By Celia Kitzinger, Claire Martin and Daniel Clark, 14 January 2022
An autistic learning-disabled man in his 30s has not been vaccinated against coronavirus (COVID-19) because his sister does not agree that vaccination is in his best interests.
The Clinical Commissioning Group responsible for his care has made an application to court for an order that vaccination is in his best interests and should be administered as soon as possible. The application is supported by the Official Solicitor (on behalf of the protected party) and by his father. It is opposed by his sister.
This was the issue at the heart of the all-day hearing we observed before Deputy Circuit Judge Rogers in Nottingham (Case no.13816452 on 29th November 2021).
Introduction by Celia Kitzinger
The backdrop to this hearing is a global pandemic with profound economic, social and political impacts.
We’ve seen draconian measures to contain the virus – lockdowns severely limiting freedom of movement, compulsory mask-wearing, restrictions on contact with loved ones – and a desperately overstretched health service.
The political motivations behind lockdown measures, their underlying legality, and their impact on parliamentary democracy have all been challenged (e.g. “Was lockdown lawful?” ”Is lockdown 2 lawful”) and have led to huge protests internationally.
Both the evidence base for masks, and questions about the safety and efficacy of a mass vaccination programme, have been at the centre of public protests and demonstrations, some directly targeting vaccine clinics.
Fears about government infringement of fundamental freedoms via compulsory vaccinations and vaccine passports has also fuelled public unrest internationally. Critics point to the weaponizing of fear to coerce population-wide vaccination and to the use of coercive psychological power to pit those who comply with mask-wearing against those who do not, and the vaccinated against the unvaccinated. “Propaganda and the manipulation of the masses has been a key tenet in totalitarian regimes”, says one critic, pointing to the “segregation and persecution” now meted out to the unvaccinated. Others make comparisons with Nazi Germany and claim we are headed at break-neck speed into a “global pseudo-medicalized police state” fuelled by the “demonization of the unvaxxed”.
In the UK, public trust in the government rose at the beginning of the lockdown imposed in March 2020 but has declined ever since, attributed to a series of government failings: its numerous last-minute U-turns, granting contracts for PPE to personal contacts who’ve failed to deliver, and its own ministers and their advisers breaking the rules.
The pandemic, and measures attempting to contain it, have exposed and exacerbated social divisions and inequalities. “The necessary restrictions of freedom during an epidemic may be strategically exploited by governments to reinforce power”, say academics who’ve studied plagues of the past (the Black Death, the Spanish flu, the great cholera outbreak in Paris) – all of which, they say, were “incubators of social unrest”.
The courts are inescapably enmeshed in the socio-political issues of the day – and this includes the politics of COVID-19.
There are statutory prohibitions on salaried judges undertaking any kind of political activity and detailed guidance for judges that they should “avoid any appearance of political ties”. Judges are warned of the risks of taking part publicly in “political or controversial discussion”, “public debate”, “public protests and demonstrations” or other conduct that might risk undermining public perception of the impartiality of the judiciary. Impartiality means that the judge’s personal, political and ethical views are subordinated to the law which he or she must administer (Guide to Judicial Conduct).
But impartial administration of the law is always already to take a side – and it’s the “wrong” side for those who oppose the law, challenge government rules and policies, and want to change them. This applies to those who dissent from mainstream views about the vaccine as to any other dissenters, and it applies across a wide range of issues addressed by the court.
It’s clear, for example, that decisions about sexual behaviour at the heart of several recent Court of Protection cases are likewise inescapably enmeshed in wider social, political, and ethical debate: the hearing we blogged as Is it lawful for C’s carers to support him in accessing a sex worker? evoked wide-ranging public discussion about the oppression of women represented by the sex industry, and prostitution as a form of modern slavery.
The remit of the court and existing case law.
Despite an enduring myth that “next of kin” are decision-makers for their incapacitated loved ones, it is rarely the case (in England and Wales) that family members can lawfully make serious medical treatment decisions, including vaccination decisions, on behalf of other adults.
In SD v RB Kensington and Chelsea [2021] EWCOP 14, Hayden J held that: “…strongly held views by well-meaning and concerned family members should be taken into account but never permitted to prevail nor allowed to create avoidable delay. To do so would be to expose the vulnerable to the levels of risk I have identified, in the face of what remains an insidious and highly dangerous pandemic virus” (§ 26)
Decisions about vaccination for adults unable to consent to it are usually made in their best interest by the person with overall responsibility for the person’s health care. Very often this means (for people living in care homes) their GP – who should consult with “anyone engaged in caring for the person or interested in his welfare” (4(7)(b) Mental Capacity Act 2005).
When there is disagreement between professionals, between family members, or between professionals and family members about whether or not vaccination is in the protected party’s best interests (and where this cannot be resolved after second opinions, mediation attempts etc), then the matter should be quickly referred to the Court of Protection.
For the Court of Protection, the ’facts’ about COVID-19 and vaccination are pre-determined as in line with government policy, the NHS England COVID-19 Vaccination Programme, the Joint Committee on Vaccination and Immunisation (JCVI) and mainstream scientific research.
In SD v RB Kensington and Chelsea [2021] EWCOP 14, Hayden J held that: “… it is not the function of the Court of Protection to arbitrate medical controversy or to provide a forum for ventilating speculative theories. My task is to evaluate V’s situation in light of the authorised, peer-reviewed research and public health guidelines, and to set those in the context of the wider picture of V’s best interests.“(§ 31)
This means that little weight is given to “alternative” perspectives from family members (or others) who oppose vaccination of a protected party on the basis of challenges to the “authorised, peer-reviewed research and public health guidelines”. Non-mainstream medical viewpoints from family members (or – indeed – from professionals) about COVID-19 are, according to this stipulation, simply disregarded by the Court.
Reliance on mainstream science means that, in practice, the Court overwhelmingly finds in favour of vaccination being in the protected party’s best interests, as illustrated by these extracts from judgments.
