW’s mother would welcome observers in the case. A previous case I observed concerned a woman who most definitely did not want observers to be present:
I managed to observe the majority of the three-day hearing. At the end of the hearing, I requested and received the position statements, transparency order and final order from HHJ Tindal.
Background
NW was adopted as a baby and lived with her adoptive mother until 2017 when she was admitted to a specialised care home (pseudonymised here as Dover House). This was initially for respite, when her mother was admitted to hospital.
When her mother was discharged from hospital a couple of months later, the CCG assessed that NW lacked capacity to decide where to live (capacity is not disputed) and that it was in her best interests to remain at Dover house, where she has been ever since.
The care home is in a different county, around 2 hours travel from her mother’s home and there have been practical (and other) difficulties with contact between mother and daughter. At the time of the hearing there had only been seven visits over the last three years and six months, the first in September 2020, the remaining six since 26th March 2021.
In February 2019, NW’s mother applied under s.21A of the Mental Capacity Act 2005 to challenge the Deprivation of Liberty (DOLS) standard authorisation and the case originally came before Judge Plunkett in November 2019 (see the mother’s blog post referring to this hearing). It is unclear what happened at that hearing, or why matters were then delayed until November 2020 – “covid intervened” says HHJ Tindal in his judgment.
In November 2020, there was supposed to be a three-day hearing. This didn’t happen. Although NW’s mother went to the courthouse and was there for the whole of what was supposed to be the first day of the hearing, what actually happened that day was a complete mystery to her (see her blog post).
According to the position statement from the CCG, the November 2020 hearing was adjourned to enable contact between mother and daughter. The court’s order set out recitals that it was lawful under the relevant COVID-19 regulations for that contact to take place, and outlined how it would be arranged. The order made s.15 declarations that NW lacked capacity to make decisions about litigation, residence, care and contact and provided an expert report on her communication abilities, and an interim declaration that it was in NW’s best interests to have contact with her mother – in the care home, in the community and at the family home. It seems that at that point HHJ Tindal was keen to see if a ‘third option’ could be found, whereby NW would remain a care home resident but have overnight visits to her mother.
The issue at this hearing was (still) whether NW should remain in Dover House, which is what the CCG (who fund her care) argued, supported by the local authority, or whether she should return home, which is what her mother wants.
The parties
NW’s mother was the applicant, as a litigant in person. She told us that about 2-3 weeks before the hearing, her legal aid team had told her they would no longer be working on the case. “I immediately set about seeking a practice that would accept the case, but following 70 – 100 enquiries in that short time I failed.” She represented herself in court but was supported by written submissions by Victoria Butler-Cole QC, provided pro bono. (“Victoria phoned me on a Friday evening and worked on my submission on the Saturday and Sunday”, she told Celia Kitzinger in a phone conversation after the hearing. “It was absolutely more than wonderful and something I will remember to the end of my life.”)
NW was represented (via her litigation friend the Official Solicitor) by Grainne Mellon. The Clinical Commissioning Group was represented by Rosie Scott and the County Council by Michael Paget.
My impressions of the process
This hearing was ‘hybrid’, meaning that some of the people were physically present in court (including NW’s mother) and others were on video link. From an observer’s point of view, I felt the format worked well (with the inevitable odd technical hitch). It seemed a good compromise, neatly reflecting this period where we appear to have one foot in the pandemic, one foot out. I’m sure for some witnesses, providing evidence by video link is a far more practical option and maybe hybrid hearings will become more commonplace – though it is concerning to know that in one recent case observers were excluded from attending a hybrid hearing via video link and were only permitted to attend in person.
Early on the first day, remote observers did have difficulty hearing the first witness, due to the noise of the judge typing near the microphone. This was quite swiftly resolved by the court clerk after observers raised the issue via the video link chat function. I did also have some difficulty working out who was who, particularly those who were physically in court, but I think this was largely down to my limited experience of the legal arena, and I learned some lessons for next time!
From the outset, HHJ Tindal came across as warm and sensitive, immediately addressing NW’s mother in a down-to-earth manner. He told her that there were observers, explaining to her that ordinarily COP proceedings are held in private because important decisions were being made about vulnerable people, but a balance between privacy and confidentiality is required (although his explanation did not quite reflect the situation as I understand it, e.g. as explicated here). In any event, she readily agreed to having observers present.
I felt that HHJ Tindal struck an excellent balance between allowing witnesses time and freedom to give evidence and parties to ask questions; and steering and refocussing the process. At times when things looked like they might derail, he quickly suggested a break in proceedings so that an advocate could re-evaluate their line of questioning.
How NW’s mother experienced the process (as told to Celia Kitzinger)
At least this time on Court morning I was prepared for the entrance security measures. Last time I had been confused and uncertain by the expectations on arrival and the lack of any guidance.
I was intentionally early and when the others arrived, we all went down to small rooms where I sat alone while they each prepared.
A member of court staff came to me and made herself known as a court clerk. She was part of the court hearing throughout and always kept a kindly eye on me.
The barrister for the Official Solicitor came to see me to reassure me that no-one was preparing to act unpleasantly to me in court and that I should ask for help at any time.
We were called to enter the court and to arrange our seating Covid style. To my horror I was placed alone in the front row, on something like a church pew. When the judge came striding in and sat down, I was right in front of him. It felt like a first day at a new school and I felt about 8 years old.
Right at the beginning the judge spoke to me and said, quite strongly, to both me and the court, that I was not in any way under any criticism by the court at all and I should not feel guilty about anything. Even now I find that both unexpected and surprising. I have said on many occasions that while I am not guilty of any wrongdoing or lack of truth at any point, I have had to cope with many implications of failure and inadequacy by the NHS during the last three years as they seek to justify their actions.He said he was sorry that I was unrepresented but that he would endeavour to be as helpful as possible. He was helpful and courteous throughout. So were the barristers. I often felt at a loss to fully understand what was going on but that is to be expected as I am not familiar with legal language, and no fault of the professionals.
The options
Initially, HHJ Tindal suggested that there may be three available options with regard to NW’s residence:
(1) NW to remain in the care home;
(2) NW to return home to live with her mother with a package of care; or
(3) NW to remain in the care home, but with regular overnight stays at home with her mother.
Regarding the option of living with her mother, there was a question of whether the care would be commissioned by the CCG, or whether NW’s mother could manage a Personal Health Budget and employ carers directly.
NW’s own wishes and feelings
Whilst ‘P’ may not always have the mental capacity to make certain decisions, s.4(6) Mental Capacity Act (2005) requires that their wishes, feelings, beliefs, and values are taken into account. The Court of Protection has given increasing prominence to this in recent years.
In this case, we learned that not only was NW deemed to lack capacity to make decisions about her residence and care, but that her wishes and feelings were near impossible to determine. Her mother did not argue that NW wanted to return home. Instead she said that NW was unable to have or to express a preference.
Her mother explained that NW has a developmental age of 33 weeks. She believes that NW has Angelman syndrome. NW has recently been tested for this and the result is pending. One of the symptoms associated with the condition is a tendency to smile and laugh, often with little stimulus. NW’s mother said (in a written statement to the court):
“The facial appearance is rather meaningless… The Angelman person has limited or no capability to express any negative emotion at all… [NW] has not cried for many years; she barely reacts if hurt… those reactions are largely meaningless. Some have said that they think she remembers them. But there is no way to tell. She reacts much the same to any person, strangers or not, me included. She has no capability to express a negative choice or any choice at all.”
An exchange between the judge and NW’s mother went like this:
HHJ Tindal described the mother’s opinion on NW’s inability to express choices or views as unusual, and “an incredibly honest philosophical position”.
NW’s mother wrote to Celia Kitzinger, afterwards, about this part of the hearing:
“The judge tried hard to understand when I answered truthfully that since she is unable to express or even show whether she has emotions or can make choices I would be untruthful if I stated that she loves me. I refused to declare that I can easily know what is going on inside her just to suit my own need. I tried to explain that careful observation over a length of time is just a starting point and that she makes almost no meaningful gestures like head nodding, and that I do not pretend that I choose to know what she might want in order to justify my own opinion.“
Expert evidence from a speech and language therapist (provided in a report) concluded that NW “does demonstrate ability to engage in interaction with a communicative partner” via vocalisations, body movements and facial expressions, that she is “aware of people and demonstrates knowledge of who is familiar and who is not” and that her behaviours “are suggestive of her expressing her emotions” but this may only be apparent “when the communication partner is highly familiar with her types of communication”.
The director of care at the Trust which runs Dover House provided evidence that NW engages well with familiar people and “without a doubt recognises who are her peers”.
There was evidence that she ‘plays games’ with staff, declining to make eye contact or ‘talk to them’ and then laughing and engaging animatedly with them. She has indicated she “likes certain individuals caring for her” and NW has spoken single words (including two carers’ names). Care home staff are said to have reported that NW “interacts with all those around her” and that she had taken “a lead role in the home’s pantomime and loved the whole festive experience”.
NW’s mother disagreed with these assessments. She sees them as ‘fantasy’. She dismissed references by the care home that NW ‘engages’ with activities such as drama, as she said that it is not possible for her to interact in this way. She said that “NW is not able to express needs in a way which others can accurately interpret”. In her view, the staff “read things into her, what they assume they should read”. She said that NW is unable to communicate even severe pain or basic choices. She postulated that cats and dogs were better able to express their preferences.
On the other hand, NW’s mother did point to some ways in which NW conveys preferences. She said that she thought NW liked balloons, wondering if she interpreted them as faces. She also said that she seemed to respond particularly well to men’s voices, particularly when they were loud and confident.
