By Celia Kitzinger, 29th July 2025
The aim of this blog is to promote a more realistic understanding, both for would-be observers and for court staff, lawyers and judges, of what it takes to observe (remote) court hearings. I want to make visible how much time and energy it takes – not only for me but also for others (especially, court staff) to achieve the relatively modest ambition of access to Court of Protection hearings. Transparency is a very time-intensive and costly commitment.
It was Monday 21st July 2025. I’d returned from a 10-day hiking holiday at the weekend and was eager to get going again on court observations. I live in rural Cumbria and most of the hearings I watch are remote (i.e. via MS Teams or Cloud Video Platform). I set out to observe a couple of hearings and after looking at the listings (almost all were remote hearings), I chose one case for the morning (10am in Exeter before District Judge Murray – a judge I’ve never seen before) and another for the afternoon (2pm in the Royal Courts of Justice [RCJ], before Mr Justice Poole, a judge who is very familiar to me). By 8.30am, I’d sent off requests for both links.
This blog is about what happened next.
It turned out that both of the hearings I wanted to observe were vacated (i.e. they didn’t happen) although I didn’t learn that until nearly an hour after the listed start time for the Exeter case and about an hour and a half before the start of the RCJ case. Lots of hearings are vacated (about a third of all those I apply to observe) and – contrary to the suggestion sometimes made by would-be observers – I don’t think for one minute that hearings are vacated to prevent us from observing them! Reasons why hearings can’t go ahead as planned are explained in another blog post (“Last-minute vacated hearings in the Court of Protection”). Often it’s because the parties have reached an agreement about the order and the judge decides the case on the papers. I don’t know why the afternoon hearing I’d asked to observe today was vacated, but the morning one (to which I was briefly admitted) was abandoned because the judge had been asked to recuse himself (i.e. to remove himself as judge and allow a different judge to hear the case).
Like other observers who set aside time to watch court hearings (many of whom have to navigate time out of their working days or caring responsibilities), I tried over the course of the day to replace the vacated hearings with alternatives. I wasn’t too bothered about which hearings I observed – I was simply looking for time-slots that worked.
In the end, I was successful in observing two hearings – albeit not the two I had initially requested – but it involved a full day’s work of repeatedly checking the listings for candidate hearings, emailing the court staff for links, chasing the staff when the links didn’t materialise by the time of the listed start of the hearings, pursuing Position Statements from lawyers, and (in one case) requesting a variation to the reporting restrictions due to an error in the Transparency Order.
I’ll describe what happened, moment by moment throughout the day, and then reflect on how unwieldy, time-consuming, stressful and expensive this process is, and the high cost of open justice both to me and to the justice system.
My observation experience
08:15 I request the Exeter hearing: COP 20014381 at 10am before DJ Murray
I selected this one primarily because I wanted a 10am hearing – the earliest available – to leave open the possibility of applying for a later (11am or 12 noon) hearing that morning if it was vacated.
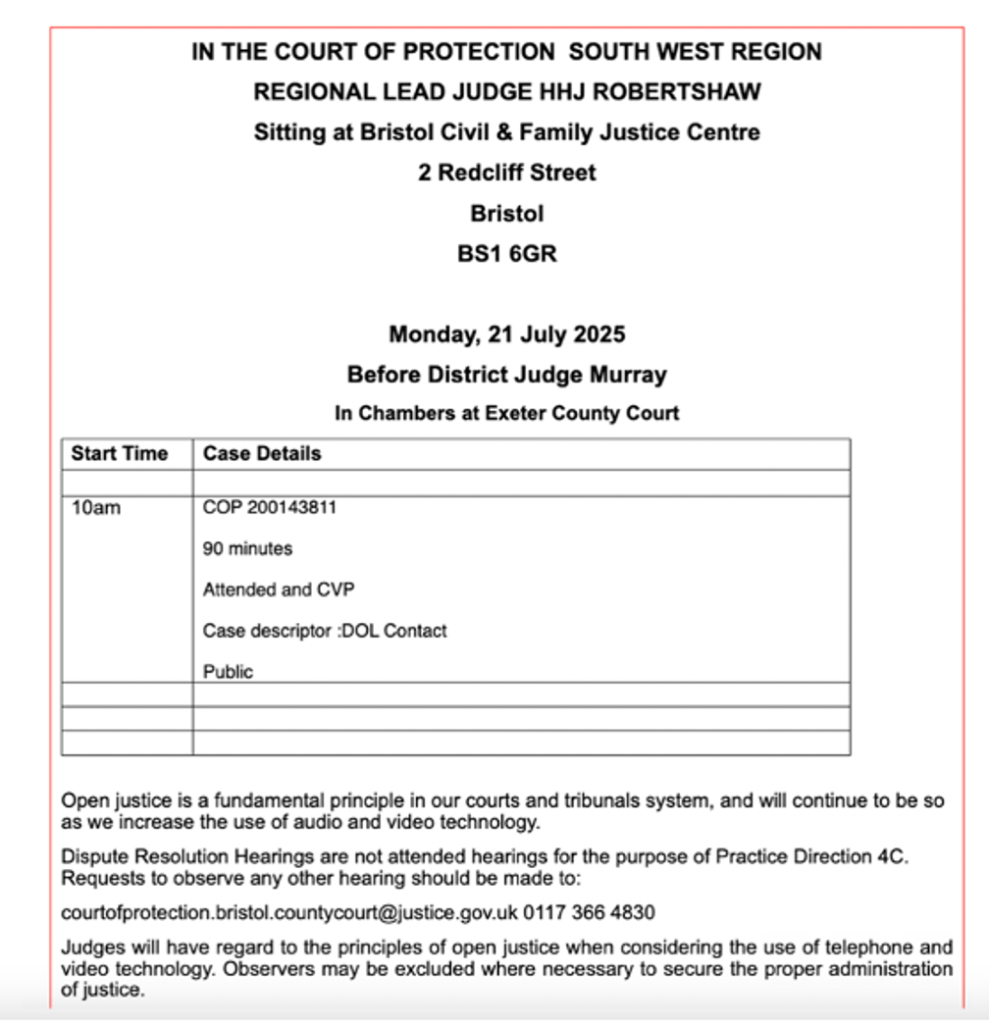
I also chose to observe this one in particular (there were quite a few 10am hearings) because I’d spotted some problems with the listing (reproduced from CourtServe below):
- there’s an additional digit in the listing: COP hearings typically have 8 digits, so nine digits is odd and probably an error (I turned out to be right about that). It might be a small point but errors in case numbers make it hard to use electronic searching when we’re looking for them later.