In stark terms the balance Mrs E, aged 80, must confront is between a real risk to her life and the unidentified possibility of an adverse reaction to the virus. This risk matrix is not, to my mind, a delicately balanced one. It does not involve weighing a small risk against a very serious consequence. On the contrary, there is for Mrs E and many in her circumstances a real and significant risk to her health and safety were she not to have the vaccine administered to her. […] By virtue of her vulnerabilities, the prospects for her if she contracts the virus are not propitious; it is a risk of death, and it is required to be confronted as such. The vaccination reduces that risk dramatically and I have no hesitation in concluding that it is in her best interests to receive it. (Hayden J , §17 & 19, E v LB Hammersmith and Fulham [2021] EWCOP 7,
“I find that the risk to V’s life and health, if she were not to have the vaccine, would be unacceptably high and that it is in her best interests to receive it. In cases such as this, there is a strong draw towards vaccination as likely to be in the best interests of a protected party (P).” (Hayden J, §33 in SD v RB Kensington and Chelsea [2021] EWCOP 14)
This mainstream science must, however, be considered in the wider context of the protected party’s own past and present values, wishes, feelings and beliefs (as mandated by s. 4(6) Mental Capacity Act 2005).
P’s values, wishes, feelings and beliefs
As Hayden J said (in the context of a judgment approving vaccination, counter to the position of the family,[I] it cannot be presumed that vaccination is inevitably in a protected party’s best interests:
What it is important to emphasise here, as in so many areas of the work of the Court of Protection, is that respect for and promotion of P’s autonomy and an objective evaluation of P’s best interests will most effectively inform the ultimate decision. It is P’s voice that requires to be heard and which should never be conflated or confused with the voices of others, including family members however unimpeachable their motivations or however eloquently their own objections are advanced.” (Hayden J, §33 in SD v RB Kensington and Chelsea [2021] EWCOP 14)
And in another judgment, this time finding that vaccination was not in the protected party’s best interests, Hayden J said: “A determination of ‘best interests’ in this context … [is] not to be confined to the epidemiological; it requires evaluating welfare in the broader sense” (§36, Re SS [2021] EWCOP 31)
The case in which Hayden J made this comment was one in which the protected party herself (as opposed to her family members) held strong views about vaccination: “It seems unlikely she would have wanted [vaccination] whilst capacitous and certainly does not want [vaccination] at this point”. (§ 32 Re SS [2021] EWCOP 31.).
Cases in which both the past and present wishes of the protected party are not to be vaccinated are fairly rare in my experience. This case was specifically assigned to a Tier 3 judge (the highest level in the Court of Protection) because it represented “an opportunity to evaluate strongly and consistently expressed views by P relating to vaccination and the weight they should be given, in the broader landscape of the insidious risk arising from the Covid-19 public health crisis” (§ 35).
The case concerned an 86-year-old woman (SS) with dementia living in a care home, who was refusing COVID-19 vaccination. It was accepted by all parties that she lacked capacity to do so.
Her refusal of vaccination was in the context of increasing resistance to medical interventions of any kind. The judgment records that SS had kept a newspaper cutting of an article she read as arguing that medicine “did more harm than good”. She would “brandish [the newspaper article] with characteristic forcefulness, at anybody who sought to afford her medical care of any kind” and has been “almost entirely non-compliant with any attempted intervention”: she has refused blood pressure medication, and application of cream for a rash on her leg.
Specifically in relation to vaccination, her medical records going back to 1997 show no record of SS receiving any vaccination of any kind at all.
”Even more strikingly there is an unambiguous note that SS declined both seasonal influenza and pneumococcal vaccines when offered them by the surgery. The first of these refusals is recorded in 2002 with entries identified in 2010, 2012 and 2014. Thus, there is a clear and consistent pattern of behaviour which predates SS’s diagnosis of dementia by a significant period.” (§20 Re SS [2021] EWCOP 31)
In court, Hayden J explained to the staff giving evidence that he was “trying to balance risk of death against trying to protect her dignity, autonomy, who she is, her pride” (quoted in blog post). In the end he decided: “though much of [SS’s] cognitive function may have gone, her autonomy – and her own sense of it – not merely continues but flourishes, and she guards it carefully. Ultimately in my judgment, it is that which requires to be respected and is ultimately determinative of this issue” (quoted in blog post).
In the published judgment, Hayden J concluded:
“…. there can be no doubt that SS lacks the capacity to take a decision on the question of vaccination. Nobody has sought to argue to the contrary. The issue for the court therefore is one of determining what is in SS’s best interests. Having regard to the available evidence I consider that there is substantial material from which to conclude that SS if capacitous would most likely have declined the vaccination. …. it must be borne in mind that even though a capacity to weigh and balance the decision in focus has long disappeared, SS has nonetheless consistently and volubly opposed the vaccination. SS’s reality is undoubtedly delusional, but that does not stop it being her reality. This has to be both recognised and respected.” (§25 Re SS [2021] EWCOP 31)
Each case, then, has to be assessed on an individual basis, and it cannot be presumed that simply because vaccination is in a person’s medical interests according mainstream scientific evidence, that it is therefore in their best interests overall.
If the evidence is that a protected party would have wanted to refuse vaccination (or is in fact refusing it, albeit non-capacitously) then that would need to be taken into account as part of best interests decision-making, and could (as in Re SS) lead to a best interests decision not to vaccinate.
The difficulty in many cases (including the one reported here ) is that P’s own wishes may not be, to use the language of the Act, “reasonably ascertainable” – and in cases like the one we’re focusing on in this blog post, which concerns a person with a learning disability, the person may never have had the capacity to express their own values, wishes, feelings or beliefs about vaccination.
Where – as here – the person at the centre of the case has not been able to communicate either past or present views about vaccination, it is difficult to see – as we will show – how any argument from family members challenging mainstream scientific research about the safety or efficacy of the vaccine could influence the court’s best interests decision-making.
The hearing on 29th November 2021
This hearing concerned whether it is in the best interests of a man (P) living with what was described as “severe intellectual disabilities and severe Autism Spectrum Disorder” to receive COVID-19 vaccinations.
There was no dispute that P lacks capacity to make his own decision about COVID vaccination, and hence that a ‘best interests’ decision was required.