The difference of opinion between NW’s mother and the professionals was characterised by the judge, in his published judgment as “a difference of emphasis… not a difference of substance”.
“Like the proverbial half-full or half-empty glass of water, Mum focusses on the limitations of NW’s communicative ability (not least because Mum derives ‘some comfort’ from her belief that NW cannot recognise her own happiness or unhappiness) whereas [the speech and language therapist] focuses on the fragile potential …. This resonates through the evidence in this case: in many ways a debate between Mum’s focus on what NW cannot do and the professionals’ focus on what she can.” (Judgment, 15th May 2021)
What came through most powerfully from her mother’s testimony was her deep and enduring love for NW and her strong commitment to her welfare. She described her daughter as “an unusual and remarkable person”. She said that she thought that NW had “come here for a reason” and that she was “stirring all our thoughts here”.
Dover House vs. returning home – considering the issues
NW’s mother’s position – returning home
The key argument advanced by NW’s mother in court was that her daughter should return home. The main reason she gave for this was because of grave concerns about the care NW was receiving at Dover House and her belief that she would be able to oversee the care provided to NW at home and ensure it was appropriate. She accepted that she could not provide care alone, due to her own health condition, but is content for a care agency to do so, with her oversight.
NW’s mother described the care at Dover House as “horrifying really”. She said that her daughter had sustained a broken elbow under their care (cause unknown). This had been reported to the police and to the safeguarding team (with no evidence of any lack of care found). She also expressed concern about night seizures, NW not wearing glasses and delay investigating Angelman’s Syndrome. She said that on one visit, NW had “big strapping things digging into her neck”, and that on another occasion they “ignored that she was ill – her lips were cracked”. She also said that her daughter was cold all the time. She said, “I just don’t have the right to leave her there”. When asked about how she would feel if the court decided that NW should remain at Dover House, her mother said that in that case “I would pray she doesn’t live very long”.
The judge, however, accepted that “the objective evidence satisfies me beyond any real doubt that NW is very cared for and is settled at [Dover House]”, finding this evidence is “corroborated by the consistent view of a number of experienced professionals” who had visited the home and checked on NW “over a very protracted period of time when Mum was not visiting”.
NW’s mother had – as the judge pointed out – rather limited knowledge of how her daughter was being cared for, since she had only recently started visiting her there. Difficulties with regular contact seemed in part due to practical and financial impediments, and in part due to the mother’s concern that visits might upset or unsettle her. She had however recently visited more frequently, following an order by HHJ Tindal in November 2020, facilitated by funding for travel from the CCG.
NW’s mother described her own living environment as a rather idyllic close rural community. All the neighbours were concerned for NW and were “looking for her”. The house had been adapted extensively for her some years ago. Her mother said that she thought there was a perception that she and NW “did nothing but look at each other” and explained that she had involved NW in many activities up until she went to Dover House over three years ago. She described how she had done horse riding and hydrotherapy for some years, but these had been unfortunately stopped as the staff had become concerned by her seizures.
The written submission (the position statement) prepared for NW’s mother (on a direct access pro bono basis, at short notice) by Victoria Butler Cole made additional arguments. She pointed out that NW’s right to respect for her family is “of fundamental importance”, drawing on case law[1] to argue that: “It is for the state to show that institutional care is better than care at home, and further, that the person’s welfare cannot be adequately sustained other than in an institution.”
This position statement submitted that:
“For someone with limited communication, the significance to NW of being with a person who has known her for her whole life and loves her, cannot be overstated. There is really no comparison between the bond of mother and (adult) child and that with paid carers, whose involvement in N’s life will inevitably be temporary and inconsistent. There can be no doubt that [her mother] knows NW better than anyone else.”
In relation to the ‘third option’ (frequent visits to the care home by NW’s mother), exploration of which was encouraged by the judge at a previous hearing, the formal position statement says:
“The quality and extent of contact between N and her mother if she remains in institutional care is hugely significant. It is not unusual for a parent in [this] situation to feel unable to visit their (adult) child in an institution where the admission and detention of the child are against the parent’s strongly held wishes. Feelings of guilt for not having been able to protect the child, and fear that the child will not understand what has happened and might feel abandoned or rejected, are common. It is also common for people to feel that by visiting they are endorsing the arrangements. It would be wrong in this case for the court to conclude other than that [her mother] loves NW and is dedicated to her, and that their relationship is of great importance.”
The position statements concludes – in line with NW’s mother’s stated position in court – that a bespoke care arrangement using a Personal Health Budget would be the best and most sustainable way of providing care. The court, however, heard evidence from two agencies.
Two community care companies presented evidence regarding potential care packages, should NW return home. Both were confident of their ability to provide such care. The care providers could not be very specific about the options for activities and physical therapy without their services being commissioned, but there was discussion about consistency of community activities being affected by likely timetabling and logistical difficulties. The rural position of her mother’s house and recent incidences of NW having seizures which were seemingly triggered by travelling, were cited as potential obstacles to community activities.
The CCG position – remain at Dover House
At the current care home, NW has access to 24 hour registered nursing for management of her complex needs, including her PEG, postural management for scoliosis, epilepsy management, physiotherapy, occupational therapy and speech and language therapy.
NW’s mother commented afterwards on the way in which one of the witnesses for the Trust described the need for expert nursing care, and the gulf between what was being said and her own experience of managing problems with a feeding tube.
“From my perspective, much of her testimony had little to do with my daughter’s life and care. Perhaps it sounded authentic to the Judge but certainly had no relevance to our community healthcare arrangements. She gave a dramatic description to the judge of potential problems with gastric feeding tube – describing the need for district nurses, emergency ambulances and hospital admissions. It was an enormous exaggeration and made it sound like a real emergency. I realised I needed to act, though I was almost being sick with nerves. I silently put up my fore finger to get the judge’s attention and looked hard at him. He stopped her, then spoke gently to me saying that I should not interrupt. I carefully said “please, I want a chance to respond to this when possible”, and then she continued. He turned to me when she finished and I explained that when we have a problem with a tube, we set up a hygienic area, bring a new boxed sealed tube set from bathroom storage and perform the replacement ourselves. Later, I would inform the speciality nurse with dates etc. and perhaps the consultant’s secretary and that is all.”
Dover House offers a wide range of activities including wheelchair dancing sessions, sensory activities in a special room with a projector, aromatherapy, arts and crafts and (in the neighbouring house) a hydrotherapy pool and special trampoline. NW’s mother referred to this as “Butlins style accommodation rather than committed care at home – care that has exceeded her several life expectancies, with no broken bones and no medical or social care criticisms.”
The available activities and therapies in the community were discussed throughout the hearing. Whether these were assessed to be ‘desired or required’ was said to have a likely impact upon their being funded. However, at Dover House, such activities and therapies were on site and ‘part of the package’. One of the community care providers stated that he was very impressed with Dover House when he visited, and evidence from the CCG was that Dover House provided the “Rolls Royce” option. Evidence from Dover House was that NW had exposure to wider experiences than “in the insular home environment”.
Evidence from care providers and from the CCG was that recruiting and retaining regular, consistent carers was not easy in a rural location and that this would be a particularly difficult task without using a care business. NW’s mother had previously recruited carers using a Personal Care Budget and was confident that she could do this again. She had struggled to recruit carers but said that this was because the CCG had stopped her from advertising.
Official Solicitor – concerns with mother-daughter bond
Before the hearing, the Official Solicitor said in her position statement that the decision about where NW should live was “a difficult, and finely balanced, decision for the court to make”.
In the absence of evidence about NW’s wishes and feelings regarding where she should live, Ms Mellon, on behalf of the Official Solicitor categorised elements of NW’s quality of life, care, and treatment into 9 discrete factors. In this way, an attempt was made to objectively quantify, compare and contrast these factors across the two options. These factors included activities, nursing care and contact between NW and her mother.
One of the main issues on which this case hinged related to the suggestion by NW’s mother that if NW remained in Dover House, their bond would be “destroyed”; a factor described by Ms Mellon as “magnetic”.
The final position of the OS was, although the issue was finely balanced, that it was in NW’s best interests to return home.
“When we left the court for a break the OS barrister quietly spoke to me alone and told me that she was going to suggest that my daughter should be allowed to come home. Very surprising, and it was truly kind of her to let me know.”
The oral judgment
There was a short break before the oral judgment was delivered. During the break, NW’s mother was given a single page summarising the judgment so that she knew in advance what it would be. The decision went against her (and – somewhat unusually – the Official Solicitor). NW must stay in Dover House.
HHJ Tindal began by addressing NW’s mother directly. He said, “There are few occasions in your life when you are going to disagree with someone as much as you are going to disagree with me.”
Although he had drafted a judgment of more than 30 pages, he did not read it out. He said, “You have the right to hear the judgment from me and me talking to you, rather than me just reading it out or hiding behind an email”.
A care package at home would have a number of advantages and a number of disadvantages, but the judge was not comfortable that this would be sustainable in the long term. He was “gravely worried that she would not be able to access activities”. HHJ Tindal told NW’s mother “we will have to agree to disagree. I respect your right to disagree”.
In his written judgement, HHJ Tindal explained that if NW returned home to her mother, he was concerned that the mother’s difficult relationship with the CCG could make the ongoing success of any care arrangements precarious. In the event of the home package breaking down, NW would be unlikely to have a place back at Dover House, and her most likely destination would be a care home less well-suited to her needs.