- it’s confusing to find a statement that the judge is hearing the case “in chambers” (which means “in private”) but also that the case is “public” (it turned out to be – as most COP hearings are – in public). This could easily lead a member of the public not to request a link.
- the public bodies are not identified in the listing – which I discovered was definitely an error as the Transparency Order (sent to me as a consequence of my request to observe) does not prohibit identification of the public body as Devon County Council. This has important transparency implications, of course.
In accordance with the instructions in the listing, I emailed Bristol (the regional hub) with my request for the link and Position Statements. What usually happens is that the hub passes on requests to the court at which the case is actually being held, so I expected them to forward my email requesting the link to Exeter court staff, who would then alert the judge. The procedure for dealing with requests for Position Statements is not (as far as I know) yet formalised[1], but I hoped Exeter court staff would forward my request for the Position Statements to the lawyers involved in the case (which, it turned out, they did).
Here’s the email I wrote to the regional hub at Bristol.
Please may I have the link to observe this hearing (as per the Courtel/Courtserve listing reproduced below).
Please could you also alert the parties to my request for all the Position Statements (and for the Transparency Order) relating to this hearing. This is so that I can follow the hearing and to support accurate understanding and reporting of it.
The court may be aware that there is new case law relating to provision of Position Statements to observers. For guidance from Poole J see §36(1)-(10) in AB, Re (Disclosure of Position Statements) [2025] EWCOP 25 (T3) (15 July 2025)
In brief:
- counsel can share anonymised PSs with observers without seeking permission from the judge. (§36(5))
- Alternatively, counsel should ask the judge at the beginning of the hearing for permission for release of non-anonymised PSs. (§36(6))
- If any party refuses to provide their PS to an observer, they should so inform the observer who can then make an oral application to the court (§36(7)(8)(9).
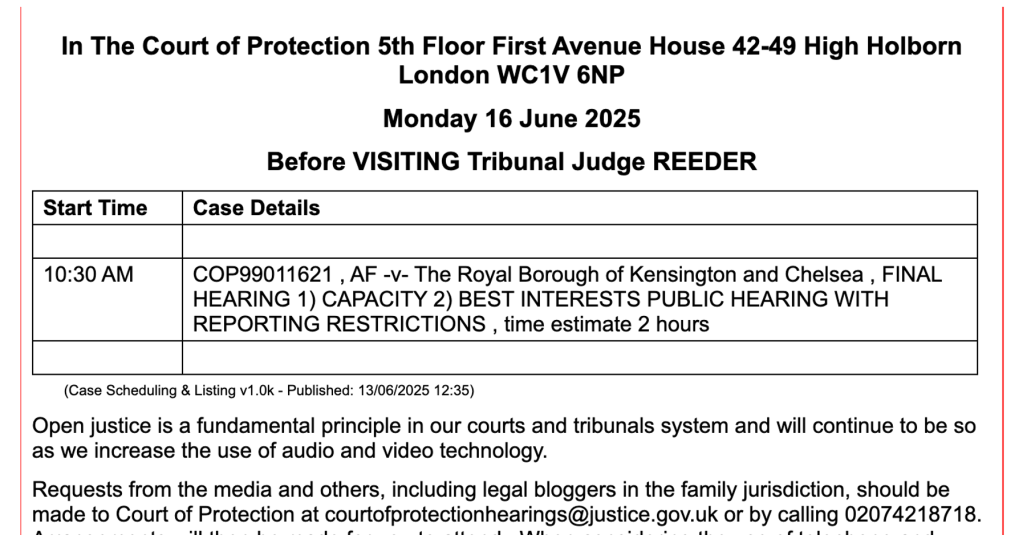
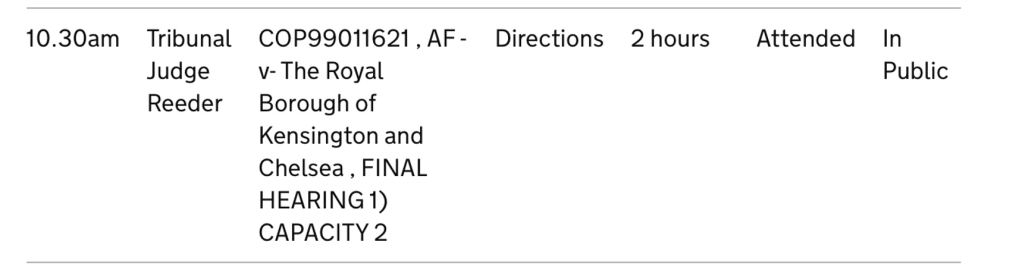
08.30 I request the Royal Courts of Justice hearing: COP 20001522 before Poole J
I’ve watched Mr Justice Poole many times before. He’s very interesting to observe and I’m looking forward to doing so again. I know nothing about the case save what is in the listing – reproduced below – and it’s new for the RCJ listings to provide information about the issues before the court, so I’m pleased to see that, and I say so in my email to the staff when I request access. As with my email for the Exeter hearing, I request both the link and the Position Statements. In neither case do I know who the lawyers in the hearing are, so I have no way of contacting them directly to ask for Position Statements.

09.42 I chase the Exeter hearing (listed for 10am): “Hello – I’m resending because the hearing is listed to start in less than 20 mins and I’ve had no acknowledgment, no link, and no PSs.”
10:00 I request Stoke on Trent hearings (listed for 11am and 12 noon before HHJ Davies)
I suspect I’m not going to get access to the Exeter hearing, so I try elsewhere. I have no particular interest in or knowledge about the Stoke on Trent hearings – but they are listed for (what are now) convenient time-slots. Surely one of those will turn out to be possible?
10:06 I receive the link and Transparency Order for the hearing I want to observe this afternoon – the Royal Courts of Justice hearing (COP 20001522 at 2pm before Poole J). Oh good, at least that one’s sorted!