He doesn’t understand the relevant information about COVID-19 and cannot weigh it up in coming to a decision. Attempts to help him to understand and express a view have failed: asked what coronavirus is, he pointed to the symbol for sweets. When asked what happens if you get the virus, he twice pointed to the symbol for a holiday.
It had proved impossible to elicit P’s wishes and feelings on the matter – beyond the obvious observation that he dislikes having needles put in his arm.
At a meeting on 1st March 2021 (so 9 months before this hearing), it had been agreed by the care home staff looking after him, his GP, and his father that vaccination was in his best interests.
His sister does not agree, which is why the case came to court.
The application (for an order that vaccination is in P’s best interests) was made by NHS Nottingham and Nottinghamshire Clinical Commissioning Group (“the CCG”), represented by Ben Tankel of 39 Essex Chambers.
The man at the centre of the case, P, was represented via the Official Solicitor by Victoria Butler-Cole QC, also of 39 Essex Chambers.
P’s father played a “low key” role (the judge’s term) as a litigant in person. (There are no quotes from him in this blog because when offered the opportunity to contribute in his role as a party in court he usually declined to do so, beyond simply asserting his support for his son to be vaccinated.)
And P’s sister was represented by Geoff Peter of Wingrove Law – a lawyer we’ve not previously seen in the Court of Protection, and a specialist in the law relating to new build properties. (We understand that P’s mother supports the position of P’s sister but that she was ill and unable to attend court.)
The hearing opened with a discussion of the admissibility of evidence from a retired GP whose advice P’s sister had sought and then forwarded to the court (see our previous blog post, and further discussion of his role by Daniel Clark below). Although this GP, Dr Jon Rogers, played no formal role in the case, there had been (as the judge put it) an attempt by the sister to “leak information” from him into the case, and so his role is of interest to us.
Counsel for the applicant CCG summarised their reasons for believing that vaccination is in P’s best interests and went on to describe the other parties’ positions as follows:
“His sister objects to giving of COVID vaccination, full stop. The main substance of her objection is what I’ll call, in a non-derogatory way, an ‘anti-vax’ stance. The Official Solicitor is not objecting on clinical grounds but did have room for pause or hesitation over the issue of restraint, because by Friday we hadn’t set out what that would entail. We now have done so and she agrees it is limited, proportionate, minimal and lawful. And P’s father supports the giving of the vaccine.”
He said there was a question “about the extent to which the court should get involved with the generic questions about the merits of the COVID vaccination as such”, and drew attention to Hayden J’s statement that it is not the function of the Court of Protection to arbitrate on medical controversies. In any case in which “mainstream scientific evidence” is set against the views of “anti-vaxxers”, the court – said counsel – “is going to prefer the former”.
Victoria Butler Cole QC (for P via the Official Solicitor) took the same position. P’s sister, she said, had “submitted various Excel spread sheets which purport to set out scientific opinion …. We have no objection to the court looking at this, but it’s not going to take the court very far. The court cannot prefer an Excel spreadsheet analysis from a non-expert over advice from the government and peer-reviewed articles in scientific journals”.
The judge was clear from the outset that “this is not a forum for a public symposium on the merits and demerits of COVID jabs that go beyond the best interests of this patient” and said “I do not want this to become a soapbox for a broader debate about the rights and wrongs of COVID vaccination”.
The tension that ran throughout this hearing was between “mainstream” views (as represented by government policy, NHS England and JCVI) and the views of P’s sister (and the GP whose opinion she had elicited), which were critical of this mainstream perspective, questioned the dominant narrative about the safety and efficacy of the COVID vaccine and challenged government policy of mass vaccination and other ‘coercive’ measures. On our analysis, it seems that P’s sister set herself against what, for the Court, constituted an overwhelming body of scientific opinion on vaccination.
As the judge stated at the outset, it is not for the Court of Protection to “embark on a broad, academically-wide debate on the merits and demerits of vaccination”.
The case for vaccinating P
The case of the applicant Clinical Commissioning Group (CCG) for vaccinating P was that, like everyone else, he was at risk of contracting COVID-19 – more so since he does not understand the need to observe social distancing measures. The evidence is that people with learning disability are also more likely to become seriously ill and die from COVID-19. There is “very little to weigh in the balance against his receiving it”, said counsel for the applicant, since the restraint to enable vaccination would be minimal and brief.
The Official Solicitor (OS) took effectively the same position, providing research evidence published in the British Medical Journal in June 2021 based on review of 17 million patients showing that people with learning disabilities who test positive for COVID-19 are five times more likely to be admitted to hospital and eight times more likely to die. A long period of hospitalisation would be difficult for P, she said, and any physical restraint required for vaccination would be “very fleeting”.
For both the applicant CCG and for the OS, then, the risk/benefit analysis was unambiguously in favour of vaccinating P.
The case against vaccinating P: A “veiled” and “tactical” approach from P’s sister
The sister (we’re referring to her as CT) gave a wide range of reasons as to why P should not receive COVID-19 vaccinations.
The reasons she’d provided in advance, in documentation to the court (which we haven’t seen), were summarised or read out at different points in the hearing by counsel for the CCG and counsel for the OS and by the judge.
We understand that they relate to concerns about the clinical risks of the vaccine generally, and about the ethics of it being administered to a person like P without his consent (which of course he is unable to give, or to withhold).
We have not seen CT’s witness statement, but according to counsel for the CCG her main focus in that document is that:
“… contrary to the established scientific consensus and all applicable public health guidance, she believes the COVID-19 vaccine is harmful. Opposition to vaccination appears to be the lifelong stance of P’s sister and mother: P has never received a flu vaccine and only received a few vaccinations when he was born”[2]. (Counsel for the CCG)
The judge described CT’s witness statement as “an argumentative statement which goes from first principles to the efficacy of the vaccine itself”. The documents CT had submitted, and those submitted by counsel on her behalf were, he said, “of a wide-ranging and general nature” concerning the safety and efficacy of COVID vaccination.
From what was said by counsel for the Official Solicitor, it seems that CT also suggested that people who are vaccinated are more likely to die from COVID than those who are not. Counsel described this as “based on a misunderstanding of risk” and relied on the Office of National Statistics for evidence that the rate of death from COVID among the unvaccinated is 32 times higher than among the vaccinated.