Considering her fear that the ongoing placement would destroy their relationship, HHJ Tindal said hopefully, “what I see is your relationship re-blossoming”. He continued “given the balance of advantages and disadvantages, I wouldn’t be honest if I said that I felt that her best interests lay with you”.
HHJ Tindal’s judgement was that NW’s best interests lay at Dover House, with transport for her mother to visit her being funded by the CCG. He also requested that funding for her accommodation also be considered. He also talked of ‘mediation’, suggesting that Dover House identify a single point of contact to assist in forging a better relationship between the organisation and NW’s mother.
The ‘resistance’ of NW’s mother to visiting NW at the home reflects, says the judge:
“… her ‘all or nothing’ perspective: either NW returns to live with her or their relationship will be ‘destroyed’. Whilst of course I accept this is not deliberate on Mum’s part, she agreed with me it did feel quite like an ‘ultimatum’”. (Judgment, 15th May 2021)
My reflections
My impression over the three days, was that much care and attention had been taken to explore all the options in some considerable detail. NW’s mother had clearly been deeply hurt and angered by past events around the time that her daughter was taken into care, but the judge was at pains to focus very much on the future, with a “fresh approach” (this included a new representative from the CCG, since the previous hearing in November 2020).
Representing herself as a litigant in person, I felt that NW’s mother’s voice was absolutely heard. She was given time and freedom to express herself. She conducted herself with great dignity and strength. Her commitment to and advocacy for the daughter who cannot speak for herself was truly awe inspiring. HHJ Tindal educated and guided her through the legal process. He was pragmatic in his approach, and I thought he showed humility and flexibility.
During the course of the hearing, it became apparent that the Section 21A challenge had been brought predominantly due to NW’s mother’s serious concerns about the care her daughter is receiving in her current placement. She may have been frustrated that these concerns were given so little attention, but in the apparent absence of other evidence to support these concerns, it was difficult to see how these could have been further addressed within this forum.
I was struck by the approach taken by the Official Solicitor of itemising, comparing, and contrasting factors relating to care and activities between the residence options. On the one hand, how else does one consider the relative merits? On the other, weighing the relative importance of these factors can surely not be so straightforward. Is the unique relationship with a primary caregiver who has lived with and cared for the person for over 30 years, understands them intimately and loves them unconditionally, a tangible benefit that can be quantified? Maybe this would have featured more prominently in court if Victoria Butler Cole had been there to represent NW’s mother.
I have observed a number of hearings in the (virtual) Court of Protection now and they have taught me so much more about the workings of the Court and the application of the Mental Capacity Act (2005) in the legal arena than any reading has done. I learned even more about the real-life application of the law in this area by absorbing myself in a longer hearing, with subsequent access to the associated paperwork. For instance, the final judgement explores the legal arguments and case-law relating to the rights to a private and family life (responding in full to the points raised by Victoria Butler Cole) and the associated implications in this case.
By the end of the three-day hearing, I felt that a rapport had been forged between NW’s mother and HHJ Tindal. He told her that the job that she had done in looking after NW was “nothing short of astonishing”, that he believed her to be an “inspirational person, “heroic” in her care of NW, and “one of the most fascinating people I’ve ever met”.
During his summing up, HHJ Tindal considered whether any review hearings might be required, NW’s mother said,“I’m never coming here again!”. HHJ Tindal explained that he had confidence that she had “the wherewithal and ability” to raise any future concerns and that “she knows where we are”.
I really hope that NW’s mother – despite her profound disagreement with the judgment – will, as the judge suggests, visit her daughter regularly as everyone now seems to want to make possible – enabling her to have what the judge described as “the best of both worlds” – all the facilities of the care home, and the love and attention of her mother. “I would urge Mum to work as hard as ever to do her best for NW. Mum told me more than once NW is here for a reason. I know Mum will always love and support her in that.”
Dr Katharine Shipley is a Clinical Psychologist who has worked for most of her career in forensic mental health and adult neurodevelopmental NHS services. She now works in private practice and has been a Court of Protection Special Visitor since 2017, conducting mental capacity assessments for the Office of the Public Guardian and the Court of Protection. She tweets at @KatharineShipl2
Editorial note (Celia Kitzinger): It is a great privilege, as co-director of the Open Justice Court of Protection Project, to find that families caught up in the Court of Protection sometimes contact us – asking whether we can arrange for someone to observe an upcoming hearing, or simply wanting to make sure their story is heard. This blog is written by a mother who was in touch after I observed (a small part of) a hearing at which she was a litigant in person. In conversation, I asked how the experience of being a litigant in person compared with a previous hearing, seven months earlier (November 2020) when she’d had legal representation. She told me she had already written an account of that experience shortly after the earlier hearing. She’d circulated it among her friends, but not sent it to lawyers or to the judge. When I read it, I was very troubled by how alienated she felt from the whole hearing, and how – despite having legal representation – she had understood very little about what was going on. I asked for permission to publish it (lightly edited to maintain confidentiality in line with the requirements of the transparency order, and with a new opening paragraph) because her account bears witness to some of the challenges the court poses for families of protected parties. The subsequent hearing, in May 2021, was a hybrid hearing at which there were several public observers, including Katharine Shipley who wrote a blog about it, including what this mother told me about her experience of that later hearing.
This is a factual account of my experience of the Court of Protection in November 2020 as it was for me. Being involved in court is very strange – nothing like this has happened before. I gave up work when I had my children but I trained as a nursery nurse and worked in a children’s home for a time.
I have written this anonymously because I have a transparency order saying I cannot write under my name – although I have no secrets and nothing to hide, and my daughter is unaware and cannot be hurt by publicity. I would prefer to use my own name, and my daughter’s name, but I cannot. To learn that a ‘transparency order’ actually means enforced lack of transparency is preposterous.
It was the second hearing about my daughter, Lillian (not her real name) who has profound learning disabilities. She was taken into temporary respite care in 2017 when I had to be admitted to hospital, but has not been allowed to return home – for nearly three years at the time of this hearing. So I applied to the Court of Protection to try to get her back home.
The first hearing was in 2019. On that occasion I sat alone all day with my solicitor in a waiting area. The lady barrister I had then kept coming back and forth across a crowded area to see me. Then we were shown into court for about 10-15 minutes or so in the afternoon and my barrister stood up and gave a few people’s names – after which we all left the court and went home. There was a group of strangers in court who I did not know. I did not understand what was happening then, and I do not understand what was happening at the next hearing, a year later (or why there had to be two hearings).
The November 2020 hearing was supposed to be over three-days, but only the first day happened. I found the whole experience to be very unsettling. I am deliberately not making criticism or expressing opinions about what happened, as I have never been to court before they took Lillian, and so have nothing to compare it with. Was my experience unusual? I don’t know.
I did rather feel that I was an onlooker at someone else’s social event – but maybe that it always how it is.
Meeting my legal aid barrister
I was asked to arrive in the court building for 10.00am to meet the barrister who was representing me. We had once spoken by telephone some months ago and he was a different barrister from the one in 2019. My original solicitor had left the practice and was replaced by another who did not attend the court.
I arrived at 9.30 and was shown to a waiting area. He came straight to me when he arrived, and we went to a side room with a large window and light blinds for some privacy. He shut the door for the same reason. We agreed to take off our masks and sit at distant ends of a long table. The barrister was actually extremely pleasant to me and seemed to be very supportive of me. He asked me some questions he wished to clarify about Lillian.
Other people were coming and going outside the window all day long and soon there was a tap on the door, he stood up to open it, put his mask on, and spoke to them. Some people went into the adjoining room beside us. They were part of our court hearing. We continued to talk about the issues concerning Lillian and more interruptions followed. Every time he had to grab and use his mask, stand up and open the door. Sometimes he went out into the waiting area to talk.
Gradually he was gone for longer periods and was out of sight of the window. One time he came back and said he had met the judge and was very impressed by his attitude to our case. I had the impression there had been a meeting of several of them.
Two ladies came to the door to see me one time when he returned and he told me they were acting for Lillian.
My barrister started to give me advice about issues to do with the court case and the way he felt the judge would be thinking. He was persuading me to accept certain matters in order to make progress. I believe he was spending time in the adjoining room with Lillian’s legal team, and he was telling me that they were willing to be accommodating. At one point he was telling me how greatly impressed he was with the judge and the way the judge was thinking. I am not sure exactly when that was as the barrister was leaping up, down and leaving so often. I just sat there.
At one point he said we were due in court at 1.00pm.
Nearing 1.00pm he said that he was desperate for a sandwich as he had been up since 6.00am and asked if he could get me anything. I said no thank you and he dashed off. I have no idea where he had to go for that. Not seeing the sandwich being eaten I don’t know if he ever got one; but I became aware that he might be in the room next door with the other legal team. It was well after 1.00pm when he came back to talk to me. Then another call at the door and this time he seemed to be called urgently and rushed off.
He was gone for quite a while and when he came back, he was telling me the judge wanted to make plans about me visiting Lillian and arrangements were being made between everybody, and there would be another hearing.
I asked when we would be going into court and he told me that it had happened and was all over. I was shocked.
Afterwards
He then asked if I wanted to talk to the care manager of my daughter’s care home. I don’t know what she was doing there or what she was doing in court. I did not, but I said yes. She very smoothly talked at length about my concerns and how they wanted to deal with my concerns and how they understood my concerns. No mention of Lillian. I stayed silent. I don’t need to be told about my concerns. When she stopped, she asked me ‘did I have any thoughts?’ I just looked at her. As she waited, I said ‘I am here for a court hearing, not for having any thoughts.’ Then I told her that she needed to sort out Lillian’s spectacles and her long delayed blood test. I told her I expect those two demands should be met. Then she left the room.