10:09 I receive information that the Exeter hearing (listed for 10am) is delayed. “Good morning, The hearing is delayed. We will keep you updated”. Ah, so that sounds as though it will be going ahead, but meanwhile I’ve asked for the Stoke on Trent hearings (at 11am and 12 noon), so I hope it starts soon, otherwise I’ll have been granted access to two hearings taking place at the same time and will have to pull out of one of them. (I juggle applications to observe hearings carefully so that this doesn’t often happen – I think only a handful of times ever, over the course of five years and 600+ observations. When it has occurred, I’ve apologised profusely to the court that I’ve taken up their time in arranging my access to a hearing I now can’t attend.)
10:44 I receive the link for the Exeter hearing (listed for 10am) – which I don’t see right away because I’d given up on getting it and was chasing Stoke on Trent (see below) and searching the lists and writing requests to observe other hearings instead. (I see it six minutes after it was sent [at 10.50am] and join then, but am not admitted until 10:54am).
10:46 I chase Stoke-on-Trent hearings (listed for 11am and 12 noon) I’m still assuming at this point that I won’t be able to watch the Exeter hearing, and I’ve also heard nothing back yet concerning either of the two Stoke on Trent hearings: “Hello – I’ve requested access to two MS teams hearings (see below), the first of which is listed to begin in 15 mins. I look forward to receiving the links.”
10:50 I am told the Stoke on Trent hearings are vacated. “Unfortunately, both of those hearings have now been vacated.” I’m not having much luck, am I?! I check my emails again and find I’ve finally been sent the link to the Exeter hearing. I join it.
10:54 I’m admitted to the Exeter court: I learn the case is being adjourned until a different judge can hear it.
It was to have been hybrid hearing. Two people are in the physical court room and there is at least one lawyer on the link. It’s apparent that something has been going on without me (maybe since 10.00am which was the listed start time?). The judge tells me he’s sorry that there were “logistical difficulties” at the beginning of the hearing and that “something was brought to my attention earlier this morning which means I as a judge can’t deal with this case”. He says he was “hoping to proceed today with a different judge” but that’s turned out not to be possible. He’s courteous and apologetic – but I’m not sure why I wasn’t admitted earlier to observe what (I think) would have been a request to the judge to recuse himself. The judge deals briefly with a request from one of the lawyers to alter the initials used for parties in court documents (agreed), but a week later I’ve not received a revised Transparency Order (the one I have was made by DJ Priddis on 10th April 2025 and issued on 12 May 2025). I can deduce the initials originally used for P from the Transparency Order I already have, and the new initials (for P and for other lay parties) from those used on the Position Statement which I received later from the Official Solicitor. At this point I have no idea what the now-adjourned hearing was about. It only becomes clear when I read the Position Statement from the Official Solicitor sent after we all leave the video-platform.
On reading the Position Statement, I learn that the case concerns what, in the view of the local authority, is mistreatment and financial abuse of a woman in her 90s. It appears that P granted Lasting Powers of Attorney (both Property and Finance and Health and Welfare) to one of the two people (I think the two I saw in the physical courtroom) who have gone on to (allegedly) abuse her. The Lasting Powers of Attorney have now been disclaimed and there’s an application to appoint a panel deputy. The issues currently before the court don’t seem to be reflected in the case descriptor in the list (which says the case is about “DOL Contact”), but it’s common for cases to move on and for the court’s focus to shift, without listings being updated to reflect this. That’s an ongoing problem for court observers keen to learn more about particular issues of interest to them. There’s been a lot of publicity recently about abuse of Lasting Powers of Attorney[2] and this is an important matter of legitimate public interest that hasn’t been flagged up properly in the public listings.
11.09 I request the link for a hearing in Hastings (12 noon before DJ Owen)
As I’ve not yet succeeded in observing a hearing this morning, I go back to the listings to see what else I can find. There are two hearings listed before DJ Owen in Hastings – another judge I’ve never watched before. They’re both listed for 12 noon, which suggests to me that the judge believes that one or other might be vacated (or that he’ll reallocate one them to a later time if both go ahead). I know nothing about these cases – but I’m looking for a 12-noon hearing to fill the gap. I say “Please may I have the link to observe either of the two hearings listed for 12 noon before DJ Owen (as reproduced below from CourtServe). If they’ve both been vacated, and DJ Owen is hearing a different case at 12 noon then please may I have the link to that one.” I also apologise that “this request is being sent closer to the time of the listed start of the hearing than I would have liked” and explain that this is because other hearings have been vacated. I do this knowing that judges occasionally chastise us in open court for having asked “very late” to observe hearings, and I hope to pre-empt and avert that public humiliation. Sometimes, it seems, judges simply don’t understand that we can’t ask for links until the listings are published at around 4pm the day before (see “Why members of the public don’t ask earlier to observe hearings (and what to do about it)”) and I figure the judiciary is unlikely to have any awareness of – or be able to imagine – the situation I find myself in now (which is one of the reasons I’m writing this blog post).
11.19 I receive the Transparency Order for one of the 12noon Hastings hearings. As usual, there’s been an automated reply (at 11.10am) saying my email will be dealt with within 10 days but then I get this: “Your details have been forwarded to the relevant team for the link to be sent to you. Attached is the Transparency Order (for 20004304) which you must read through before the hearing. The other case (20002225) has been adjourned“.