Counsel for the CCG addressed another concern apparently raised by CT in advance of the hearing: the problem of administering the vaccine to someone unable to consent to receive it. That, of course, is what the Court of Protection process is for: it supplies the consent that those lacking capacity are unable to provide for themselves. “To hold otherwise would mean that the most vulnerable members of society would be deprived of all medical treatment, which would be a far worse ethical outcome.”
As observers, we have access to these arguments from CT only via the rebuttals from counsel for the other parties. These were not the key arguments she presented in her oral evidence to the court.
In court, CT raised concerns about not having been given sufficient information by the treating team about the risks and benefits of the vaccine for her brother, and said that in the absence of that information she did not believe that she (or, by extension, the court) was in a position to make a decision in his best interests.
She also asked for further investigations to be undertaken. These included a blood test to see whether her brother already had natural immunity (which might have been achieved from an earlier COVID outbreak in his care home), an ECG, and research into possible counter-indications for vaccination due to drug interactions. If the court were to order that vaccination was in P’s best interests, she asked for this to be delayed until after Christmas, so that he could enjoy the festive season without side-effects.
The judge found a “rather stark contrast” between the witness statement CT had submitted to the court, which he described as embodying “an inherent opposition to the vaccine and to the vaccination programme”, and the position she took in court today in which “she was careful to give credence to vaccination and the dangers of COVID” and to “follow what is obviously the court’s task of looking at what is in P’s best interests”.
Commenting on this “contrast” (between the documents submitted and the oral evidence), the judge said: “I regret to say this. I wish in no way to be unpleasant, but I am quite satisfied that this was a strategic or tactical approach that was taken.”
He added: “I am satisfied that she is, in principle, in opposition to COVID vaccination (and maybe vaccination in general)”.
The judge suggested that CT’s oral submissions in court served “substantially to cloud the issue” and that she had made “a veiled submission in the hope of deflecting consideration away from the substance of the case”. This is “a dangerous approach and clouds the issue”.
In the rest of this blog post, the three observers – (1) Daniel Clark, (2) Claire Martin and (3) Celia Kitzinger – explore the way in which the politics of COVID-19 vaccination played out in court, both via the sister’s attempts to introduce evidence from a campaigner who’s been explicit in taking a position against government policy on COVID-19 vaccination, lockdown, and laws about face-coverings, and via the sister’s own testimony in court, in relation to opinions she’s stated out-of-court. Finally in section (4), I draw on my experience of watching COVID vaccination hearings more broadly to make some suggestions for how people can put in place protection for themselves to ensure that they won’t be vaccinated against their wishes after loss of capacity, and how best to promote the wishes and beliefs of those who have, or may be about to, already lost capacity to make this decision for themselves.
1. Dr Rogers and politics in court by Daniel Clark
This was the first time I’d observed a hearing in the Court of Protection, and knowing in advance (from the listing) that it was about COVID vaccination, I expected it to stimulate reflection on my experiences in social care, as a paid carer.
As it turned out, it was my interest in political theory (having just completed an MA) that was most stimulated.
First, briefly, in terms of social care. In this case, there had been (some months earlier) a COVID-19 outbreak in P’s care-home. Whilst it transpired that P did not contract COVID-19, the deputy manager was very clear that every resident was affected “one way or another”. This did strike a chord with me. COVID-19 is not just a virus that has the potential to cause serious illness. Living in a care home brings a unique sort of social isolation for all residents, with family visits potentially cancelled depending on the scale of the outbreak. It also brings with it an overwhelming atmosphere of panic, both for residents and, I must admit, for staff. It’s hard to ‘switch off’ after your shift when, after a couple of days off, you could be going back to even more people who have tested positive.
These were, however, background thoughts. Instead, I’ve mostly found myself reflecting on the way in which politics and the Court of Protection came together. Before going further, I do want to acknowledge my own epistemic bias – that is to say, the bias I have with regards to the type of knowledge that I identify and categorise as true. I accept the mainstream science regarding the COVID vaccine, and I believe that lockdowns saved many thousands more people from dying. I emphasise this so that all of my cards, so to speak, are on the table.
Dr Jon Rogers
The hearing got off to a rather confusing start (at least for me) with a discussion about “the unauthorised disclosure of court material to Dr Jon Rogers” (described as “a retired GP”) and whether an email from him could be used as evidence.
The judge ruled the evidence inadmissible because it had been improperly obtained (P’s sister had breached a court injunction by sending confidential court documents to Dr Rogers) and because the Court of Protection Rules Part 15 procedures had been breached in a number of other ways (as described in an earlier blog).
Dr Jon Roger had been subsequently revealed (after the Official Solicitor, on receipt of his letter, had requested his CV) to be one of the directors of the UK Medical Freedom Alliance (UKMFA), one of whose objectives is to “provide information and resources to aid people who wish to challenge mandated Covid-19 testing, interventions or Covid-19 vaccines, and any resulting restrictions or penalties imposed on them”.
The involvement of Dr Rogers was raised again later in the hearing, when P’s sister (CT) was cross-examined by Victoria Butler-Cole QC. “You showed Dr Rogers a draft of your witness statement and got his comments on it before you filed it with the court”, she said. CT confirmed that was so.
Although Dr Rogers is a “retired GP”, the GMC ‘temporarily restored’ him to the register “as part of the UK government’s response to the coronavirus (COVID-19) pandemic.” It is somewhat ironic, then, that having been re-registered for this reason, he opposes the government’s response to the pandemic[3].
Both as a “retired GP” and with reference to his re-registration by the GMC, Dr Rogers has used his medical credentials to spread what has been described as “disinformation, conspiracy theories and pseudoscience” about the pandemic itself, and the vaccine, especially via the UKMFA (see this tweet thread for commentary).
