Celia Kitzinger and Gill Loomes-Quinn, 15th June 2021
One year ago today, on 15th June 2020, we launched the Open Justice Court of Protection Project, a child of the pandemic.
It was born of our passionate belief that “publicity is the very soul of justice” at a time when it seemed that the public health emergency was closing down the opportunity for people to observe the court in action.
Before the pandemic
We’d both had the experience of walking into courtrooms to observe hearings as members of the public. Serious medical treatment cases have always been held in public. As part of her work with the Coma and Disorders of Consciousness Research Centre, Celia had previously attended around 20 hearings in which judges made decisions about whether or not to continue life-sustaining treatment for people in vegetative or minimally conscious states. Gill had spent a month of 2017 in London observing hearings in First Avenue House as part of her PhD research – many (like the one she blogged about here) concerning Deprivation of Liberty.
These hearings concern fundamental human rights issues: the right to life, the right to family and private life, the right not to be arbitrarily deprived of liberty. Gill wrote:
“For disability rights activists, the transparency agenda affords us new opportunities to strengthen and inform our activism. So much of our experience of oppression – of discrimination, and of bureaucratic intransigence – happens behind the closed doors of doctors’ consulting rooms, or of local government offices. But here, in the Court of Protection, it is played out before the authority of the court, and now, before us – the public. Shining a light on collective injustice might be the first stage to challenging and changing it – if we can seize the opportunity.”
Before the pandemic we had found the doors of the Court of Protection wide open, and now it seemed they would be closing again.
Closing the courtroom doors
On 23rd March 2020, after the Prime Minister’s address to the nation, the Lord Chief Justice announced that (with urgent exceptions) “no hearings that require people to attend are to take place in any County or Family Court until further notice”.
On 31st March 2020, Mr Justice Hayden reiterated that guidance for the Court of Protection and published a protocol for remote hearings (via phone or video-link). The template order states they “shall take place in private” and any previous transparency order (permitting public access) “shall be disapplied”.
For remote hearings, Mr Justice Hayden considered the usual practice of making hearings public (as set out in Practice Direction 4C) to be “unworkable”. He considered that the right to freedom of information could lawfully be restricted in this way since it was necessary for the protection of public health (Article 10(2)).
But as Vice President of the Court of Protection, Mr Justice Hayden is deeply committed to transparency, and even as he (in effect) closed down public access to the courts, he included a section in the Guidance reaffirming the importance of transparency, with the opening sentence: “The culture of the COP is one of transparency, and I am determined to maintain this insofar as possible” (paras. 54-64).
He left open the possibility of public access, despite the new default “private” nature of all hearings:
“In each case active consideration must be given as to whether any part of any remote hearing can facilitate the attendance of the public, if so Practice Direction 4C may be applied and the transparency order reissued.” (para. 59, Guidance 31 March 2020)
It was that ‘loophole’ (that’s how it felt) that we exploited in setting up the Open Justice Court of Protection Project.
Launching the Project
On 17th March 2020, Celia attended the first ever remote hearing in the Court of Protection, held over Skype for Business. She did so not as an “observer”, but in a voluntary capacity to support “Sarah”, whose father was at the centre of a serious medical treatment case. It was a brutal experience in which an already deeply-distressing situation for Sarah was made much worse by use of remote technology.
Horrified by the idea that future hearings would be equally alienating and distressing for family members, Celia decided to try to observe other remote hearings – and succeeded, against the odds, in mobilising the “Transparency” section of Mr Justice Hayden’s Guidance to gain entry to 19 hearings in May 2021.
This took huge persistence and determination and the willingness to deal calmly with frequent rebuffs. She sent over 100 emails, and had more than 30 phone calls with court staff, to gain access to these 19 hearings. The request to “observe” was often misheard over the telephone: “You want to what? To adjourn?”. Once the request was understood, she was usually simply told that hearings were “private”. There was correspondence from some judges who said the same thing. She was cross-questioned repeatedly about why she wanted to observe and had repeatedly to explain and defend the principle of open justice (to the judiciary!). Celia blogged about the first of these 19 cases (it was before Mr Justice Hayden), and tweeted about others – and we quickly realised that there was a surprising amount of public interest, at least from our own followers on social media.