Towards 4.00pm my barrister asked me if I would like to go home. Surprised I said that surely, I was expected to stay all the time? He told me they were waiting for ‘the court’ to tell what would happen tomorrow and they were preparing documents. I asked what he meant about tomorrow. He said that the court case was all over and I may not have to attend the next day. On that day one of my care assistants was meant to attend the court and had been in contact with the solicitor. I asked what about her and he said that she probably would not be required. I was stunned and said I must text her right away because she had taken a day’s leave to attend and would be preparing. I did so in front of him.
He spent some more time in the other room then came to tell me all was finished; I would not be attending the next day and they were waiting for a document and then some printing. He started to pack his bag, showed me the confusing way out of the building and then ran to get his train.
I had sat on that chair from 10.30am until 4.30pm and had not even stood up in that time!
I don’t understand what was decided at the hearing. I did not get anything like a bit of paper saying “This is what was decided at your court hearing”. I don’t understand why there is another hearing planned for next year. Throughout these months between now and the next hearing my belief is that Lillian is not being given the care that she needs and is not being protected. I just want my daughter to come home.
Concluding Note (Celia Kitzinger)
After reading this account of the earlier hearing, I looked through the court documents to which I’d been given access (as an observer at the May 2021 hearing) to see if I could learn more about what happened. I discovered an account in the Position Statement provided by the CCG for the hearing on 10-12 May 2021. Lillian’s mother had also been provided with this Position Statement as part of the whole court Bundle which she was sent as a litigant in person – but of course this constitutes an overwhelming amount of paperwork in complex legal language. Here’s what it says:
The Official Solicitor’s statement for the May 2021 hearing adds the following concerning the November 2020 hearing:
I have shared this account of what happened that day with Lillian’s mother. She wrote back:
“The barrister did tell me the general idea that the judge presumed that visits to my daughter by me would be automatically of value. But that was when I presumed we had not yet been ‘in court,’ and I would be able to answer and explain to the judge why such theories may not apply to her. Even then the barrister was also bouncing between the rooms and the other lawyers etc. so there was no real conversation. And that still ignores the basic fact that decisions were being made by outsiders without listening to and questioning me as Lillian’s mother.”
It is easy, in my experience for lawyers to over-estimate how much members of the public understand of what is happening in court about matters that intimately concern them and their families. The language and processes are part of lawyers’ everyday work but alien to the rest of us – and can be especially hard to make sense of when we are anxious and under stress.
For a moment I thought I was reading about a maternity case that occurred last century or certainly in some far-away country where women’s rights are not acknowledged. But no, it is England in 2021. It was not so far a departure from the Handmaid’s Tale and that era of womanhood is long gone – or is it?
I am writing this as a midwife of many years and as an experienced psychotherapist who has worked within the NHS maternity services all of my long career. I am also the founder of SANCTUM Midwives, a pregnancy care centre that supports, educates and campaigns in respect of women who have experienced sexual abuse in their lifetime.
Over the course of my professional career, I have seen and implemented the development of sensitive and woman-focused pathways and guidance that has recognised that personalised care is the optimum model for childbearing. Many years ago, I witnessed liberal use of sedatives in childbirth and practices that were crude and by and large unevidenced. I hardly thought that I would see the use of brute force lawfully sanctioned to compel this woman (and, previously, in a very similar case, the woman in a Court of Protection hearing in March 2021) to experience treatment determined for them, and not by them.
Judging whether someone has ‘capacity’ to make decisions is burdened with bias. In my practice and experience, mental capacity is ever-changing and not knowing either of these women I make no judgement about the assessment and finding of lack of capacity. However, the basic principles of the Mental Capacity Act 2005 are clear.
I am somewhat concerned that both these women may have been assessed as lacking capacity to fit the predetermined desired outcome of bringing them into hospital against their will.
Reading the judgment from Mr Justice Holman, I was angry beyond words. It should never have been brought to a court of law. In my experience and that of many Perinatal Mental Health Midwives (who’ve described their experience in another blog here), women who present with a range of anxiety-based disorders are best cared for in a relationship-based model of care, which incidentally these midwives are skilled to offer. In abundance.
This anxiety-based diagnosis is manageable by therapy and sometimes medication to control the anxiety triggers. I know I have worked with many women with these kinds of diagnoses. I could not find in the judgment any recommendation of therapy for this woman apart from prescribing a strong sedative (Lorazepam 2mgs) prior to leaving home in suspected labour. There is no record here either of the benefit of a trusting relationship with her midwife as recognised in the National Maternity Review, Better Births.
Home birth today is an established and safe option for women who are pregnant – it’s even, in some cases, the most appropriate place for birth to occur. I note that two medical professionals gave expert opinion to the judiciary: Professor James Walker (retired obstetrician) and Dr Glover (a psychiatrist instructed by the Official Solicitor, acting for the pregnant woman). Where is the expert opinion from a midwife? I assume in delivery of antenatal care thus far a midwife or midwives have visited the home to establish antenatal care and to assess maternal and fetal wellbeing. Surely the opinion of an experienced midwife in this field could have given some weight to the argument for a home birth or at least some decision about an alternative place to birth such as a midwifery unit within the hospital. In my practice this has usually been a realistic and safe option where women have requested alternative place of birth. Surely this would have given this women a less stressful environment where her labours would have been supported by midwives skilled in this area of care.
This is patriarchal medicine and law at its worst and in complete collusion with each other This woman has been subjected to compulsory (sedated) attendance in hospital in the name of maternity care. A concern with the foetus’s well-being (despite the fact that the foetus has no rights until born within our legal system) seems to have surreptitiously influenced the judge’s decision in this case.
What the judge has done here is to create a precedent that any woman who has an anxiety disorder and requests birth outside of the regular menu of choice may be subjected to strong-arm maternity care – or may fear it, even if in fact the legal process is never instituted. For many women the impact of these experiences during their pregnancy care and birth will cause deep and long-standing trauma. Obstetric violence is a familiar term to me and I am careful in my use of this phrase. However, I cannot think of a better description to illustrate what has happened here in the UK in 2021.
It fills me with deep sadness that these cases have been dealt with in this way, when a gentle and knowledgeable midwife, skilled in relationship-based care, might have achieved a different outcome.
Instead, we have birth by court-order and the annihilation of vulnerable women’s childbearing rights.
My midwife heart weeps.
Dr Kathryn Gutteridge is a Consultant Midwife & Clinical Psychotherapist. This opinion piece reflects her own views in her capacity as a midwife. She tweets @Sanctummid
‘Whatever else it may be a 36-week foetus is not nothing: if viable it is not lifeless and it is certainly human.’ (St George’s NHS Healthcare Trust v S [1998] 3 WLR 936 at 957 per Judge LJ.)
Introduction
In the recent case of A NHS Foundation Trust v An Expectant Mother [2021] EWCOP 33 (hereafter, ‘An Expectant Mother’), the Court of Protection (COP) was asked to give authority for a pregnant woman with severe (‘longstanding and deep seated’) agoraphobia to be transported to hospital for a planned delivery (using restraint if need be), notwithstanding her stated wish for a vaginal birth at home. As is now well-known, Holman J made the requested declaration, having determined that the woman lacked capacity to refuse because her agoraphobia prevented her from weighing relevant information and using it to reach a decision. As is also now known, the woman subsequently travelled to hospital without the need for restraint, and her healthy baby boy was born there, apparently naturally.
There have been numerous responses to the case published on the Open Justice Court of Protection blog (and elsewhere), written from a range of perspectives and focusing on the case’s central themes: mental capacity; best interests; phobias; paternalism and compulsion around childbirth (‘obstetric violence’). In this comment, I take the case as a starting point for reflecting on the COP’s engagement with the late-term foetus.
The status of the foetus in UK medical law
It is well-established in UK law that the foetus – at any stage of gestation – is not a legal person, nor a locus of independent justiciable rights or interests. As Sir George Baker noted in Paton v British Pregnancy Advisory Service Trustees [1979] QB 276, ‘[t]he foetus cannot, in English law, in my view, have a right of its own at least until it is born and has a separate existence from its mother. That permeates the whole of the civil law of this country.’
This position has been reaffirmed in medical law cases involving the right to refuse a c-section. In MB (An Adult: Medical Treatment)[1997] EWCA Civ 3093, Butler-Sloss LJ noted that ‘[t]he foetus up to the moment of birth does not have any separate interests capable of being taken into account when a court has to consider an application for a declaration in respect of a caesarean section operation.’(para. 60, emphasis added)
This was echoed the following year in St George’s NHS Healthcare Trust v S [1998] 3 WLR 936, with Judge LJ observing that ‘while pregnancy increases the personal responsibilities of a woman it does not diminish her entitlement to decide whether or not to undergo medical treatment…Her right is not reduced or diminished merely because her decision to exercise it may appear morally repugnant.’ (para. 957)
Judge LJ was clear that ‘the perceived needs of the foetus did not provide the necessary justification’ for overriding S’s capacitous refusal to consent to a caesarean.
Court of Protection jurisprudence
The principle that the foetus has no separate legal existence applies equally, and has been reaffirmed repeatedly, in the COP (see, for example, Guys and St Thomas’ NHS Foundation Trust v R [2020] EWCOP 4; The Mental Health Trust and Anor v DD [2014] EWCOP 11). In the COP, however, medical treatment cases involve assessing the best interests of the party (P) whose capacity is in question, and where that party is pregnant, ‘the delivery of her healthy unborn baby will be an intrinsic factor’ in the best interests assessment (Guys and St Thomas’ NHS Foundation Trust v R [2020] EWCOP 4 at para. 62, per Hayden J.)