Dr Rogers is very publicly opposed to a great deal of government policy in relation to COVID-19. He has signed a number of public letters (such as this one) raising concerns about COVID vaccination, including what is said to be the government’s exaggeration of the nature of the threat from COVID, its inappropriate and unethical use of behavioural science to generate fear, and the misunderstanding concerning asymptomatic spread and its use to promote public compliance with restrictions. He signed a letter to the Education Secretary arguing for #NoMasksInClass and he’s a signatory showing support for the British Ivermectin Recommendation Development Group (BIRD).
The UKMFA provides links to downloadable template letters for people to use across a range of situations: for example, if you have been refused access to any type of medical treatment without taking a COVID-19 test; to help parents withdraw their consent to any offer of COVID-19 vaccines for their child at school, and to challenge any claim that their child has Gillick Competence to consent themselves; and a letter for care home staff to use to decline ‘mandatory’ vaccines.
The videos Dr Rogers has posted on Facebook express his passionate resistance to government policies on lockdown, mask-wearing, and vaccination – in large part due to his commitment to “freedom” in the form of individual autonomy and the right to choose.
He commented recently on a survey which he found “reassuring” for showing that “the majority believe that protecting the right to choose is more important to people than controlling Covid” (23rd November 2021, Facebook).
At a “Freedom Rally” (College Green Bristol, 15th May 2021, Facebook Video 98) he was scathing about mask-wearing (which does not work, he says, to prevent COVID transmission) as a form of “virtue-signalling”. His speech comes to a rousing conclusion, as he pumps his arm up and down over his head and leads the chant, followed by cheers, whistles, and applause from the crowd.
“We are now in a situation where we can carry on living in fear, living in this dystopian, disproportionate world or we can stand up and say: I am free! You are free! We. Are. Free!
We are free! We are free! We are free! We are free! We are free! We are FREE!”
At an event called “Glastonbury Freedom Festival”, Dr Rogers referred to government policy as “a scam”, to roars of approval from the crowd. He said of COVID: “Children don’t get it. This is not a disease of young people. This is a disease of the elderly and frail” (at around 4 mins, Facebook Video 107).
In the same talk, he says: “the vaccine is not safe, and frankly it’s not even very effective” (at about 19:40, Facebook Video 107) stating that “most of the people in hospitals with COVID have had two jabs”.
Freedom from coercion is again at the core of his message:
“This is a little virus that I’m not that frightened of. I’m frighted of the totalitarian regime that seems to be coming on the back of it. I’m frightened of the vaccine passports. I’m frightened of the identity cards, I’m frightened of all those things, but I’m not frightened of COVID. I personally have a number of co-morbidities. I’m 66. But I reckon I’ve got a 1% chance of dying if I catch it. That’s not enough to make me want to rush out and get a vaccine.”
Last year, as part of my MA in Political Theory, I spent a great deal of time reading (and writing about) Hannah Arendt. In 1967, she published an article titled Truth and Politics. Here she wrote that “no opinion is self-evident. In matters of opinion…our thinking is truly discursive…until it finally ascends from these particularities to some impartial generality”. Facts, on the other hand, are in her words, “irritating…for they have no conclusive reason whatever for being what they are”. What connects fact and opinion for Arendt is that neither of them is self-evident, “and this may be among the reasons that opinion-holders find it relatively easy to discredit factual truth as just another opinion”. Thus, the factual truth that the COVID vaccines are mostly beneficial and not harmful can be discredited as “just another opinion”.
I have raised this because Arendt’s essay clearly sets out that opinion is political but truth is strictly non-political: in fact, she suggests, it may even be “anti-political”. Therefore, when something that purports to be fact is presented in an overtly political way, we have the glimmer of an idea that what we’re being told is actually an opinion. Dr Rogers speaks quite clearly about being ‘“frightened of the totalitarian regime that seems to be coming” as if it is a fact. In the interests of transparency, I would like to be very clear that I have grave concerns about the policy direction of this government. But to describe our government as on the cusp of totalitarianism as a result of extraordinary measures taken in an extraordinary situation is not a factual description: it’s a political opinion.
I do suspect that concerns about the vaccine have been conflated with concerns about the handling of the COVID-19 pandemic. In a review of a book about ‘Anti-Vaxxers’, Julie Leask tells us that vaccine concern “has always been a proxy for wider fears about social control”. In the last 21 months, we’ve had what could be described as “social control”, in the forms of lockdowns, mandatory mask wearing, and limitations on social contact and travel. And then a new vaccine.
It is when the distinction between fact and opinion is blurred that we are in potentially hazardous waters. CT’s view of P’s best interests was couched in claims of being factual when they amount to opinion (her views about vaccination, discussed in detail by Celia Kitzinger below, are simply not reflective of commonly accepted scientific facts). When opinion masquerades as just another version of truth, the waters become muddied, and (as in this case) decisions are delayed. It is presumably because the care home gave weight to CT’s opinions about what was best for P – opinions that seem to have drawn on the kinds of campaigns advanced by Dr Rogers (among others quoted in the Introduction to this blog post) – that P did not receive a vaccine for almost 9 months.
As a result of anti-vaccination campaigns, at least to the extent that CT is part of them, P has been unvaccinated and at risk of COVID, despite the fact that (as his counsel established from the care home deputy manager) he has been “out and about in the community”, unable to understand social distancing or to wear a mask. This would have significantly raised his risk of contracting COVID-19.
What remains, therefore, is a situation in which the politics of the pandemic (including the vaccine rollout) have intruded into the assessment of the best interests of P on the ground. This is not to say that the beliefs held by CT are not genuinely held, the result of years of her own research. However, what cannot be avoided is the fact that her beliefs, in tandem with her political opinions about vaccination, delayed a best interests decision for almost 9 months.
Of course, I do not believe that CT genuinely wanted to put her brother at risk – her love for him seemed quite profound. A possible interpretation of CT’s resistance to her brother having vaccines is that she believes that her priority is to protect him from human-made harm, and that it is more important to protect him from this than a ‘natural’ harm (of infection). She was doing the best she could in accordance with her beliefs, desperately trying to keep her brother safe against the weight of the NHS and the law. Speculation aside, what remains is that CT’s cost-benefit analysis misidentified the greatest risk in this case i.e. the risk of COVID rather than the risk of vaccination.