It also became apparent that remote hearings potentially offer increased access to the court. People don’t have to travel to attend. We can watch hearings across England and Wales from the comfort of our own homes. Far from closing down open justice, the pandemic had opened up a new means of supporting it.
Gill suggested a pandemic project: “Let’s create our own website, blog about some hearings, and encourage a few others to do the same”. We invented some “aims” for the project, created an email account, set up a website, wrote a “welcome” page and pressed the button to launch it. And so the Open Justice Court of Protection Project began.
We said:
A key aim of the project is to raise awareness of the work of the Court, and its social impact. Blog posts covering observations by Public Observers, analyses of published judgments, and other social and legal commentary will be at the heart of how we go about achieving this aim. (Welcome page, 15 June 2021)
We had no funding, and no institutional backing (then or now). We were just two people with experience of the Court of Protection, who cared passionately about open justice in a court which makes draconian decisions in relation to the human rights of some of the most vulnerable people in society. We imagined the Project would be something of a niche interest.
We had some time to create a project like this because many of our usual activities had been cancelled (or “postponed’) due to the pandemic – and at that point it was widely-believed that life was simply ‘on hold’ for a few months and that we would give those talks, attend those conferences, run that training, meet those students in person, after a short delay. We assumed that things would soon go back to ‘normal’, we’d get back to our usual business, and our Project would have been a brief intervention to support transparency at a particularly challenging time.
Two weeks later, we were forced to reassess. We were (as we said) “overwhelmed” by the response, as more than 70 people had contacted us for help with observing hearings. And three family members involved in upcoming Court of Protection hearings had also emailed, asking whether we would observe ‘their’ hearings.
Within the first two weeks of the Project, by the end of June 2020, we’d published seven blogs based on public observations of court hearings: by two future barristers (here and here), a third sector worker, a speech and language therapist, an MCA trainer, a nurse, and a family member of someone with an impairment in the functioning of mind or brain.
On 1st July 2020 we published the first of our ‘collective’ blog posts. Seven people who had observed the same hearing (seven members of the public observing simultaneously was virtually unheard of back then!) were welcomed by Mrs Justice Lieven who “thanked us for attending … and pointed out that it’s not “open justice” if nobody comes”. We were a varied bunch, including a clinical psychologist, an academic lawyer, and a family member currently involved in an “intimidating” COP hearing of his own. During July 2020, observer-bloggers included a trainee solicitor, a case manager, a social worker, a DOLS Manager, and a trainee IMCA. We were realising the range and scope of interest in observing these hearings. The Project was turning out to be less ‘niche’ than we’d thought.
During this period, we were confronting multiple access problems – including four days during which the email to request access to hearings at First Avenue House had been mistyped on their webpage (so emails were bouncing back) and contact details were missing from the listings for many hearings in regional courts. We had somehow created the impression that we were a big organisation with the resources and connections to solve access problems for members of the public. All we could do was email the courts on their behalf.
We learnt from the blog posts (and informal feedback) that once people overcame the hurdles of access, they were struggling to understand what was happening in court. It became apparent to us how much we already knew about court process and procedures, and that observers without previous experience in court were struggling. The barriers to open justice are not just barriers to access, but extend to legal jargon and obscure court procedures. As speech and language therapist, Olwen Cockell, wrote in one of the earliest blog posts we published: “I could see justice being done. I could hear justice being done. But, hand on heart, I can’t say I fully understood the justice being done.”
So, we enlisted the help of some lawyers and published some ‘explainer’ blogs: A basic guide to the Court of Protection(Alex Ruck Keene); Who’s who in the Court of Protection? (Victoria Butler Cole QC) and what’s in the ‘bundle’ (Kyle Squire). Celia wrote a blog about the reporting restrictions order (here), because several observers simply refused to write blogs, believing they were not allowed to say anything at all about the hearings. We’ve continued to develop these ‘explainer’ blogs, because being in court without understanding what the judge and counsel are talking about can feel a bit like being a child having adults talk ‘over your head’ in sometimes deliberately obfuscatory language, designed to exclude you. We also tried to ‘humanise’ the court, by publishing a more ‘personal’ account from a Court of Protection solicitor about her lived experience and its relation to her professional expertise.