11.31 I receive a follow-up response concerning my request for the Hastings Position Statements – my request for the Position Statements has been forwarded to the judge
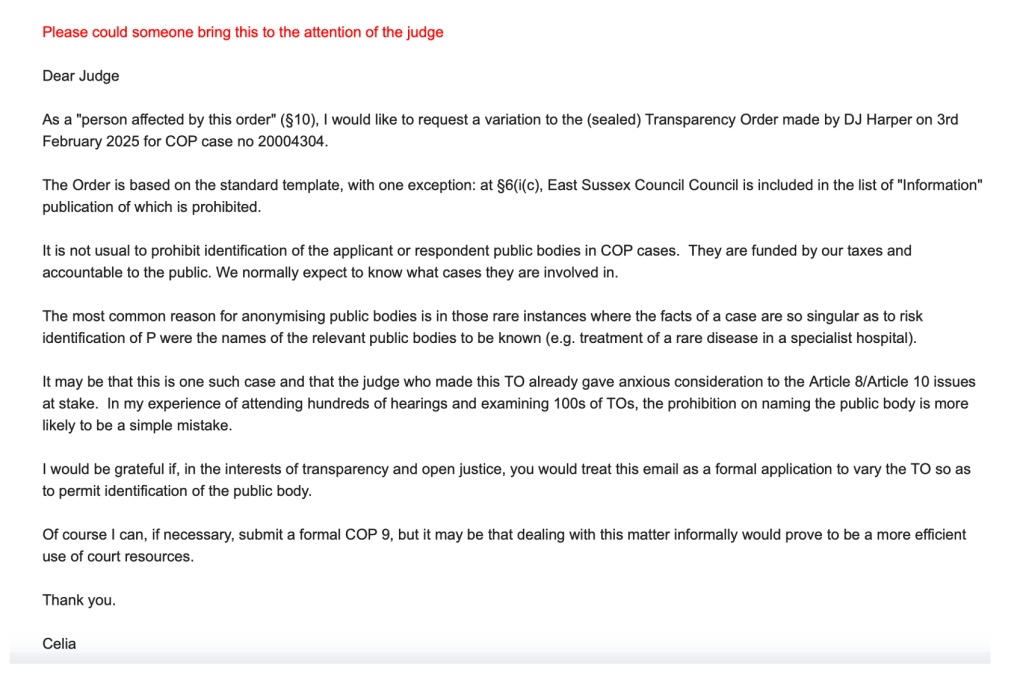
11:36 I send an email for attention of the judge (DJ Owen) in the Hastings case, requesting a variation to the Transparency Order. I’ve discovered a problem with the Transparency Order for the DJ Owen (Hastings) hearing. It says (§6(i)(c)) that I’m not allowed to name the public body as a party to the proceedings. I email the judge making an informal application to vary it.
11:58 I chase the link for Hastings “Sorry to bother you again but I’ve not received the link for the hearing listed to begin in about two minutes.”
12:18 I chase the link for Hastings again “I’ve checked my spam. I keep refreshing my email… Please can someone send me the link”
12.24 I’m told the Royal Courts of Justice hearing for this afternoon is vacated. “The COP matter listed before Mr Justice Poole this afternoon has been vacated”. Oh no!! Now I’ll have to find an alternative hearing for the afternoon! It’s early afternoon – I’ve been trying since 8am and I’ve still not observed a hearing.
12:31 Reading Hub tries to help with the Hastings link. Staff copy me into an email sent to Hastings (“Following my earlier emails please see below a further email from Celia Kitzinger who is chasing the link for the hearing which started at 12 pm.”)
12.40 I still have no link for the 12noon in Hastings. I assume it’s been vacated (or gone ahead without me), so I ask for the 2pm before the same judge also sitting in Hastings (DJ Owen, COP 14115755). I say: “I was very disappointed not to be sent the link for the 12 noon hearing before DJ Owen. Can someone please explain what went wrong. This is not a good look for transparency in the Court of Protection. Can we try again please. There’s a 2pm hearing (screenshot from CourtServe below) also before DJ Owen in Hastings. Please could I have the link to observe that. Perhaps this time it will be possible to sort out how to get me the link. I am making the same request for Position Statements (and the Transparency Order) in relation to this hearing” (and I spell out what that request was again).
12.40 Link to the 12noon Hastings hearing arrives. My email chasing the link turns out to have been sent at exactly the same moment as the “Digital Support Officer” sent the link itself. As soon as I refresh my email, I see it!
12: 42 I join the hearing in Hastings: Appointing P’s son as Deputy for Property and Affairs
There’s no proper introduction (perhaps because I’m slightly late joining) and I’m not sure who is in court but I recognise one lawyer (and locate him via google) and it becomes clear that someone else (whose camera isn’t on) is the son of the protected party. The judge confirms that the lawyer will send me a “Case Summary” on behalf of East Sussex County Council (I’m not sure whether this means there are no Position Statements?) and I email the lawyer to make sure he has my contact details at the same time (it turns out) that he emails me to make sure he has mine.
The judge says at the outset that there’s “no good reason not to identify the council involved” and that he’s “happy to endorse that amendment of the Transparency Order”. (Hurrah! That at least was efficient.).
The lawyer tells the judge that P’s son is now willing to act as Deputy for his father. The judge asks the son about this and he says (as best I could capture it) something like this: “My father’s always been a very strong man and very clear that he wants to be in control of his own affairs. As his health has deteriorated, he’s become increasingly unable to do that. Initially, we agreed that I wouldn’t act on his behalf, hence why I didn’t apply to be Deputy earlier. It wasn’t that he didn’t want me to be Deputy, it’s that he didn’t want anybody to be his Deputy. But as his health has deteriorated, he’s come round to agreeing that a family member should do it. The days when we had a large amount of money to manage are long gone, but it’s all the things I have to remind him about on a daily basis – outstanding debts, his car that’s been in a carpark for three years that’s accruing fines, and he loses his bank card probably on a monthly basis and that’s always a rigmarole. It’s all the simple but frustrating matters of day-to-day practicalities. And I’m the best person to do that. I visit him monthly and speak to him on a daily basis.”
Counsel for East Sussex County Council says that the son’s position is clear, and that “there’s a benefit for a family member to do it” so the local authority is “happy with that”. The judge checks there’s “no doubt as to the absence of capacity – there’s no one seeking to challenge that or raise any doubts?” Counsel says: “His son has been very polite about it, but P burnt through the money from his properties and there are questions as to whether others may have benefitted and taken advantage of him. It’s a bit sad. But the reason why there’s a hearing is because P himself was asked about this and he didn’t agree with the application. He said he does not lack capacity and he has “no issues managing my finances”. We can be as respectful as we can of his views, but every factual matter points in the other direction”. (When I read the “Case Summary”, sent later the same day in lieu of a “Position Statement”, I learn that P has Korsakoff syndrome.)
Around this time the judge notices that the son has left the video-platform and waits for him to return (without any support, since “the ushers are stretched between more than one hearing”). When the son returns a few minutes later, the judge confirms that he will approve the draft order and the son’s appointment as P’s Deputy. The hearing ends at 13:00
During the hearing some emails are exchanged….
- 12:46/12:47 Counsel sends me an email to check we are in contact (I respond immediately “yes!”) at the same time as I send counsel an email for the same reason saying (only) “yes, please for the PS”. We now know each other’s email addresses.
- 12:51 Court staff say: “We have just received an email from DJ Owens saying his previous case has just finished. He has also emailed counsel about amending the Transparency Order and in relation to your request for the position statement. Please note the 2 pm hearing has been adjourned.” (The 2pm hearing is the one I’d asked to observe when I thought the one I’m watching now must have been vacated or proceeded without me.)