As Dr Marcus Gillespie writes, a “common source of error in deciding who is an expert is to mistakenly conclude that because someone is an expert in one field, they are an expert in another” (emphasis in original). He uses the example of Senator Rand Paul who, when people know he is a doctor, is usually assumed to know ‘as much about Covid-19 as the experts he is challenging’. However, Rand Paul has a medical degree in ophthalmology, meaning that ‘he isn’t an expert in the relevant field’ (emphasis in original).
Despite the fact that GPs actually do make judgments all the time about best interests for people with complex long term needs in a community residential setting, Dr Rogers is not an “expert” in the relevant fields of immunology, virology, epidemiology.
The judge found, ultimately, that it was in P’s best interests to receive both shots of the COVID vaccine, the booster, and any subsequent booster deemed necessary. I was relieved by that.
This considered judgment emphasised to me that fact (not political opinion) is at the heart of the decision-making process of the Court of Protection.
2. Clouding the issues: The blemish game by Claire Martin
Many thoughts were going through my mind observing this hearing.
Why was this case only reaching the court now – 11 months after the introduction of COVID vaccination in the UK?
What is the Court of Protection’s position on debating the whys and wherefores of COVID-19 vaccination?
What do care homes and treating medical teams need to understand in order to navigate decisions about, and (if necessary) expedite, medical treatments for people who lack capacity, when there is family disagreement about those treatments?
How can the Court navigate arguments against action X when those arguments do not seem to be in ‘good faith’?
I found this hearing an education. P is the only resident in his home (of eight people) who has not received the COVID-19 vaccination. He doesn’t like needles (or indeed any medical intervention) and his sister was against the vaccination for him, she said, because she was concerned about the impact on him emotionally and because the clinical risks of vaccination for him as an individual (as opposed to the clinical risks to him of COVID), she asserted, had not been fully investigated.
Witnesses at the hearing
The hearing opened with an initial discussion about admissibility of evidence from retired GP Dr Jon Rogers (previously blogged elsewhere) and then opening submissions (as described earlier). This was followed by witness evidence from the Deputy Manager of the care home.
Deputy manager of the care home
Counsel for the CCG, Benjamin Tankel, asked her how long she had known P (12 years) and how often she sees him (every day when at work).
We learned that P is generally an anxious person and is prescribed Lorazepam for this by a psychiatrist. Anymedical procedure causes him anxiety, and restraint, in the form of holding his arms for “no longer than two or three minutes” is sometimes necessary.
The deputy manager explained that restraint is ‘potentially’ necessary for medical procedures and the home has ‘a lot of plans in place’ for that eventuality and they ‘try to avoid it, but it is a possibility’. Notably, P has PCR tests every twenty-eight days and does not resist or experience distress from this.
Counsel: Does he form a negative view of the people restraining him?
Deputy Manager: No, he doesn’t actually.
Cross-examination by Geoff Peter (for P’s sister) raised the question of how long P remains distressed after a medical procedure (such as a blood test): “it depends … usually around 1-2 hours”.
It transpired that the care home had a COVID-19 outbreak last year and all residents, except for P, contracted the virus.
Exploring P’s understanding of, and response to, injections, the deputy manager clearly described P’s visceral response (‘Yes he understands what a needle is. He knows enough to not want a needle in his arm’) – as distinct from an understanding of what the injection is for and a considered decision to refuse. Victoria Butler-Cole QC further explored this line of questioning in her cross-examination.
Counsel: Are there any medical treatment decisions where he’s been assessed as having capacity to make decisions for himself?
Deputy Manager: No.
Counsel: Does he understand what Covid is?
Deputy Manager: No
Counsel: Can he socially distance?
Deputy Manager: No.
Counsel: Can he wear a facemask?
Deputy Manager: No. He would not wear a face mask under any circumstances.
Counsel: He’s going out and about in the community though, isn’t he?
Deputy Manager: Yes.
Counsel: Can he self-isolate, or manage periods of isolation?
Deputy Manager: No. He’s not able to do that due to his behaviours.
Counsel: Would he find it difficult to be admitted to hospital?
Deputy Manager: Oh yes. Very, very difficult.
The deputy manager also explained the care plan for P should a direction be made to give him the COVID-19 vaccination: they would prepare the vaccination out of sight, P would be distracted by watching TV or doing something he enjoys, then he vaccinator (a stranger to P) would enter, P’s arms would be held by carers for a couple of seconds and the vaccinator would vaccinate him swiftly and then leave the room
P’s sister (CT)
Mr Peter opened his questioning of P’s sister by saying that there had been a suggestion in the CCG position statement that CT was ‘anti-vaccination’ in principle.
“NO. That is abhorrent. I strongly refute those claims. I am a medical ethicist. I have a Masters in biomedical law. …. As an ethicist I want a risk-benefit analysis. That was denied to me. I felt bullied and victimised. What should have been good clinical practice has been tainted by how vaccination is presented in the press. I feel very much alone in trying to make sure P’s wishes are maintained. … His best interests is not vaccination. This is not about the vaccine – it is purely and simply about the balance for P.”
Notwithstanding the (im)possibility of ascertaining P’s ‘wishes’ in relation to COVID-19 vaccination (it had been agreed by all parties that P lacked capacity to decide about vaccination and those caring for him said they were unable to ascertain his wishes), my understanding of CT’s submission regarding the balance for P (not having seen her position statement) is essentially that her interpretation of the scientific evidence is such that her brother is not at risk of hospitalisation or death from COVID-19 (should he become infected), that he is at higher risk of complications from the vaccination, and, therefore, that it is not in his best interests to be sedated and restrained in order to administer that vaccination.
Counsel for the local authority cross-examined CT:
BT: Do you have any expertise in immunology?
CT: I have many books. I’m not an expert.
BT: Virology?
CT: I read books. I’m not an expert.
BT: Epidemiology?
CT: The same – I have read up on the subject widely but I don’t consider myself an expert.