But what most struck us two weeks after pressing the ‘launch’ button, was how positive observers were about the court – most especially in their appreciation of the huge emphasis the Court places on the autonomy of the disabled people at the centre of its work, and of individualised, person-centred decision-making. One observer (who herself advocates for a family member) said of the hearing she witnessed:
“The law enabled a person with a learning disability to access the same rights and healthcare as any other citizen. This gives me a huge sense of relief that my family member will be safe and listened to with these structures in place, and free to live the life he chooses.”
Others made similar points:
“My main focus is that the person remains at the centre of everything. It was so reassuring to see that this also was the primary focus within a formal court hearing for Mr Justice Hayden” (Sara Shorten).
“What I saw happen in this case, was a serious focus on getting things right for the individual person at the heart of it all” (Meriel Scott)
“Mr Justice Williams maintained unwavering focus on what is right for P … I left feeling reassured that person-centred decision-making, an issue I feel strongly about, prevailed.” (Upeka de Silva).
In some ways this was unsurprising: we have both seen good practice in the court. In other ways, it wasn’t necessarily what we were expecting – especially given our own critiques of some of the underlying principles of the Mental Capacity Act 2005 (particularly the concept of ‘best interests’) and our own experience of some very bruising encounters in the Court of Protection. It was also becoming very clear that these blog posts, written by members of the public, presented a version of the Court of Protection that is very different from media representations: they were more personal, more reflective, and more engaged with the challenges of how to do the ‘right thing’ for the person at the centre of the case.
A year of open justice
A year on, we have a much bigger project on our hands than we ever predicted and no indication that we can stop any time soon.
We simply didn’t predict the degree of interest and enthusiasm the project has stimulated, or the extent to which the project has encouraged and supported people from a range of backgrounds (including health and social care professionals, lawyers, and people who are themselves engaged in ongoing proceedings in the Court of Protection) to observe the court in action, and to share their experiences and their reflections via our blog and social media. In the past year we have published 139 blog posts featuring 97 different authors. As it became clear that hundreds – now thousands – of people would be involved in our Project (way beyond our original estimation of maybe a blog every couple of weeks or so), we also had to develop a formal ‘policy’ about what we would and wouldn’t publish (here) and some guidance for bloggers (here).
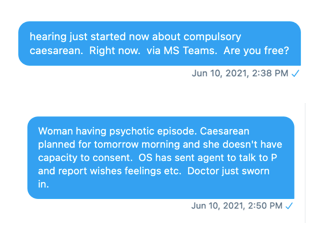
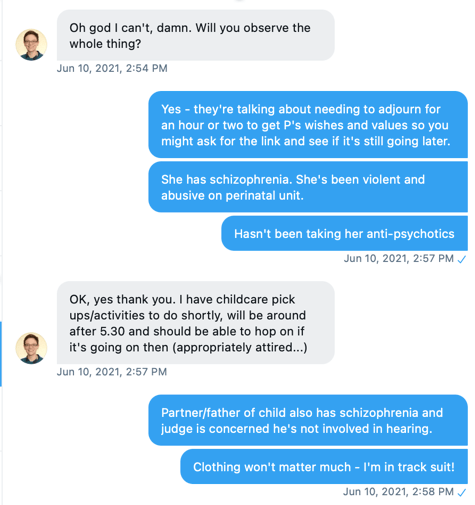
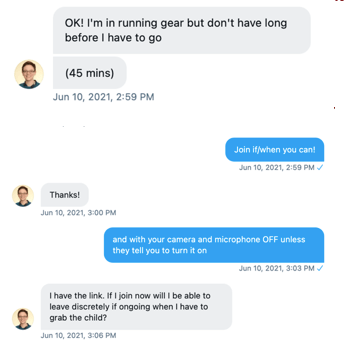
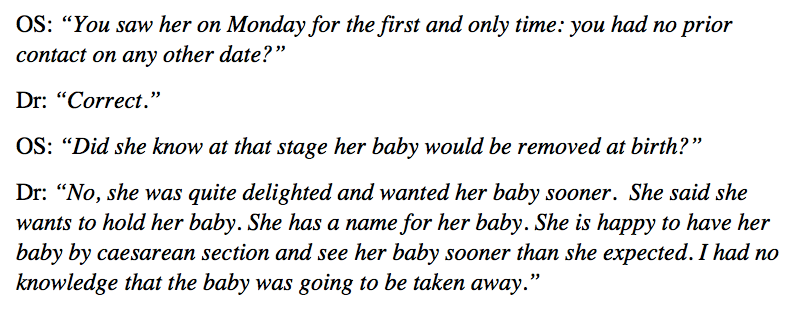
Recently we’ve also developed tweet threads (collected as pdfs on our web page here) as a method for reporting on some of the hearings we observe. Initially this was simply a means to get something out publicly about a hearing when time-pressures precluded writing a blog – but we realised subsequently that tweet threads are a mode of communication which turns out to be extraordinarily effective in promoting dialogue and discussion with people who’ve not previously engaged with the Project. (Note: the pdfs on our webpage don’t include replies to tweets – to find them, and appreciate the engagement they promote, copy some of the text into the search facility in Twitter, to locate the original tweet thread and responses to it).