- 12:57 I reply: “Yes, thank you – I am now in the 12 noon hearing. Understood that the 2pm is not available to observe. Many thanks for your help.”
13:00 End of hearing before DJ Owen (Hastings). It’s lasted less than 20 minutes.
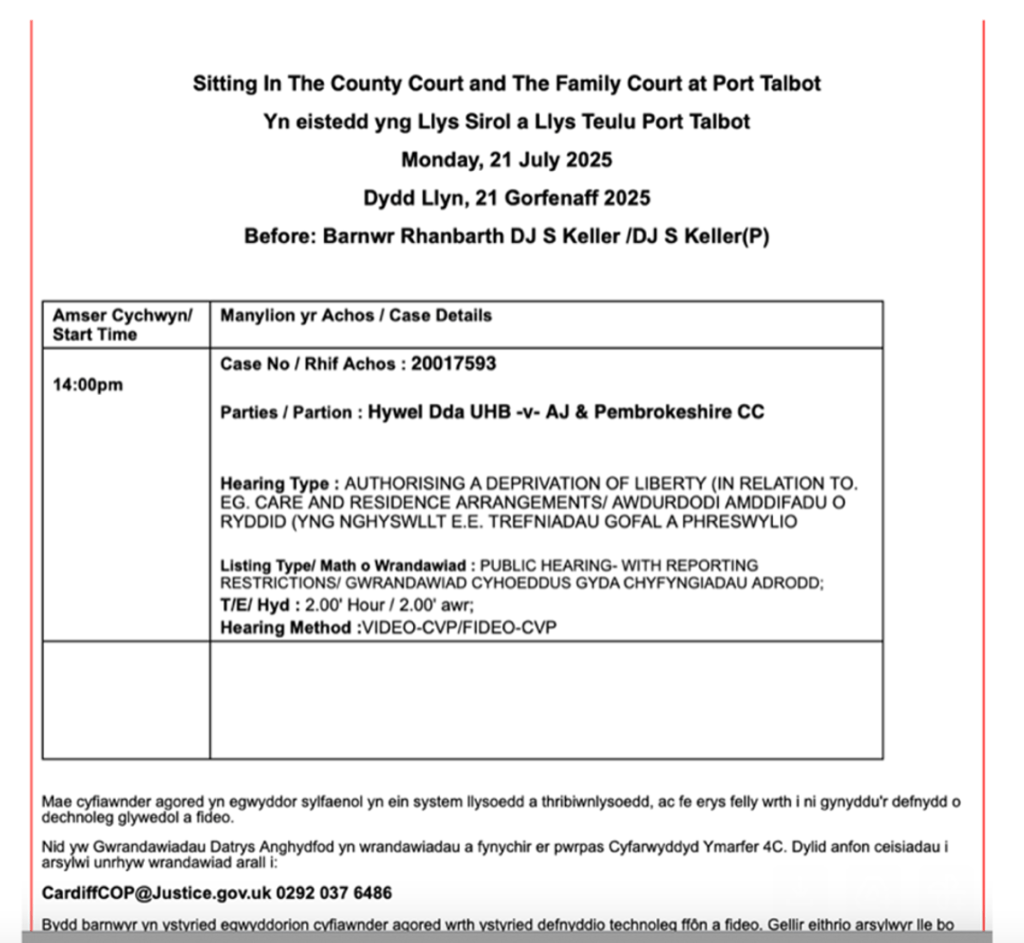
13:07 I request a Port Talbot hearing (2.00pm COP 20017593 before DJ Keller)
As the 2.00pm RCJ hearing has been vacated and so has the 2.00pm Hastings hearings – what else is there? I scan the lists again: it’s getting very late to ask for a 2.00pm hearing, especially as it’s now the lunch hour. I am not optimistic about this, but it’s worth a try.
There are 2.00pm hearings in Walsall, Reading, Horsham and Port Talbot. I pick Port Talbot for no particular reason except that I don’t want to bother staff at hubs I’ve already contacted today, and not remembering quite which those were by this point of the day and in the scramble to find another hearing, one thing I do know is that Cardiff (the hub for Port Talbot) wasn’t one of them. I’m stressed out, and anxious about getting something wrong.
I also know that we’ve experienced repeated listing problems with Port Talbot (e.g. hearings have taken place without ever appearing on the COP list in CourtServe, and when they do appear they are often missing essential information) so I thought it might be helpful, from a transparency viewpoint, to observe a hearing there – if it turned out to be possible.
In fact, today’s Port Talbot listed hearing has all the necessary information – including the names of the public bodies (Hywel Dda University Health Board and Pembrokeshire County Council) and the issues before the court (“Authorising a deprivation of liberty in relation to e.g. care and residence arrangements”) – although again this turns out not to be quite accurate for this case, which now also (I discover later) concerns the validity and applicability of an Advance Decision to Refuse Treatment, a matter I’m particularly interested in.
13:08 Counsel from the Hastings case sends me a “case summary” (“I attach the case summary as promised”). I leave it until later. – I’ve got information overload and am beginning to get confused about which hearings are which, while also wanting to make best use of my time. I’m still looking through the lists, trying to decide whether to apply for another hearing as well as the Port Talbot one for this afternoon, especially if there’s one due to start at 3.00pm or later.
13:09 I request a 3.00pm hearing before DJ Buckley in Reedley (where’s Reedley? It’s in the Manchester hub and I find it on Court Finder (here: https://www.find-court-tribunal.service.gov.uk/courts/reedley-family-hearing-centre). This is a better option than asking for another of the 2.00pm hearings (what if I get both!?) and a 3.00pm hearing gives everyone a bit more time to get me the link and the Transparency Order. I see that the 2.00pm in Port Talbot – the one I’ve already asked for – is listed to last for two hours, so if I get both the Port Talbot and the Reedley hearings, I might find myself double-booked). Fingers crossed it works out somehow.
13:12 I’m told the Reedley hearing has been vacated. The “Administrative Officer” from the Manchester hub says: “The hearing for this matter has been vacated. The parties filed an agreed order, which the Judge has approved.” At least I got a swift response to that one!