CT explained that (from her reading) P risked myocarditis or pericarditis from the vaccine and that those risks had not been acknowledged in a balancing exercise. She argued that this, combined with the necessity of restraint to administer an injection, meant the vaccine was not in P’s best interests. She wanted further assessment of those risks for her brother, in the form of an ECG, and she also wanted an antibody test for him to establish any current immunity from COVID-19. Of course, further assessment would entail more medical intervention for P – which would also necessitate restraint (for a blood test for antibodies) and likely sedation too for an ECG.
This didn’t hang together. If one of CT’s key anxieties was to prevent unnecessary medical procedures for P (because he finds them distressing) arguing for more procedures flies in the face of that concern.
It started to feel to me that CT was using a straw man argument and that her anxieties were actually more about the vaccine per se.
This became most apparent when counsel for P via the Official Solicitor asked CT a series of questions.
Did she accept that COVID-19 can result in “serious illness, hospitalisation and death”? CT replied with a question: “for what percentage?”
Counsel said that wasn’t what she was asking and asked the question again. CT said, “not for everybody”.
When pressed whether the risks are there for everyone, she said “no”.
When pressed further as to whether COVID-19 is worse than the vaccine, she said “it depends”.
I felt for CT when she said she felt “bullied and victimised” by medical professionals at the best interests meeting earlier in the year. She said that the minutes of that meeting were not accurate in terms of how the medical professionals engaged with her and her concerns. It is entirely possible that she was dismissed at that meeting, and that the minutes (written by the professionals) were from their perspective only. It must have been a difficult meeting for her. It is also entirely possible that CT’s position in that meeting was lacking in transparency about why she was taking the stance she was. Both parties would therefore be approaching the meeting with suspicion of the other.
It did start to feel as if she was against vaccination in principle. Instead of just stating that, in good faith, CT’s oral argument in court rested upon criticism of the process of medical risk-benefit analysis for P.
As the hearing continued it seemed as if there would not, ever, be enough ‘evidence’ from assessments of P’s medical risks, to satisfy CT that COVID-19 vaccination was in her brother’s best interests.
If an argument is made in good faith (i.e. you state your clear position and argue from there) then this can be addressed and dealt with by others. If an argument is not made in good faith, then, as at this hearing, parties end up talking about things that are not, really, the nub of the issue.
In his judgment, Rogers J said: “I reject the submission that there is insufficiency of information before the court today. This was a veiled submission in the hope of deflecting consideration away from the substance of the case.”
How can and should courts deal with experiences such as this? If, indeed, CT’s position is one of anti-vaccination in principle, then not saying so means that the questions, discussions and evidence in court are predicated on (what are for her, according to her underlying belief) irrelevancies.
Everyone then starts to feel that their time is being wasted.
Reflecting on CT’s account of feeling ‘bullied and victimised’ in the best interests meeting, I am wondering whether she could have felt the same in this court hearing? The Court of Protection takes an inquisitorial position – rather than a combative approach. Nevertheless, as stated earlier, it has to rely on the scientific evidence accepted and adopted in national guidance insofar as medical matters are concerned. CT might not have appreciated the inquisitorial nature of this court.
In this blog post, journalism students make exactly this point about the Court of Protection:
“It wasn’t combative like you see on the TV. Instead there was a very clear statement from the judge that these were civil proceedings and were very different from a criminal case – there was no ‘prosecution’ and it should not be seen as ‘a fight’ – ideas which seemed to be in the head of the patient’s brother, and the judge was keen to challenge this. The judge said the Court of Protection was trying to make a best interests decision which meant people coming together to try to work out what was right for the person at the centre of the case – combining what was known about his clinical condition with what was known about him as an individual.“
I wonder whether, because the COP operates in this way (and not in a combative manner), CT’s approach was misguided. An approach that appears to be in ‘bad faith’ (i.e. not actually a party’s true position) is unusual in the COP, and its effect was to derail the usual etiquette and conventions. CT might not have known this, of course, and her counsel is not a COP barrister, so also might not have been familiar with the conventions. Even if CT and her advocate had been aware of the inquisitorial nature of the court, they would have been at a disadvantage due to the fact that the court accepts the mainstream scientific evidence – but at least they might have chosen the approach of presenting a transparent, good faith, argument. Then all parties would have been advancing their ‘true’ position.
So, CT might well have, again, “felt bullied and victimised” in this hearing. It is possible that she (and anyone who has some scepticism about, or outright opposition to, vaccination) will feel this way in general at present, given the public health narrative and messaging about COVID-19.
Anyone who is already feeling “bullied and victimised” is likely to respond badly to the COP’s (mandated) position in relation to what it recognises as medical evidence.
From a relational perspective (whatever one thinks about vaccines), it might have felt to CT that her ‘bullied’ position was acceptable to the court, at the expense of challenging (what CT might see as) the “bullying and victimising” behaviour of the court/the government/the scientists/the system.
Under these circumstances it would be hard to hold on to an “adult ego state” (see next section) while feeling “bullied and victimised”. If your frame of reference (to a specific issue) is entirely through this lens, a forum where ‘best interests’ are based on a body of information that you fundamentally oppose is not going to seem fair. It might then lead to particular approaches as a way of coping. I explore one potential approach below.
The blemish game
Eric Berne, the founder of transactional analysis, wrote a book called Games People Play. In this book, he describes:
“a series of “mind games” in which people interact through a patterned and predictable series of “transactions” which are superficially plausible (that is, they may appear normal to bystanders or even to the people involved), but which actually conceal motivations, include private significance to the parties involved, and lead to a well-defined predictable outcome, usually counterproductive.”
One of those ‘games’ is called the ‘blemish game’. In this game, the (possibly unconscious) aim of the game’s instigator is to keep everyone, including oneself, looking in a direction other than the key direction. This involves relentlessly pointing to the failings of others and deflecting attention away from one’s own contribution to proceedings.
Unless everyone can occupy what Berne calls the ‘adult ego state’ (distinct from a parent or child ego state), dialogue and relationships are compromised.
Stating your position, plainly and straightforwardly, would fit the ‘adult’ role. It is very hard to argue about something when the real something is different. I ended up thinking that this is exactly what was happening at this hearing, and it made it hard for everyone to approach their task.