The day-to-day work on the Project includes our own observations of the Court of Protection in action, editing and publishing blog posts and tweet threads, maintaining the social media presence of the Project and mentoring would-be observers, who sometimes need considerable support (as described by one contributor who mentored undergraduate students to observe).
Additionally, over the past year we have given 18 talks, seminars, and conference papers. These include: participating in a conversation about remote hearings with COPPA North-West (branch of the Court of Protection Practitioners’ Association); providing continuing professional development training for incoming judges to the Court of Protection via the Judicial College; contributing to the ‘Transparency Review’ being undertaken by the President of the Family Division of the High Court, Sir Andrew McFarlane, and presenting our work to the conferences of the Society of Legal Scholars and the Socio-Legal Studies Association.
In May 2021, we invited Claire Martin and Kirsty Stuart to join the project. Claire is a clinical psychologist based in Gateshead who works with older people; and Kirsty is a solicitor with Irwin Mitchell. Both had become involved with the project via writing for our blog, and subsequently giving talks about their experience as public observers. Both bring a wealth of complementary expertise, experience, and interests to the project.
The virtual ‘home’ of the Open Justice Court of Protection Project is our website. This is where we share details of upcoming hearings in the Court of Protection (‘Featured Hearings’), host supporting information and guidance for observers, including the resources in our Public Observer Wiki and our Hearing Feedback Form, designed to support observers in structuring and making sense of their observations. It’s also where publish our blogs and tweet threads.
The ‘reach’ of the website has surpassed our most optimistic expectations. During this first year of the Project, it’s had over 111,000 views from over 55,000 unique visitors, across more than 100 countries. This has enabled us to put into practice one of the key aims of the Project – that of supporting members of the public not only to gain physical (or virtual) access to the Court of Protection, but also to understand and engage critically with its work as informed ‘citizen journalists’.
We were delighted that in April 2021, the Open Justice Court of Protection Project was awarded the Mobilizing Research into Action prize in the Emerald Real Impact Awards 2020. It was brilliant to see the Project recognised in this way – and a great tribute to the contributions of the thousands of people who have been involved with it since it began: by engaging with the Project via social media; by observing the Court of Protection in action; by writing about their experiences for our blog; by sharing their expertise via our ‘explainer’ blog posts; and by inviting us to contribute to seminars, discussions and other events.
Reflecting back on the last year, there are four achievements we’re particularly proud of:
1. Changing the culture of the court
The Court of Protection now expects and prepares for scrutiny by public observers. This is especially so for Tier 3 judges hearing cases in the Royal Courts of Justice and judges at First Avenue House in London. Outside of London, judicial experience is more patchy (because public access is harder), but it’s many months since a would-be observer has been told that all COP hearings are ‘private’ or cross-questioned about their motives for wanting to observe.
When we started observing we were offered essentially ‘fly on the wall’ status – i.e. the court just went about its business pretending we weren’t there. Now, by contrast, there’s almost always an opening summary (usually from the applicant counsel, sometimes from the judge) about the background to the case and the key issues to be addressed. This is useful not just for us as observers but also for lay participants:
“It’s good practice to have to think ‘how can I summarise this case in 2 minutes’ at the outset. I think it helps to do that in most cases anyway, but a public observer’s presence means we are more likely to have thought about it first. It aids the judge’s understanding and just as importantly the understanding of non-lawyer participants/litigants.” (Barrister)
We’re also now increasingly sent position statements on request: these skeleton arguments which outline the positions of the different parties at the beginning of the hearing are invaluable in supporting our understanding of what is going on. We’re hearing now that, knowing that their position statements may be requested and read by members of the public, some lawyers are trying to write them with more clarity and careful exposition of the law.