13:21 I receive the Transparency Order for the Port Talbot hearing: “Thank you for your request to observe the hearing before District Judge Keller at 2pm on 21st July 2025. The link to the hearing will be sent to you from the hearing court and the transparency order is attached to this message.” This is looking positive! I read through the Transparency Order. It’s in the standard form (with no prohibition on naming public bodies) – that’s a relief!
13:32 I receive a Position Statement from Exeter: it’s the one on behalf of P by her litigation friend the Official Solicitor. It has the wrong case number on it: instead of the number in the listings and on the Transparency order [20014381], it’s given as 20014881 – so an ‘8’ where an ‘3’ should go as the sixth digit. (This matters because I use case numbers to search for information on my computer and errors like this mess up my search system!). I haven’t received a Position Statement from Devon County Council (nor, perhaps unsurprisingly, from the two lay parties, who are litigants in person). The Official Solicitor’s Position Statement provides me with some information about the case (as I reported earlier) which is about possible financial abuse by someone holding Lasting Powers of Attorney (there are also suspicions relating to a fraudulent last will and testament). It looks interesting, and I’d like to observe it when it’s back in court before a different judge. I email the lawyer who sent me the Position Statement, thanking her for sending it and asking whether she can tell me the date on which the case will now be heard. No answer. If I have to search the listings manually (only journalists can use “alerts” to tell them when a hearing comes up), it will be hit and miss as to whether I locate it. Frustrating! There’s a chance that the new date of listing will be included in the approved Order (if there is one) from today’s hearing, so I decide to ask for that, and make a note to do so this evening when things are less pressured and I’m not having to juggle all these requests. (I then grab a sandwich!)
13:51 I chase the link for the Port Talbot hearing (listed to start at 2.00pm) “I haven’t received the link yet…”
14:03 I receive the Health Board’s Position Statement for the Port Talbot hearing. Counsel for the Health Board sends me their Position Statement, having been forwarded my request by the court staff. I tell the lawyer that I don’t have the link yet – he tells me the hearing will now start “not before 14.30”. Nobody had told me that!
14:15 I receive the Port Talbot link from the “PTJC Family Team” (I think PTJC stands for Port Talbot Justice Centre). I join the platform and am “waiting for the conference host to join”.
14:20/14:24 I receive the Official Solicitor’s Position Statement for the Port Talbot hearing. Counsel for P via the Official Solicitor contacts me to say “I’ve received your request for the PS in the above case. I’m told you have a copy of the Transparency Order – can I check that’s right before sending the PS?” I confirm I have the Transparency Order, and he sends their Position Statement. Since the hearing hasn’t started yet, I’m able to read it in advance.
14:29 I request a second Position Statement from the Official Solicitor in the Port Talbot case – the one prepared for an earlier hearing in the same case (a week ago). “Please may I also request a copy of your PS referred to in §3 of the PS you’ve just sent me, since that would appear to provide some useful background. (And I quote the relevant paragraph 3: ” The court is familiar with the background to this case. A summary of events between 10/08/2023 and 10/07/2025 appears between paragraphs 6 and 22 of the position statement filed by the litigation friend for the second directions hearing [12-15].”). He tells me it will need to be anonymised and says he’ll do it before the hearing if the start is further delayed; otherwise, he’ll send it afterwards. (More work for a busy lawyer!)
14:32 The Port Talbot hearing starts: A distressed 90-year-old, treated against her wishes and discharged to a care home – and the validity and applicability of her Advance Decision to Refuse Treatment
It turns out the order is agreed by everyone. The judge asks the applicant counsel to go through the recitals on the chronology. This covers information that I later see is given in full in the earlier Position Statement from the Official Solicitor, so I’m confident in reporting it here.
The protected party is now 90. Prior to admission to hospital in March 2025 she lived at home alone, near her daughter. On 10th August 2023, she made an Advance Decision recording that she refused any treatment that required her to go into hospital “even if my life may be at risk from this refusal”. On 6th March 2025, she was admitted to hospital (the Health Board says they didn’t know about her Advance Decision to Refuse Treatment) with abdominal pain and discharged home nearly a month later on 3rd April 2025 – but was returned to hospital by ambulance during the night of 3rd/4th April 2025 due to concerns from a domiciliary carer. She was assessed as lacking capacity (capacity for what was not specified), following which a s.21A Court of Protection application was made. At a best interests meeting there was a “patently unlawful” analysis resulting in P’s discharge to a care home on 30th June 2025, without the approval of the court being sought, and without P being present or represented at the meeting. She’s already lost 2 stone in weight at the hospital and is continuing to lose weight at the care home. On 10th July 2025, the litigation friend visited P and found her “confused”, not eating (her body mass index was around 16.88) and saying that she “wanted to die”. The Official Solicitor is “shocked by what has happened” and “astonished by what [P] has undergone”. The Position Statement records: “She is an extremely vulnerable woman who deserved (and deserves) the protections of this Court. Instead, she is in a placement to which she has voiced objections for years and in which she is confused, fearful and acutely vulnerable”.
The judge went through the agreed order (I’ve requested but not yet received it). It puts in place what’s needed for another hearing to decide on the scope of P’s Advance Decision to Refuse Treatment – in particular what it means in event of any future medical emergency – and her wishes and feelings, as they relate to the s.21A application. There was a brief exchange about what might happen if her BMI (now in the region of about 15) causes concern to the extent that a naso-gastric tube, or PEG tube, is considered medically necessary before the case comes back before DJ Keller in Port Talbot. I think I understood that an urgent application to a Tier 3 judge in the Royal Courts of Justice would need to be made.
It wasn’t straightforward to arrange the date of the next hearing (“My lists are (sigh) well, let’s just say impossible” said the judge) but it’s eventually fixed for 21st August 2025, for 3 hours.
I am really keen to observe the next hearing. I have a special interest in Advance Decisions to Refuse Treatment (ADRT) from a personal perspective as I have made one myself (I wrote about it here: Determining the legal status of a ‘Living Will’: Personal reflections on a case before Poole J) and I’m dismayed that the issue with the ADRT was not included in the public listing. If it had been stated in the listing that the issues before the court included the ADRT, this would have been my first choice of hearing – rather than simply the one I ended up with after all the others I’d asked for were vacated. I so very nearly missed knowing about this case altogether due to inadequate listings. That’s not transparency – and I wonder how many other ADRT cases come before the court, but I never learn about them.
The hearing finishes at about 14.40
14:41 I receive the earlier Position Statement for the Port Talbot hearing from the Official Solicitor (which I’ve relied on in reporting the “chronology” above).