The health and safety of the foetus merits consideration in these COP cases, then, albeit indirectly, and Holman J did consider it in An Expectant Mother:
Using a BAILII database search, I found 14 reports of COP cases involving requests to authorise birth plans (most involved authorising c-section). In all 14, the authorisation was granted. In eight (including An Expectant Mother, which authorised transportation to hospital but acknowledged that P retained capacity to consent to or to refuse c-section), P’s known or presumed wish for the child to be delivered safely was cited as a factor in P’s best interests. In all 14 cases, however, what was authorised was also deemed necessary for P’s own safety, meaning that the wellbeing of the foetus was never the deciding factor.
Logically, for foetal wellbeing to figure at all, it must be possible to know or presume that the foetus is positively valued by P. Hayden J is undoubtedly correct in his carefully-worded observation that ‘it will rarely be the case…that P’s best interests will be promoted by permitting the death of, or brain injury to, an otherwise viable and healthy foetus.’ (Guys and St Thomas’ NHS Foundation Trust v R [2020] EWCOP 4 at 63) Nevertheless, it is possible to imagine a case in which evidence of P’s attitude to the pregnancy would make any consideration of foetal wellbeing under the auspices of P’s best interests, in Alex Ruck-Keene’s phrase, ‘a misleading legal fiction’.
It is interesting to reflect on what would happen if the Court were asked to authorise a birth plan in a case where the risk of not doing so was primarily to the foetus, not to P, and there was evidence of the latter’s indifference or hostility to the former (e.g. an attitude like that of S in the St George’s case, who had said that in her view ‘it would be better for the baby to be dead’). Hayden J has expressed the view that, although a capacitous patient may exercise her autonomy in a way that ‘jeopardise[s] the life and welfare of her foetus’, the COP does not have ‘the same latitude’ to do so when it is the decision-maker. Again, however, this was said in the context of foetal wellbeing fitting within the rubric of P’s best interests. What might happen when the evidence does not support this, or even seems to contradict it?
Among the COP cases I found, there are a few in which P’s attitude to the foetus appears ambivalent, or cannot be gleaned from the text of the judgment (often, in these cases, P is seriously mentally ill or has serious learning disabilities – see, e.g., A London NHS Trust v KB & Anor [2020] EWCOP 59; NHS Trust v JP [2019] EWCOP 23; Re CA (Natural Delivery or Caesarean Section) [2016] EWCOP 51; Royal Free NHS Foundation Trust v AB [2014] EWCOP 50). In these cases, judges tend to make no mention of the significance of foetal wellbeing for P’s best interests. The case that seems to come closest to Ruck-Keene’s ‘legal fiction’ is the case of The Mental Health Trust and Anor v DD [2014] EWCOP 11. In that case Cobb J noted, citing MB, that ‘[it] must be in the best interests of any woman carrying a full-term child whom she wants to be born alive and healthy that such a result should if possible be achieved’ and that accordingly ‘it is plainly in DD’s best interests (both physically and mentally) that her baby is born alive, healthy and safely’ (para. 97) However, I was unable to find any evidence in the case report that DD – who had ‘an extraordinary and complex obstetric history’ (five previous pregnancies with numerous complications, and five children permanently removed from her care) did actively want her child to be born alive and healthy. Unless there is additional evidence not presented in the text of the decision, this seems like a case where the presumption is doing a lot of work.
Conclusion
The right of a capacitous pregnant person to make their own medical decisions unfettered by any consideration for the life or health of the foetus they carry has been enshrined unequivocally in UK law. As Judge LJ emphasised in the Court of Appeal in St George’s NHS Trust v S, pregnancy does not reduce a competent patient’s right to make decisions about their medical treatment, and a capacitous pregnant patient therefore has the right to make a medical decision that might cause death or serious injury to the foetus, however repugnant such a decision might seem to onlookers. It was held in St George’s that S – who professed to be indifferent to the wellbeing and fate of her late term foetus – ought to have been allowed to make such a decision. Arguably, however, it is easy to say this in retrospect, and the real test of the principle would be a judge delivering a prospective judgment that enabled a pregnant person to decide in such a way.
The foetus’s lack of separate interests or rights, even in the very latest stages of pregnancy, has also been repeatedly affirmed in the recent jurisprudence of the COP. However, when a pregnant patient lacks capacity, and a ‘best interests’ assessment is being undertaken, the default position seems to be that P’s best interests will almost always be served by protecting the life and health of the foetus (where this does not risk P’s own life or physical health).
As such, the foetus of a pregnant person who lacks capacity might be said to enjoy a kind of legal status, not as anything of value in its own right, but insofar as it is known, or presumed, to matter to P. As a valued child-to-be, it wins a place in the consideration of P’s own best interests, despite lacking any legal interests of its own.
Nevertheless, as far as the law is concerned, the late term foetus is – despite Lord Judge’s famous dictum – ‘nothing’ meriting consideration in itself, and it remains to be seen what the result would be if a case came before the COP in which there was evidence that, rather than positively valuing the late-term foetus, P was indifferent or even hostile to it. Presumably, the right legal approach in such a situation would be to disregard the health and safety of the late-term foetus, perhaps obliging a judge, in Alex Ruck-Keene’s words, to ‘endorse a plan which could lead to the death of a viable baby’. To navigate such a case would surely prove very challenging, even for a court as expert in making best interests assessments as the COP.
Mary Neal is Reader in Law at the University of Strathclyde. She tweets @maryfordneal
Editorial note (Celia Kitzinger): I contacted Michelle Bromley-Hesketh after she posted several tweets about the judgment by Holman J, as reported in the press and covered by my blog post. She said it made her “very angry”, and she was concerned that pregnant women reading about the case – especially those with mental illnesses – would fear being coerced into hospital.
She also tweeted about her own experience.
So, I asked Michelle – who is now a doula and counsellor/psychotherapist – to describe her own experience of choosing a home birth in the context of agoraphobia. Her youngest son was born at home in April 2013. This is her story. Michelle hopes it will inspire other women with mental illness to know that a home birth is possible – and that it can be (as it was for her) an empowering and healing experience.
—————————————————————————————————————–
My most important message is this: It’s possible to be agoraphobic (or to have a mental illness of another kind) and still have capacity to make your own decisions about how you want to give birth. You can still choose a home birth – and it can be wonderful. I know, because I did this.
I have had agoraphobia since the birth of my first child, in hospital in 2005, when I had severe post-natal depression and developed a fear of hospitals. I can now actually go into hospitals if it’s for treatment for my children, or other people, but when it’s for me I get all the symptoms – panic, heart racing, sweaty, breathing difficulties. In an emergency situation I will be okay, but planned trips for my care can fill me with dread. But even at the height of my agoraphobia, emergency situations wouldn’t faze me.
I wanted to have my second child (in 2007) at home but at that time I believed (without looking at the research) that hospital was safer. She was born really quickly and I had a sense of holding the baby in to get to hospital in time to give birth there, and then her shoulders got stuck and had to be freed. I just thought, “I don’t want to do that again!”. It was a huge amount of anxiety.
My third pregnancy in 2013 was a complete shock. I thought my family was complete with the two children I already had. I was in a new relationship and we definitely were not planning to have any children between us. By this time, I had begun training as a doula and I knew that home birth could be safe. I’d done my research and I knew I wanted to birth at home.
I was told that medically it “wasn’t advisable” – partly because I’d refused a lot of antenatal care during pregnancy and I hadn’t had any blood tests except for one finger-prick iron test. I got some very good therapy during pregnancy that enabled me to have that one blood test.
I also went to 43 weeks (by my dates) – but the scan from the hospital put my dates back 2 whole weeks, which gave me breathing time for NHS induction protocol to kick in. By their dates, I went into labour at 41 weeks. I wasn’t worried. I knew what I was doing.
There was a large element of agoraphobia in my decision to give birth at home, but I am confident that I’d have gone into hospital if there had been an emergency.
I definitely feel I had the mental capacity to make the decision to have a home birth. When I was preparing for this home birth, I read lots of information and weighed up the pros and cons of home versus hospital, taking into account all the relevant factors, but especially considering that home birth would be safe, that I could transfer in an emergency, and that my agoraphobia and fear of hospitals would mean that home birth would be a much better experience for me. I didn’t want the trauma and the panic. A big driver for deciding on a home birth was that I would feel that I was in a safe space, that I would be the person in control: midwives would be guests coming into my space where I hold the power.
My decision to give birth at home was far more informed and considered than my earlier decisions to give birth in hospital were. Back then I didn’t really weigh up any information about home vs. hospital – I just assumed that hospital was safer. It was an uninformed choice: I was going along with what was expected.
I did experience some degree of coercion with my home birth. I was told that I would die or my baby would die – and that’s very scary, especially if you’re already fearful and anxious. Some people treated me like a naughty child. Others treated me as if I had three heads.
The birth
The birth was a healing experience. I trusted myself and my body more than I’ve ever done before or since.
The midwife, Lynn, introduced herself, asked questions about what I wanted to happen and worked with me beautifully. We called my parents to come and keep an eye on the older two children, so we could concentrate on me and the new baby.
I had a birthing pool (it took my partner 2 hours to fill it up) but thought, ” hmm I feel comfy enough doing what I’m doing” and the thought of getting a contraction with one leg in one leg out put me off so I decided to not get in.
Much of my labour I was on my knees on the settee with my face planted into a pillow on the back of the settee, with my partner rubbing my back. My mum just sat quietly watching in the corner, which felt empowering. She seemed calm and just a “mother/ women” energy. Something quite ancient and primal. She has since said that it was an empowering experience for her too.