One barrister tells us that the presence of observers has meant a more rigorous focus on fundamental legal principles during hearings:
“There has been real enthusiasm for public observers in the Court of Protection. It has been seen as a real opportunity to counter the perception of it as a secret court. As a result, we have been taking the time to expressly set out the first principles and legal principles which should govern everything the Court does. This exercise, which was prompted by a desire to make the proceedings accessible and easier to follow has actually meant that as the principles are pushed to the forefront of everybody’s mind, they are more rigorously and consistently applied.” (Josh Hitchens, barrister)
Another barrister, reflecting on the difference it makes to have observers in court, says:
“It absolutely changes things – practitioners and judges are less sloppy I think, and take the time to properly set out the facts, the law and judgments when they might otherwise refer to things in a more shorthand way. This, I think, is a good thing since it means that anyone participating or watching (often family or even P themselves) can actually follow what is going on far better. It means we are all on ‘best behaviour’ essentially!” (Barrister)
2. Building a role as ‘critical friends’ to the court’s transparency agenda
We take as our starting point that (as Mr Justice Hayden says) “the culture of the COP is one of transparency”– meaning that the principle of transparency is a judicial commitment and aspiration. Putting that principle into practice requires our help – since obviously justice is not open or transparent if we can’t get through the door of the (virtual or physical) courtroom, or don’t understand what’s happening when we do.
Supporting the court in its commitment to the principle of transparency means both celebrating the success of open justice, as in many of the blogs on our website written by people who’ve attended hearings, and – equally – identifying and reporting the problems the court appears to have in implementing this principle.
We know that the court is under-resourced, and working hard (especially during the pandemic) to deliver justice as speedily as it can, against a backdrop of challenges in relation to health and social care. We know that public observers create more work for the court: starting with the processing of emails from observers to court staff, and often culminating in a last-minute flurry of emails between counsel and judge. Lawyers need to be prepared to anonymise documents, prepare an oral summary and a transparency order, inform P and P’s family that observers will be present, sort out the video-platform link, or – with telephone hearings -individually dial us into a conference call (it’s often the judge who does this). And time is taken up in court with additional explanations of legal concepts for the benefit of observers, or by reading out material from documents to which observers do not otherwise have access. There is clearly a cost to implementing the principle of open justice in practice. We do not seek to minimise the fact that transparency is a burden on the court
Since, however, the principle of open justice is – in the first place – a judicial commitment (albeit one we support) and one the courts have historically held to be crucial in a democratic society, we are surely entitled to expect that the courts will do whatever they can to bear that burden graciously. It is the judiciary who have championed the idea that “open justice lets in the light and allows the public to scrutinise the workings of the law, for better or for worse,” as Toulson LJ put it. Or, as Lord Dyson JSC said, “the open justice principle is not a mere procedural rule. It is a fundamental common law principle.” When we ask to observe hearings, we are doing our bit to support and make concrete reality one of the principles the judiciary has advanced as core to its practice.
Balancing our sense of ‘entitlement’ to attend public court hearings with the practical reality that we are frequently excluded from them is at the core of our engagement as ‘critical friends’.