That evening (between 9pm and 10pm), I requested the approved orders from the Exeter, Hastings, and Port Talbot cases. As my requests are virtually identical except for the case number, here’s the email relating to just one of them (Port Talbot):
The next day (22nd July 2025), I received an email from court staff about the Exeter hearing (the one vacated to find a different judge) saying “Thank you for your email which I have referred to the Judge. He has asked me to email you a copy of the order when it is sealed. He has not yet received a draft from the parties.” In the week or so since observing these hearings, I’ve chased all three orders but not yet received any of them.
That’s it for today’s hearings. Two hearings successfully observed! I’m hoping for more documentation to support my understanding, follow-up and accurate reporting of them in due course.
UPDATES on approved orders
Port Talbot
- 31 July 2025: “The Court currently have a backlog of orders due to staff shortages. We have made a note on the file to serve you with a copy of the order as soon as it is processed. We will get this to you as soon as we are able.”
- 5th September 2025: I receive the Port Talbot order, and have since observed a next hearing in the case which I’ll blog about.
Hastings
- 23rd August 2025: I chase the order. “I’m sorry to bother you again but I seem not yet to have received the approved order in this case.”
- 5th September 2025: “The order has not been sent because it has been referred back to the judge. We are currently waiting for judicial instructions.“
- 20th October 2025: “We apologise for the delay in sending you a copy of the order made following the hearing” – the order finally arrived – three months after the date of the hearing.
Reflections: The high cost of open justice
The two hearings I watched (in Hastings and Port Talbot) concerned matters of significant public interest – and all three cases I learnt about (including the Exeter case that was adjourned) involved the court performing a protective function in relation to an elderly person: appointing a son as Deputy (Hastings), seeking to establish both the validity and scope of a person’s advance decision, and her best interests regarding treatment, residence and care (Port Talbot) and replacing an (allegedly) exploitative attorney with a court-appointed Deputy (Exeter). They all concern the application of statutory instruments (LPA, Deputyship, ADRTs) in the real world. They all relate to how the courts determine best interests when things seem to be going wrong. They really matter to members of the public in our own lives.
- The Hastings case concerned an elderly man who (counsel suggested) may have been financially exploited as he lost capacity to manage his own financial affairs, while he also refused – and apparently continues to refuse – to acknowledge his own diminishing capacity and declines his son’s offer to act on his behalf. This is a familiar scenario for many people with elderly parents – and it’s a possible future scenario for all of us as we grow older and lose cognitive abilities we’d previously taken for granted. There is a legitimate public interest in understanding that people can be in this situation and that the court can help (even when the vulnerable person doesn’t want help) by appointing a Deputy (see ss. 15-21 Mental Capacity Act 2005).
- The Port Talbot case concerned an elderly woman who, it seems, had taken all the right steps to prevent hospital admission toward the end of her life, using a statutory instrument (the Advance Decision to Refuse Treatment [ADRT], defined in ss. 24-26 Mental Capacity Act 2005) that is legally binding on health and social care staff (and everyone else) if it’s valid and applicable. Nonetheless, she was admitted to hospital and then discharged (after a failed return home) to a care home where she is distressed and saying she wants to die. Presumably P’s daughter was also unaware of this ADRT, or at least of its legal implications. There is also strong indication that the proper best interests procedures (s. 4 Mental Capacity Act 2005) were not properly followed. The public has a legitimate interest in knowing that a public body is being criticised for its actions in this way. There have been several cases lately concerning NHS bodies over-riding people’s ADRTs (quite often – initially at least – because they were unaware of the existence of these documents), and then disputing their validity and applicability (e.g. Re AB (ADRT: Validity and Applicability)). Those members of the public who want to plan ahead for possible future lack of capacity by making ADRT and Advance Statements have a right to know how these matters are decided by the court.
- The Exeter case, the one I didn’t get to observe although I was briefly admitted to the video-platform, also turns out (from what I’ve read of the Position Statement) to concern matters of legitimate public interest. Planning ahead for lack of capacity can include appointing someone else to make decisions for you while you still have the capacity to do that (Lasting Power of Attorney, ss. 9-14 Mental Capacity Act 2005). But cases of abuse by LPAs are frequently reported in the media, and it seems to be the suspicion of abuse that led the Attorney in this case to “disclaim” (resign) from that role. There are moves to appoint a Deputy (a court-appointed representative) to replace the person believed by the public body to have been abusing their position. I hope I might get to observe what happens next (though the listing system will militate against that being possible for me).
- UPDATE on the Exeter case: On 14th August 2025, this case was heard in private and without notice to one of the parties (I assume the alleged abusers). It was was listed as a “closed” hearing on the Royal Courts of Justice listings page (see image below) – and I wasn’t available to observe it even if it had been a public hearing, which it wasn’t. (“Applications in Court as in Chambers” is legalese for a private hearing with no members of the public permitted to observe. If I’d been free to observe, I would probably have sent an email to the judge asking for special permission to observe it – permission has been granted to me to observe a “closed” hearing in a different case (see “A committal, a closed hearing, and forced removal of P“). The fact that proceedings were “closed” (i.e. a party was excluded by judicial order) makes this case of even more public interest, because it departs from the usual expectations of “a fair trial” by deliberately disadvantaging the excluded party. Lawyers often tell us that “closed” (or “ex parte”/”without notice”) hearings are very rare – but we keep stumbling over them – as is illustrated by the fact that this one turned up amongst the random selection of hearings I picked today. This one is perhaps unusual in having been listed as a closed hearing: many closed hearings take place without ever being publicly listed (for fear of alerting the excluded party).
In sum, the value of open justice is clear. What I observed showed me how the court works (and what it’s up against) with the kind of detail, clarity and vividness it’s impossible to convey in a published judgment. I doubt, anyway, that there will be a published judgment from any of these cases: judges simply don’t have time for that. If I hadn’t been in court, none of these cases would have been reported. Nobody else was there to observe. There’s hardly ever a journalist in a Court of Protection hearing. Justice might have been done – but nobody would have been there to see it being done.