I began howling and growling, swore a little too, but was inward and imagining thing moving and opening. My dad, who was upstairs throughout, said my sounds were very different to those my mum made and were very animalistic and primal.
My baby descended. I hardly pushed. Waters now popped. (First time this has happened naturally in my births). I had a panicky moment which I think was me actually realising I was having a baby in next minute and requested gas and air for the first time. The midwife went to retrieve it from her car. I had one slight puff, which was definitely a psychological thing and my baby came out! I felt the familiar “flop” feeling and he’d landed on the settee – at 4:13am on 23rd April 2013 weighing 8lb 9oz (he wasn’t weighed until an hour later). I turned over and picked him up and immediately he reached for the breast and we stayed there for ages! The moment felt wonderful and magical and very healing and cleansing even though I had NO idea I needed healing/cleansing. Wonderful!
I will never forget the experience. Amazing, magical, wonderful. I truly felt like a goddess for months afterwards. The high wouldn’t leave and when I think about it, I still smile and feel all tingly!
Reflections
It’s hard to make decisions that other people think are “unwise” – especially then they threaten you with death and serious injury. But I have learnt so much more about childbirth since my hospital births, and it was this knowledge that supported me in making my choices. Knowledge really is power!
Although my baby breastfed immediately after birth, he didn’t feed again for more than 14 hours. I myself had no concerns – he was full of mucus and just needed some time. But the midwives wanted me to go into hospital to get him examined. I said “You want me to go to hospital with my 14-hour old baby? Dream on!” They said I was putting my baby at risk. They said they might need to ring social services and get the duty social worker to come if I refused to go to hospital. Then the GP turned up – but by the time they showed him into the house I had my baby feeding at my breast. If I hadn’t been knowledgeable, at that point I’d have been whisked into hospital for no reason.
On my medical records on the computer, when the GP opens them, there’s a red flag that says “history of Severe Mental Illness” – that’s my depression, anxiety and agoraphobia. That makes health professionals feel concerned and then they try to control what you do.
I still believe I could have coped with an emergency transfer, because I would have accepted the need for it. But to be forced into hospital by punitive people who think they know better than me, without any emergency, before I was even in labour – that would have been awful.
If anyone had insisted that I must give birth in hospital and be admitted before my due date – as happened to the poor woman in the court case recently – I think I would have run away. I would have not told anyone when I went into labour. I would have given birth on my own without any health care professionals in attendance, rather than be forced into hospital – and of course that’s much more dangerous than a planned home birth with midwives. The only way they could have got me into hospital would have been to sedate me and force me. My phobias and panic would have been through the roof and the whole experience would have had a long-term negative impact on me as a woman and mother and would have exaggerated my agoraphobia.
I know that a lot of women will be scared and anxious by the media reports of this case. I want to reach out to them and say that having agoraphobia, or tokophobia, or any other kind of mental illness, doesn’t automatically strip you of the right to make your own choices. They have to prove that you lack capacity to make your own decisions about childbirth – they can’t just assume it because of your diagnosis.
There is support out there if you need it from the childbirth organisations (listed below) who understand the importance of listening to women and empowering them to give birth in the way that is best for them.
Michelle Bromley-Hesketh is founder of Snowdrop Doula Community Interest Company, a mother of three, a doula and counsellor/psychotherapist. Michelle’s interests and expertise are in perinatal mental health, trauma and complex needs, and informed choice. She tweets @michellebee34.
The essential factors in the approach of the court to applications concerning birth decisions are well established. Does the (expectant) mother lack capacity to make a particular decision for herself by reason of a mental impairment or mental disorder? If she does, which of the arrangements on offer is in her best interests and should be consented to by the court on her behalf? If the proposed arrangements include the use of force, is that necessary and proportionate?
In this case, the mother had been diagnosed with agoraphobia, and the consensus view of the psychiatrists involved was that this caused her to be unable to make a decision about whether to have her baby at home or in hospital. She had been unable to leave her home for ‘several years’ other than on a ‘very small handful of occasions’, as this caused her ‘overwhelming sensations of anxiety, shortness of breath, dizziness and palpitations’. She was also said to have short-term memory problems, although the cause of these was not identified.
We can see from the order made in the case, that the particular decisions that the mother was unable to make were ‘decisions about the location of the delivery of her baby’. She was said to be unable to weigh and process relevant considerations as a result of being overwhelmed by her agoraphobia. These considerations are not identified in the judgment – one assumes the analysis was that she was not able to weigh the objective benefits of delivery in hospital as against delivery at home, because she viewed going to hospital as out of the question and could not consider it at all.
The formulation of the decision she lacked capacity to make is important: she was not found to lack capacity to decide on the mode of delivery, only the location. This is perhaps a difficult distinction to draw, since an elective c-section could only take place in hospital, and a home birth could only take place at home. The order envisaged that she would be able to choose, once in hospital, between induction of labour or an “elective” c-section. (This is a little puzzling, since one would think that such a decision ought to be made in advance, the mother’s mental capacity being likely to be most impaired on arrival at hospital having been taken there against her wishes or with the use of force.) The finding that the mother lacked capacity to decide about the location of delivery leached into her apparent capacity to decide about the mode of delivery.
The decision on best interests turned on the evidence of health professionals about the risk to the mother of going into labour at home and then requiring admission to hospital. This was said to occur in about 45% of similar cases, of which about 10% were admissions for urgent medical emergencies. In about 1-2%, these would be ‘urgent blue light ambulance transfers’. Further, the court was informed that home births resulted in 1 in 100 still births or ‘otherwise seriously damaged’ babies, compared to 1 in 200 hospital births. The judgment does not say whether these figures relate to healthy 21-year-old first time mothers like the mother in this case, or whether they concern all births. The difference in risk is said to be ‘largely attributable to delays in effecting a transfer from the home to the hospital’. As ever in medical treatment cases in the Court of Protection, the statistics relied on by the judge are the ones the particular health professionals or independent experts happen to cite – we know from other blogs published by the Open Justice Court of Protection Project in response to this judgment (e.g. here and here) that the statistics in this case may not be universally accepted as accurate.
So, attempting delivery at home was riskier than in hospital, because in the unlikely event that medical intervention was required, it would be quicker and easier to obtain that intervention if the mother was already in hospital. This in and of itself would surely not be enough to overrule a mother’s wish to have a home birth – the higher risks identified are ones which women often choose to take, having balanced them against other considerations. In this case, there were two additional factors – the first was that the mother’s agoraphobia might mean she was resistant to going to hospital even if an urgent need for medical intervention arose, and so the delays or risks of transfer were higher than for other women. The second was that the court found that the mother herself would have wanted to give birth in hospital were it not for her agoraphobia. The reasons for this finding are not given, nor does the judgment contain a full account of the mother’s own stated views.
On the first factor, it is notable that there was no evidence before the court about the extent to which mothers with agoraphobia (or other conditions) are in fact resistant to obtaining medical intervention in the midst of labour if advised that it is necessary to ensure the safety of themselves or their baby. In so many of the cases about mode of delivery that come before the court, the concern of the health professionals is that there will be lack of compliance in labour. Yet in most cases, the babies are born without resort to force or the authority of the court order. Is that because the existence of the order compels compliance? Or are women in labour, whether they have a mental disorder or not, in fact very likely to comply with medical advice when their safety or that of their baby is at risk? Does being in labour itself affect the mental functioning of women with conditions like agoraphobia?
In this case, the independent psychiatrist said that ‘the mother’s ability to co-operate and grudgingly accept hospital transfer would be significantly enhanced’ (if it was advised during labour), but he aded that ‘her co-operation or acquiescence could not however be guaranteed’.
Is a guarantee necessary? There is no real consideration in the judgment of why the court assumed that the mother would remain resistant to going to hospital, if the delivery turned out to be in the (claimed) 10% of cases where urgent transfer was advised. The judge said that the evidence on the mother’s likely behaviour if that occurred was speculative – but this will inevitably be the case in such a situation, and it cannot be an excuse for not considering all the risks and benefits carefully.
One reason, perhaps, for the lack of analysis, is that the Official Solicitor agreed on behalf of the mother that it was in her best interests for the baby to be born in hospital. There was therefore no-one arguing the contrary position – that there was a 90% chance that no hospital admission would be needed; that even if it was, it was likely the mother would comply with transfer; that compelling the woman to attend hospital before going into labour would inevitably result in her having a medical delivery (either induction or, more likely given her agoraphobia, a c-section under general anaesthetic); and that the psychological impact on her of a forced hospital delivery in the absence of any need for medical intervention could be severe, affecting not only her ability to bond with her new-born baby, but also her relationship with the baby in the longer term, and her future decisions about pregnancy. As a result, the judge perhaps felt that he did not need to deal with these arguments in any detail in the judgment, even if they had been raised during the hearing.
The judgment does not set out the risks to the mother and baby of labour being induced, or of the option the mother said was most likely – namely a c-section under general anaesthetic. So there is no weighing up of these considerations against the risks of a possible delayed hospital transfer during labour.
The only issue in dispute before the judge was whether any physical force could be used to take the mother to hospital, in order for her to be induced or have a c-section. The Official Solicitor had agreed that sedating medication could be administered to her, but did not support the use of physical restraint (other than if the mother had gone into labour at home and needed to be transferred to hospital in a medical emergency).