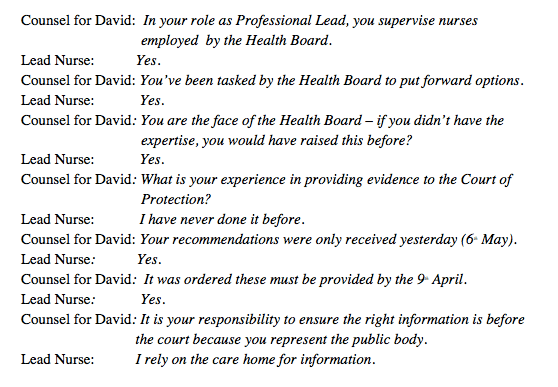
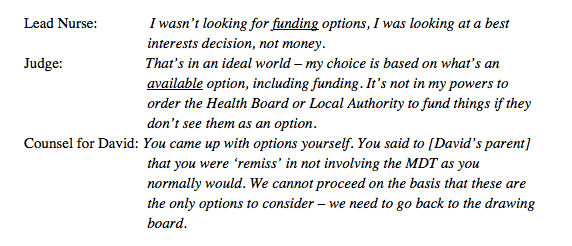
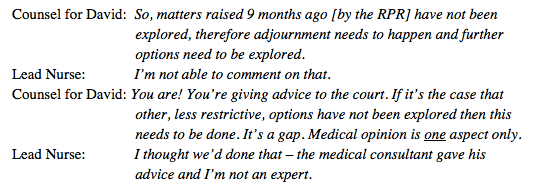
3. Scrutinising expert evidence
Our most frequently read blog post is “When Expert Evidence Fails” (viewed almost 5000 times). In essence, a consultant psychiatrist gave evidence that P, a 68-year-old care-home resident with dementia, lacked capacity to make her own decisions about engaging in sex (and various other decisions). The blog post describes – with examples of dialogue from the court hearing – how his testimony simply collapsed under cross-examination.
When the case returned to court three months later, with a different expert witness, it was deemed that P did in fact have the mental capacity to engage in sexual activity. As we pointed out, the tragedy is that P “who has a degenerative condition – so that time is of the essence for decision-making – has lost a whole year (during pandemic lockdown) of intimacy of any kind with her chosen partner. A year that she can never get back.” The human cost of expert witnesses getting it wrong in the Court of Protection is huge.
We also asked an expert witness to justify and explain the statistics he presented in court concerning the dangers of home birth (he blogged about this here) – since the published judgment quoted him without providing any references to his sources. We sometimes get the impression that the court is overly influenced by the particular individual expert before them, when other experts may have different interpretations of the evidence or draw on different evidence – and there is a problem, too, with using the same experts over and over again.
The most egregious case of expert evidence we have seen in the Court of Protection concerned a neurologist, Dr Pullicino – whose evidence the Court of Appeal said: “lacked every characteristic of credible expert evidence and it is not surprising that the Judge rejected it as effectively worthless”. His key evidence relied on 3 minutes of video recording of P, whose notes he had not examined, on the basis of which he made unsustainable diagnostic claims (as analysed in a blog post here).
After watching the hearing, and doing some background research, Celia wrote a letter of concern to the General Medical Council about Dr Pullicino on the grounds that he caused harm to the patient (and to his family) and damaged public confidence in the medical profession. They are currently investigating this.
So, open justice means exposing not just the lawyers, but also the health and social care professionals who provide evidence to the court (especially those who do so as ‘expert witnesses’) to public scrutiny and to the possible consequences of that.
4. Improving legal literacy and knowledge of the COP
We’ve both learned a lot about the law through watching Court of Protection hearings, and so too have the health and social care professionals, and aspiring lawyers, who have acted as public observers. Observation often has important benefits for continuing professional development:
“I have found the whole observation experience very beneficial. The googling, looking up of legislation, reading up of quoted case law – both during and after the court attendance – has given me a crash course in legislation, that I now realise, I only thought I understood. Listening to a talk about how the Mental Capacity Act is implemented in the courts is one thing – actually observing it as it happens is very different!” (Louise Burrell, social worker)
“I think the most important learning for me from being able to observe this hearing, is the way it has again, allowed me to watch the Mental Capacity Act 2005 ‘in action’ and understand how a senior High Court Judge … works through the process of reaching a best interests decision. I’m also able to take away with me some ideas that I can incorporate into my own practice when completing best interests assessments myself in future.” (Astral Heaven, DOLS Manager)
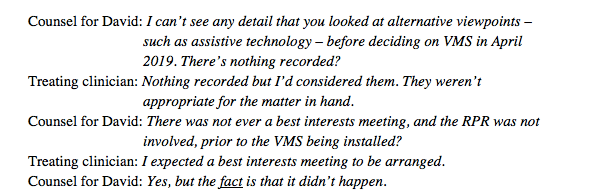
“For my part, I left [the hearing] with a resolution to examine my own practice, and to consider deeply the motivations for the clinical decision-making forums (e.g. Multidisciplinary Team Meetings) I am part of that do not physically place the person or their family at their centre.” (Caroline Barry, Consultant in Palliative Care)
“For me as a student of health care law, this experience of observing the Court of Protection in action illustrated the reality of applying the ideals of the Mental Capacity Act 2005 to real life. In theory, it’s easy to say that decisions should be made in P’s best interests, but even when – as in this case – everyone agrees what that is, judges have to deal with real-world issues like which rehabilitation unit would be suitable, how to find one with a vacancy in a particular area, how to manage a situation that could change unpredictably before the right rehabilitation unit is available, and how to ensure that the local authority and others responsible for P’s care keep up the momentum in finding the right treatment for her. Understanding the Mental Capacity Act 2005 is not just about analysing black letter law and statutes and discussing it in the abstract. I’ve learnt that the Court of Protection’s role is also about managing the concrete particular details of a particular P in the specific conditions of her life and in the context of over-stretched health and social care services.” (Lucy Williams, aspiring solicitor)
Through our social media presence and blogging, we’ve created a much broader awareness of the Court of Protection and what it does: our hashtag is #NotSecretCourt. The vast majority of people don’t (and won’t) attend hearings: they learn of the court’s work only through published judgments and media reports.