The problem is that I only got to observe – or at least learn about – these three cases by dint of an extra-ordinary knowledge-base (shared by very few others) about the daily practical workings of the court; and because I have more time, persistence, and perhaps sheer bloody-mindedness in pursuing links than anyone else I know. I completely understand why most people simply give up. And why journalists, for whom time is a paid-for commodity, don’t “waste” it by trying to gain access to Court of Protection hearings. There was nothing unusual about my experience on Monday 21st July 2025. It’s always like that! If anything, the unusual thing is that that I actually did succeed in observing two hearings – many days I’m unsuccessful.
In pursuit of what turned out eventually to be observation of two short hearings (a 20-minute hearing in Hastings and one of about an hour in Port Talbot), I sent more than 30 emails over the course of the day and (excluding automated responses) received around the same number in return. I corresponded with six different members of court staff and three different lawyers across five different courts. Behind the scenes, there were also emails between staff members about my requests to observe, as staff at each of the “hubs” forwarded my requests to the regional courts at which the hearings were taking place (so Bristol staff corresponded with Exeter, Birmingham staff with Stoke on Trent, Reading staff with Hastings, Manchester with Reedley, and Cardiff with Port Talbot). Additional internal emails passed between staff responsible for lists and staff with responsibility for audio-visual links. There was further correspondence (I was told) between judges and lawyers about my requests for Position Statements, and more again in relation to my application for a variation to a Transparency Order. Overall, my day’s work must have involved well over 100 emails.
This is all a massive amount of time and effort – especially against the backdrop of the dire situation described in automated emails I received: “HMCTS staff are working under significant pressure due to a lack of staff and the current urgent need to triage, list, vacate, and re-list cases” (from the automated reply to my emails to the Reading hub). During the course of the hearings, I also noted a comment from one judge about his “impossible” (overbooked) lists, and, from another judge, a reference to the scarcity of staff meaning that ushers are having to cover several different court rooms simultaneously. Again, this is absolutely normal in my experience – there are frequent references to the pressure everybody is working under. Despite this, everyone I corresponded with was unfailingly courteous and as helpful as they could be under the circumstances. Thank you!
The chair of the judicial transparency board, Mr Justice Nicklin has recently promised “Open Justice Champions” to support transparency. He says: “The board and HMCTS are aware that there can be issues with people gaining timely access to remote hearings. HMCTS are working to provide “Open Justice Champions”.’ The regionally based champions ‘will provide a single point of contact to assist in resolving open justice issues”. Would “Open Justice Champions” have helped me? Perhaps I’m being over-sceptical, but I can’t see what they would have known that I don’t already know, or what they could have done that I didn’t, especially if they were regional specialists, rather than specialists in the Court of Protection. Presumably I’ve had needed to contact several different champions for the different regional courts, e.g. the Welsh champion for Port Talbot and the North West champion for Reedley – even though I wanted to navigate access to one or the other hearing, but not both since they were listed to run in overlap. Would they liaise with each other to support me? Would it just add another set of duplicated emails into the mix? These “champions” will apparently be mid-level civil servants responsible for giving people resources and information to assist with transparency but it’s unclear what training they’ll have, and it seems they’ll be doing this work as part of their usual jobs. The Ministry of Justice has said: “There is no new funding for these roles. The skill of understanding open justice and enacting open justice is already an expectation of employees in the MoJ”[3]. So, when it’s confirmed that they’re in place, perhaps I’ll contact a “champion” when I don’t get a link in time – but forgive me if I’m doubtful about the value of doing so. Perhaps they will prove me wrong.
In my role with the Open Justice Court of Protection Project, I would love more members of the public to observe Court of Protection hearings – but be warned, this is what you are letting yourselves in for. And imagine what it might be like for HMCTS staff, lawyers and judges if more of us asked to observe court hearings, with the resultant increase in email traffic and an increased need for links and Transparency Orders and anonymised Position Statements, all to be sent to each one of us individually. There have occasionally been dozens of observers in hearings held in the Royal Courts of Justice (which is much better resourced) – but it’s simply not a workable proposition for the regional county courts like those I observed in today.
And a message to lawyers and judges: please appreciate what it can take to get access to your hearings and understand why we might seem stressed or anxious (especially if we’ve also had to dash off an email about varying a Transparency Order in advance of the hearing). Don’t assume that we’re being disrespectful or careless if we make “late” requests, or arrive at a hearing after it’s started, or seem to be hassling you for orders or position statements, or don’t understand what’s going on. Like everyone else, we are doing our best under difficult circumstances.
My impression is that this is a system that is not merely under-resourced and struggling, but one on the brink of collapse. Transparency puts a huge strain on an already over-burdened justice system. It’s not surprising that the judicial commitment to transparency is more aspirational than can be realised in practice. Perhaps, with proper investment in the justice system, it might be possible to create effective lists, searchable by the public, with accurate information about issues before the court so that we can pursue topics we’re particularly interested in or knowledgeable about (like me and ADRTs). Information about vacated hearings might be swiftly conveyed on a public online platform so that we’re not endlessly chasing links. There might even be downloadable anonymised case summaries or Position Statements online (and displayed via QR codes on courtroom doors) so that we don’t have to pursue individual court staff and lawyers (and sometimes judges) to get access to them. I gather there may be practical (and statutory) impediments to implementing some of these suggestions –but there is no point in devoting time to considering how those impediments might be overcome so long as there is no money to implement them in any event.
Until the justice system is properly resourced, the reality for public observers (and everyone else) in the Court of Protection will be the arduous, costly, stressful and unsatisfactory experience I’ve described here.
Celia Kitzinger is co-director of the Open Justice Court of Protection Project. She has observed more than 600 hearings since May 2020 and written more than 100 blog posts. She is on LinkedIn (here), and also on X (@KitzingerCelia) and Bluesky @kitzingercelia.bsky.social)
Footnotes
[1] There’s recent Guidance from Mr Justice Poole on provision of Position Statements to public observers here: AB, Re (Disclosure of Position Statements) [2025] EWCOP 25 (T3) (15 July 2025). I was seeking to comply with that.
[2] For example: “MPs hear call to end ‘alarming’ abuse of elderly through powers of attorney”; “Pensioner evicted 94-year old father…”; “Mum trusted to be power of attorney stole £32,000 from ill grandmother to fund gambling addiction”; ‘Woman accused of £85,000 fraud while acting as power of attorney”
[3] Quoted in Charlie Moloney “Courts to have ‘open justice champions’” (5th June 2025) and Charlie Moloney “No new money for ‘open justice champions’(11th July 2025)