The psychiatrists had agreed that the use of force may have a ‘damaging psychological effect’ on the mother. The court noted that “It may entrench her agoraphobia. It may damage or impair her bonding with her baby. It may give her long-term flashbacks. It may compromise her attitude to future pregnancies, or her dealings with persons in authority.” The judge found that these concerns were outweighed by ‘the known, if small, risk that if a pre-planned birth cannot be achieved, some acute emergency may…arise in the home from which the mother cannot be rescued before some catastrophe occurs to either her or her baby’ and relied on the mother’s stated (and unsurprising) wish that no such catastrophe should occur.
Based on the publicly available information in the court’s judgment, order and care plan, I am not surprised that concerns have been expressed about the decision. There is a lack of detailed evidence about the physical, psychological and emotional risks to the mother of enforcing a hospital delivery on her (in particular a c-section under general anaesthetic). There is apparently no meaningful engagement with what the psychological risks might mean for the mother and for her relationship with the baby. There is no detailed evidence or analysis about why it would not be proportionate to transfer the mother to hospital only if an emergency arose, even though the chances of such a transfer were relatively low and it was said the mother would be significantly more likely to accept the medical intervention offered in such circumstances. Although the use of ‘balance sheets’ has been criticised, they can have the advantage of ensuring that all the relevant considerations are clearly identified, and can then be evaluated and weighed.
For future cases, it would be helpful if there was published evidence about the realities of supporting women with mental health conditions and learning disabilities during labour to give some content to fears about lack of compliance, as well as easily accessible information and expert evidence about the impact of birth trauma. A judge confronted with alarming statistics about the risk of serious harm to a mother or her baby (in this case, a 10% risk of an urgent medical problem arising and a delay in getting to hospital as a result of the mother’s agoraphobia) will need thorough and considered evidence to enable the various options to be properly evaluated.
Victoria Butler-Cole QC of 39 Essex Chambers has appeared in many cases in the Court of Protection, including capacity disputes, challenges to DOLS authorisations, welfare matters, medical treatment disputes and financial cases. She is also instructed in medical treatment cases concerning babies and children. She tweets @TorButlerCole
Over the last two years there have been at least eight cases heard in the Court of Protection concerning place and mode of birth for women who were deemed to lack capacity under the Mental Capacity Act 2005. The case reported last week is the second in a few months about the care of a woman with agoraphobia. Birthrights has been concerned for some time about the extent to which women who are deemed to lack capacity are receiving dignified and rights-respecting care. As noted in the previous agoraphobia case, “a person who lacks capacity has the same human rights as a person who does not lack capacity”. However, in practice it is sometimes hard to see how this is enacted in birth decision-making, when women’s stated choices, wishes and values are often discarded in their ‘best interests’.
As regular followers of the Open Justice Court of Protection project will be aware, this latest case concerns a young woman – referred to throughout as “the mother” – deemed to lack capacity as a result of severe agoraphobia, who had left her home only on a very few occasions in recent years. The judgment states that she wishes to have a home birth, but that this is “due to her agoraphobia and fear of going out”. It indicates that there are no clinical risk factors which might favour hospital birth. However, the issue at hand, we are told, is not the relative benefits and risks of home versus hospital, but the risks associated with transfer to hospital, particularly in the event of a “blue light ambulance emergency”, and whether a planned transfer to hospital is in her best interests.
What is striking in this judgment is the lack of detail behind some of the key statements. It is possible that some of this was laid out in Court, however we don’t know. No-one from the Birthrights team was available at short notice to travel into central London to observe the case; and we know that remote observers were not permitted to attend. This has created significant barriers to understanding what was going on behind the ruling, in the absence of hearing the detail presumably spelt out in Court. There was no apparent reason for this failure to make the hearing open and accessible to observers who happened not to be in commuting distance to London. A video link was available and in use for the woman herself and for other witnesses to participate in the hearing. This technology has successfully enabled many other hearings to be observed, and we know in this case observers stood ready and waiting.
It is particularly frustrating since the Court heard this case before the woman was in labour (so before there was a concern about a contemporaneous obstetric emergency), allowing her to take part in the hearing “at a time when she is not in labour, pain or distress”. The Judge commented that it also permitted “a thorough and informed investigation to take place, as well as a fair and transparent hearing, lasting many hours, in which to test out the issues and evidence”. Our understanding of the case would be significantly improved by having been able to hear reports of this first-hand investigation into the issues and interests in play, particularly the woman’s wishes, preferences and values, and from having more of the deliberation reflected in the final ruling. We have previously joined with calls from others for cases to come to Court in a timely manner, in particular to avoid women going unrepresented. Yet even in this case, with time and with representation (via the Official Solicitor), the woman’s voice is hard to find in the final ruling.
The judgment states that she “would prefer to give birth at home” but attributes this solely to her agoraphobia. This may be an accurate rendition – some of the legal team involved suggested in their commentary that she wanted a hospital birth – but it is not at all clear from the ruling whether or not this really was the only factor that weighed into her wishes. The expert obstetric and psychiatric witnesses speculated that she might more willing to transfer from home to hospital in the event of an obstetric emergency, but there is no sense of whether she herself had been supported – perhaps by a specialist midwifery team – to consider how she might feel or react in such circumstances, or what care would be most helpful to her if this situation arose.
The judgment gives much more space to the views of her partner and mother, who both support transfer to hospital. Combined with the desire to avoid the risk of a “catastrophe” arising during a home birth, and the statement that “the mother dearly wishes to give birth to a healthy baby, undamaged by birth”, Mr. Justice Holman comes to the view that “but for her agoraphobia, the mother herself would opt for a hospital birth”.
As a result, he goes on to authorise both transfer to hospital for a planned birth, and the use of force if necessary, the latter against the submissions of the Official Solicitor representing the woman’s interests.
The judgment does recognise that a forced transfer is “a severe infringement of the mother’s personal autonomy and liberty”, but this is deemed acceptable to avoid the “low” but “grave” risk of a scenario arising at home from which the woman or her baby “cannot be rescued” from grievous harm. For those of us who follow such cases, this reasoning is strikingly familiar. The law is clear that the foetus has no legal interests prior to birth, but inevitably, a healthy baby is deemed to be in the best interests of the woman, despite the harm associated with the actions designed to protect her.
In this case there is at least an attempt to enumerate (some of) the specific harms which may be associated with the use of force in transfer. This does not always happen. However, the brief analysis is presented as “speculative” only, and it is not clear why the Judge ruled that use of force would be proportionate even in a planned transfer, against the submissions of the Official Solicitor.
The Care Plan
In the interests of taking a balanced view, it is worth noting that the level of detail about the final care plan available in and appended to the ruling is beneficial to commentators who were unable to observe the hearing. However, even here there are concerns. The care plan states that it “takes account of the principles of least restriction and patient choice as far as possible, but ultimately decisions have been taken to ensure clinical safety”. But clinical safety is not (necessarily) the same as best interests. And as Prof. Wilkinson noted in his blog, it is not at all clear why the less restrictive option of authorising transfer in the event of medical indication was not given more consideration.
Similarly, the care plan ostensibly reflects the finding that the woman has capacity to choose between induction of labour or Caesarean once at hospital (although apparently not to choose to wait for labour to start). But even this is troublingly circumscribed with the caveat in the ruling that “unless there is a significant medical contraindication, the hospital will respect and be guided by her choice on the day”. Whilst it is the case that a clinician cannot be mandated to give treatment that they believe is clinically contraindicated, this statement does not paint a picture of a genuine free choice, within a sphere where the woman had been declared to have capacity.
This case is only the latest to rule transfer or obstetric treatment to be in a woman’s best interests, despite her stated wishes and feelings. In many cases, the orders deemed necessary by the Court end up being redundant – in the previous agoraphobia case, the woman gave birth at home before transfer could be effected and in this case the woman apparently accepted oral medication to manage her anxiety and was then guided into an ambulance with the support of her family and midwife. What is rarely known, however, but of huge concern, is the long-term impact on women of going through Court processes and having rulings made about the births of their babies that go against their wishes.
Across this area, much more work is needed. We are hugely grateful to the work that the Open Justice Court of Protection Project is doing to highlight the workings of the Court, making them more accessible, and disseminating expert commentary on some of these hugely challenging decisions. There is unlikely to be a one-size-fits-all response to reducing the number of cases coming to Court in the first place and to ensuring that those that do result in best interests decisions which are firmly and unequivocally rooted in a thorough understanding of the person’s wishes and feelings. Support for those who find their capacity in question is vital, as is a grounded understanding of risk and – as the Judge does refer to in this case – the range of decisions that capacitous women regularly make in the face of similar risk profiles. Over the coming months we are looking forward to developing collaborative work with diverse experts across midwifery, medicine and the law to ensure that women always receive rights-respecting care, even in the most challenging of circumstances.
Rebecca Brione is the Research and Partnerships Officer at Birthrights @birthrightsorg. She is also an independent researcher in bioethics in relation to pregnancy and birth and tweets @RebeccaBrione.
By Members of the Perinatal Mental Health (PMH) Midwives UK forum, 25th May 2021
In a recent decision in the Court of Protection (A NHS Foundation Trust v An Expectant Mother [2021] EWCOP 33 (13 May 2021), Mr Justice Holman authorises the use of force if necessary to compel a pregnant woman with agoraphobia to leave her home in advance of her due date to give birth in hospital.
We are deeply concerned about the implications of the decision on the maternity care of women with complex mental health needs.
We write as perinatal mental health midwives and members of the Perinatal Mental Health (PMH) Midwives UK forum.
Specialist perinatal mental health midwives (as well as consultant midwives who have a remit for perinatal mental health) are frequently involved in complex birth planning for women with significant mental health disorders. (For more information about this role see the Royal College of Midwives document here).