Few members of the public ever read published judgments – and they are in any case post-hoc polished explanations and accounts for the judgment, which can obscure the messy process by which the judgment was arrived at – the dead ends explored, the arguments from counsel that didn’t work, the questioning that went nowhere, the thinking-aloud reflections of the judge pondering the case. It is precisely seeing how the decision is arrived at, and the real-life constraints within which the court must work, that is so illuminating. It is of course crucial for open justice that judgments are published – we wish more were! – but they are no substitute for observing a hearing.
Journalists are supposed to be the ‘eyes and ears of the public’ – but comparing media reports of the cases we observe with our blogs about the same cases, we are struck by the huge differences. Compare for example the media reports of the case of the woman with agoraphobia ordered by the court to give birth in hospital with the blogs from our contributors, who included a woman with agoraphobia, a medical ethicist, and some midwives. A journalist cannot be expected to see or hear court proceedings (or read a judgment) from the perspective of a midwife, a consultant obstetrician, a doula or a person with agoraphobia – each of whom brings her or his own unique personal and professional experience to bear, and each of whom can speak authoritatively to a specialist constituency, able to engage with the issues with expertise and sophistication.
We believe that open justice is vital in the Court of Protection not least because of the human rights issues involved. Over the course of the year we’ve covered, for example:
Covid-related issues: Is it in P’s best interests to be vaccinated against covid (yes, here; no, here)? Are a care home’s rules about visiting arrangements during the pandemic a violation of P’s human right to family life (here and here)?
Life-sustaining treatment: Should P continue to receive clinically assisted nutrition and hydration? (yes, here; no, here) Should P have their leg amputated against their wishes when not amputating will mean that they die? (yes, here; no, here)
Choices in childbirth: Should women who don’t want to give birth in hospital, or be induced, or have caesareans, be compelled to do so, by force if necessary? (See one lawyer’s take on this here.) Is it in the best interests of a learning disabled woman (wishes unascertainable) to have a caesarean? (here)
Engaging in sex: Does a woman with dementia have the mental capacity to engage in intimate relations with a man in her care home? (here) Can P can be provided with support to access a sex worker? (here) And we’ll shortly cover a case that originated in the COP and is soon to be heard in the Supreme Court, live streamed): does capacity for sex include the understanding that the other person must have the capacity to consent to sex, and does in fact consent, before and throughout the sexual activity?
Deprivation of Liberty: Does P have the mental capacity to decide where he lives or can he be deprived of his liberty, against his wishes, in his own best interests? (here) If P is deemed not to have capacity and says he’s “incarcerated against my will” and wants to return home, how long and on what basis can the court keep him in what he calls a “prison”? (here and a similar case here) If P isn’t able to express her wishes, but a family member who loves her wants to care for P at home, on what grounds can the state keep her in an institution? (here)
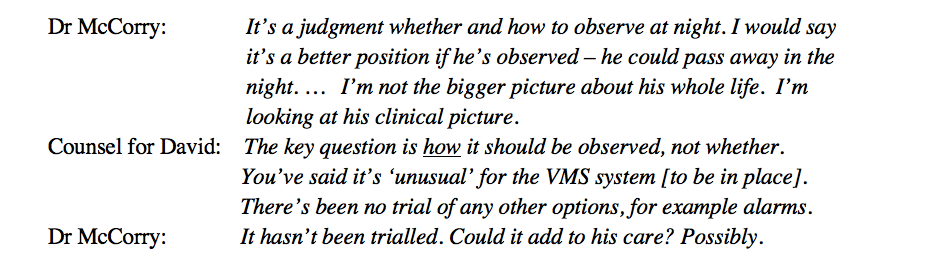
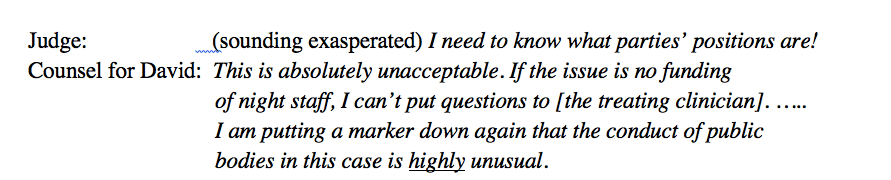
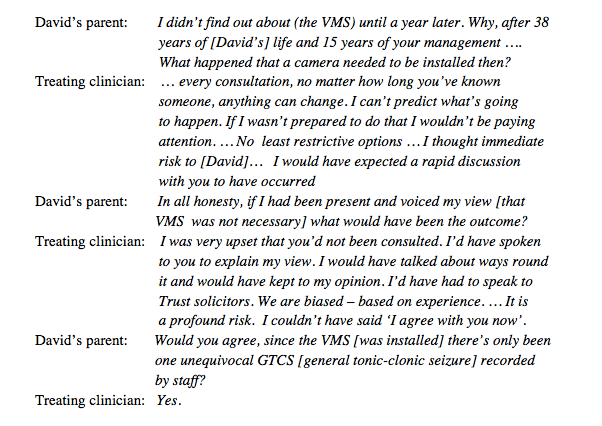
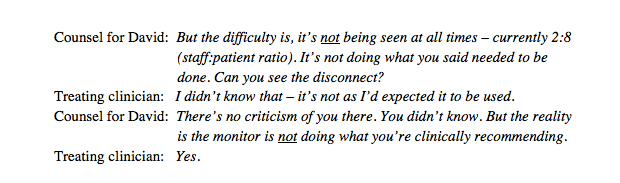
When can the state compel P to take medication that he’s refused by hiding it in his tea? (here); or restrain P to ensure he or she has the surgery they’re resisting? (here and here); or invade P’s privacy by keeping a video-monitoring device on him day and night? (here)
In a democratic society, these sorts of decisions for vulnerable and disabled people should rarely be made behind closed doors.
The future
We’re extremely pleased with what we’ve achieved so far in such a short space of time. We’re also exhausted! Happy, exhilarated and excited, yes. But also exhausted.
We’re still unfunded: we paid out of our own pockets for the (modest) costs of website hosting and logo-design. We’ve done all the work of building and maintaining the website ourselves. Five days a week, it’s still one of us who scours the listings for the Royal Courts of Justice, First Avenue House and the regional courts – correcting the errors, formatting them consistently, tweeting them to the three thousand people who follow us on Twitter, and selecting the most ‘interesting’ or ‘accessible’ for ‘Featured Hearings’. We’re not looking for funding (we value our independence) but it does mean there’s only so much we can do. We’re thrilled that Kirsty Stuart and Claire Martin have joined us.
We didn’t really plan the achievements of our first year – we reacted to circumstances, pushed on various doors to see which ones opened, took the opportunities that presented themselves, and pursued the issues we cared about most. I imagine next year will be much the same, but with more of us actively involved in the core group.
We’re celebrating how much we’ve achieved and looking forward to the challenges of the future – which will of course include how to manage open justice when the courtroom buildings are finally fully open and hearings move back, in whole or in part, into physical rather than virtual spaces. We’re hoping the courts will work with us to continue to facilitate open justice after the pandemic as they have done during it.
Happy First Birthday to Us!
Celia Kitzinger and Gill Loomes-Quinn are the co-founders and co-directors of the Open Justice Court of Protection Project. Celia tweets as @kitzingercelia and Gill as @GillLoomesQuinn
Photo by Stephen Wheeler on Unsplash