We have experience of creating individualised birth plans for women with severe anxiety, obsessive-compulsive disorder, post-traumatic stress disorder and psychotic illness, as well as agoraphobia. We have experience of cases where the multi-disciplinary team had positively planned for a home birth as the safest and most preferred option, with care provided by an experienced group of midwives skilled at home birth, and ongoing senior support and planning for labour events as well as planning for possible deterioration in mental health. Our experience is that in all these cases, there were safe and happy outcomes – without recourse to court orders or forced hospital transfer.
We are gravely concerned that this judgment permits the use of chemical and physical restraint to enforce a hospital admission, without any actual risk to the life of mother or baby.
This sends a very worrying message to women who want to choose to stay at home to birth their babies.
Forced hospital admission risks psychological impact of further trauma postnatally, damage to the mother’s ability to bond with her baby and to parent, as well (as acknowledged by the court medical experts) known trauma and long-term adverse effects from the use of restraints. These concerns have not, in our view, been adequately or fairly considered in making this judgment.
We believe this judgment to be a form of ‘obstetric violence’ – the over-medicalisation of childbirth without informed consent. This term was first officially introduced in 2007 in Venezuela as a new legal term rooted in a human rights perspective (see Perez, 2010, and the powerful film by Amnesty International here). It’s defined as:
“the appropriation of the body and reproductive processes of women by health personnel, which is expressed as dehumanized treatment, an abuse of medication, and to convert the natural processes into pathological ones, bringing with it loss of autonomy and the ability to decide freely about their bodies and sexuality, negatively impacting the quality of life of women”.
The largest recent and most comprehensive meta-analysis comparing outcomes of intended home and hospital birth(Hutton et al, 2019) finds that risk of stillbirth, neonatal mortality or morbidity is not different whether birth is intended at home or hospital. A further systematic review and meta-analysis (Reitsma et al, 2020) found women intending to give birth at home were less likely than women intending to birth in hospital to experience: caesarean section, operative vaginal birth, epidural analgesia, episiotomy, 3rd or 4th degree tear, oxytocin augmentation and maternal infection.
A hospital birth, in particular a non-medically indicated induction or caesarean, has greater risks to the mother and no improvement in outcomes for her baby. Yet women with severe tokophobia (overwhelming fear of childbirth) are supported in their choice of mode of birth and offered caesarean sections despite evidence that a non-medically indicated caesarean has some increased physical risks for the mother and no perceived benefit for the baby. It is not considered good practice to sedate women with tokophobia and force them to have a vaginal birth.
But Mr Justice Holman is forcing unnecessary intervention on the agoraphobic woman in this case and increasing her risks of having unnecessary surgery when she is expressing an entirely reasonable wish to remain at home. At home, the likelihood is that she will have a healthy baby via vaginal birth without intervention. Instead, it seems highly likely that she will end up with a caesarean section via general anaesthetic as a “choice” she will make arising directly from forced hospital admission (para. 23).
Transfer from home to hospital is often resisted initially and can rarely be ‘guaranteed’
According to Mr Justice Holman: “The nub of this case is the potential difficulty of transferring this particular mother to hospital if a medical emergency arose, but she was so overcome by her agoraphobia that she would not go.” (para. 11).
In our experience, transfer from home to hospital is not always something women readily agree to at the outset. However, when faced with an emergency situation most women are strongly motivated to act in the best interests of themselves and the unborn child. The chance of achieving this outcome is even stronger when a woman’s concerns have been heard and validated by the team caring for her.
In this case, in the unlikely situation where birth started at home and urgent transfer to hospital was recommended, both expert witnesses (one a psychiatrist, the other an obstetrician) considered that this mother would indeed accept (albeit “grudgingly”, para. 19) a transfer to hospital – although this could not be “guaranteed” (para. 19). As we understand it she has not (in advance of the event) declined transfer in an emergency. In our view, using litigation to control this situation before it has unfolded is unhelpful.
Women with the capacity to make their own decisions about place and mode of birth are legally entitled to make ‘unwise’ decisions. This includes those with complex physical conditions, for whom birth in hospital is recommended as the safest place. Nonetheless, they have the human right to give birth in a place of their choice, and are frequently supported to do so. In this context, we consider it entirely disproportionate to deny to the woman in this case the freedom of choice to birth at home that is afforded to capacious expectant mothers, and to give so little weight to her wishes in this matter.
This judgment undermines trust between women and caregivers
This judgment has been widely publicised in the media (as analysed in this blog) and has resulted in heightened public awareness of the possibility that a pregnant woman can be forced to comply with an order from a court. This can only undermine our ability to build good relationships between women and caregivers, thereby making it harder for us to work together to achieve safe outcomes.
It is this trust which, as specialist perinatal mental health midwives, we seek to build in the most challenging of circumstances to support open conversations about risks and rights.
The most important theme through all of our experiences in caring for women with severe mental illness (and, possibly, lack of mental capacity for birth-related decision-making) is that we listen to women. We ensure each woman feels safe and heard. We ensure that we give her all the evidence in a non-biased way, develop a trusting relationship, and are able to act as her advocate.
This trust, which supports women making safe decisions about birth and preserves women’s psychological safety, is totally undermined by this judgment.
The Court of Protection needs midwifery expertise in perinatal mental health (PMH)
From the judgment it appears that the court heard expert evidence from two people. One was
Dr Tyrone Glover, a consultant psychiatrist, who gave evidence about the debilitating effect of the woman’s agoraphobia on her decision-making capacity about leaving her home. The other was Professor James Walker, a consultant obstetrician with numerous recent publications on pre-eclampsia (which is not at issue in this case).
We are very concerned that the Court of Protection did not seek evidence from a Consultant Midwife with a remit in PMH and/or a specialist PMH midwife. Midwives are the experts in physiological birth and in particular home birth, and as such an expert view from this profession should have been sought rather than an obstetric view only.
As PMH midwives we have a huge amount of experience in the practicalities of birth at home, in midwifery led care as well as supporting ‘out of guidance’ birth plans in complex cases.
It is a great pity for this woman, and for all women reading about this case who are now concerned about being forced into hospital themselves, that the appropriate expertise was not made available to the court – and, indeed, to the woman herself before the case ever came before the court, thereby avoiding the need for legal intervention.
We recommend that when cases like this arise in future and appear to be heading towards the court, contact should be made with the woman’s local or neighbouring Trust for a consultant midwife with PMH remit or specialist perinatal mental health midwife. This might avert the need for a court hearing altogether. Alternatively, we would be available to provide evidence for the court and can be contacted via our team email address: perinatalmentalhealthmidwives@gmail.com
Authorship: This piece was written collectively by members of the Perinatal Mental Health (PMH) Midwives UK Forum. It reflects the opinions of the individual authors not their affiliated Trusts. Unless otherwise indicated each of the authors is a perinatal mental health midwife: Kate Allon, Laura Bridle (also trainee consultant midwife), Susie Cabrillana, Kelda Folliard, Suzy Hall, Mary McCarthy, Louise Nunn (Consultant midwife, PMH lead for maternity and Co-Chair NW London Mental Health clinical network, Chelsea & Westminster Hospital NHS Trust), Bernice Peter, and Laura Walton. Contact: perinatalmentalhealthmidwives@gmail.com

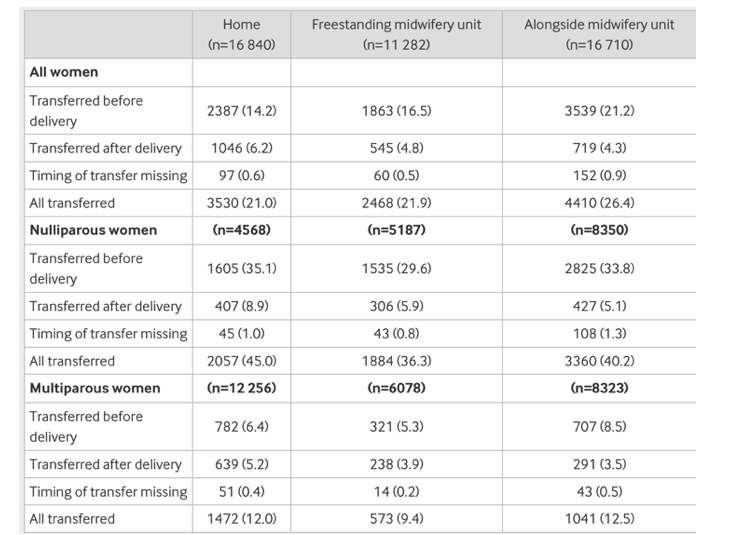






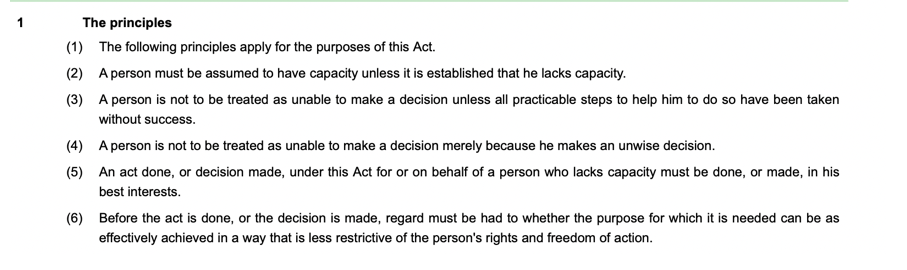







.jpg#filelinks){kind=link}