People have many and varied views on issues of our times. Misinformation and disinformation are rife. At the same time, people are entitled to hold whatever views they wish. Why not just state your view – especially if your case hangs on that position? In a court of law any view, if it informs a submission, would rightly be scrutinised. If a view underpins a party’s position, it is good faith to name that view and to articulate it clearly. Then everyone can proceed with trust. Without that basic ground-rule being observed, there is a pervasive sense that discussion of the issues is missing the point.
Going back to my original questions, I wonder now whether the reason the case took so long to come to court was because the system around P got caught up in the ‘blemish game’, chasing more and more evidence that the vaccine would be in P’s best interests, in the hope of consensus. This pattern casts everyone in a perpetual conditional-to-striving reciprocal relationship, where the conditions are never met. . As Berne’s theory of transactional analysis would suggest, the system ended up in a “well-defined predictable outcome” – a lack of consensus that was protracted and counterproductive.
The judge answered my question about how much the Court can become involved in the whys and wherefores of medical treatment (in this case COVID vaccination) – very little and they must rely on accepted authorities’ evidence.
The third question seems trickier. What do care homes and the treating medical teams need to understand in order to navigate and (if necessary) expedite medical treatments for people who lack capacity, when there is family opposition? For P in this case, if they had realised they were engaged in a ‘blemish game’ they might have brought the case to court sooner. How would one realise?
Perhaps the seriousness of the decision in question could be a guide – in this case P is a 39- year-old man with a learning disability, in a pandemic for which, as Victoria Butler-Cole QC emphasised, the evidence shows that “people in care homes and with learning disabilities are at increased risk [of COVID]”. Given the increased risks for P, the care home or health care team and CCG should have brought the case to the Court of Protection sooner, as soon as agreement could not be reached. The Vice President of the Court of Protection, Hayden J, has often said in hearings (across a range of contexts) that “delay is inimical to P’s welfare”.
The court navigated the issues of the argument, as presented by CT, in a straightforward and logical manner. It would have been possible for counsel to take a more compassionate, less adversarial, position if they had been addressing a clear (good faith) position. Instead, they were presented with needing to expose what they suspected was CT’s actual position underpinning her opposition to the vaccination for her brother.
As it transpired, I think what happened was probably more upsetting and uncomfortable for CT, in the spotlight of a (virtual) courtroom with observers present, than had she simply stated her beliefs outright.
Of course, she would have known that to do so would not have been supported by the weight of the internationally accepted scientific evidence (on which the court must rely), and would be likely to be dismissed. So, she was in a bit of a double-bind.
It must be isolating to be faced with the establishment position, when you hold a diametrically opposed view. I had no doubt throughout the hearing that CT believed that she was acting in her brother’s best interests – whatever the underlying reasons for opposing a vaccination for him, she expressed love for him and wanted what she thought was the right outcome for him. I’m not sure that was sufficiently acknowledged by the court.
Furthermore, CT’s (and P’s) father was also a party to, and present at, the hearing. He listened to proceedings and confirmed to the judge that he was in favour of P receiving the COVID vaccination. This must have compounded the sense of isolation that CT reported feeling.
Any of us can get caught up in the blemish game, especially when we feel strongly about an issue and we’re outnumbered and isolated. Someone holding the ‘adult ego state’ is required. Compassionately acknowledging that, if a person holds non-mainstream narrative views, that they feel unable to air straightforwardly, though understandable, this presents everyone with a very difficult task when trying to resolve a dispute.
The judge did say that CT’s position “clouded” proceedings. If there was anything the court could have done differently, I think it might have openly acknowledged the emotion of the situation, and the discomfort CT might have been experiencing in relation to the court’s position of having to rely on officially recognised mainstream medical evidence.
3. Is P’s sister an ‘anti-vaxxer’ by Celia Kitzinger
In the hearing, P’s sister took strong exception to her position being labelled (by counsel for the local authority) “an anti-vax stance”. She said it was “not accurate at all” and that it was “abhorrent that I’ve been characterised in this way”.
The problem with labelling someone as “anti-vax” is that there’s a spectrum of views from people with a range of different concerns, hesitancies and skepticisms – both about the vaccine itself, and about the government responses to it.
Yet throughout the hearing it was hard (as Claire Martin points out) to see her opposition to her brother having the vaccine as driven by anything other than strong scepticism as to the merits of the science underpinning COVID-19 vaccination.
The arguments she raised were, in essence:
- COVID-19 is unlikely to be dangerous to P. This is because he’s “very robust immunologically” and apparently did not contract COVID-19 when there was an outbreak in the home and all other residents did become ill. He’s a relatively young man (39 years old), he has “no respiratory conditions, no liver or kidney malfunction” and in her view COVID might be “unpleasant” for him, but would not put him “significantly at risk”.
- Vaccination may be dangerous for P. Not only is it likely to require some restraint which he would find distressing, but also there are risks, she said, such as myocarditis. She said the vaccine can possibly cause COVID infection, or neurodegenerative disease, and can possibly be lethal in some cases – plus there are also potentially dangerous interactions with anti-psychotic and anxiolytic drugs P is receiving. She believes, in the context of mounting evidence that COVID vaccination does not confer full immunity against COVID infection, the risks of vaccination do not outweigh the benefits. She also highlighted that there are more deaths from COVID-19 among those who have been vaccinated as compared with those who are not vaccinated[4].
- The evidence provided to her by health care professionals about the risks and benefits of vaccination is not trustworthy. In her written statement (read out by counsel for P), she’d said that – contrary to medical claims – vaccines “do not limit or prevent infections” and “do not limit or prevent death”. She repeatedly said that health care professionals had failed to engage adequately with her questions and concerns about – for example – drug interactions and the idea that vaccination was “experimental treatment”. She said: “the questions I raised were tainted by the way vaccines have been presented in the media, with exaggerated claims that they are contributing massively to the reduction of COVID.” She wanted “upfront acknowledgement of the risks of vaccination” and had submitted to the court various Excel spread sheets which set out her own analysis of scientific data relating to the risks and benefits of vaccination.
Counsel for the CCG (Ben Tankel) commented that although P’s sister’s opposition to COVID vaccination for her brother “is sometimes presented not as outright opposition but rather that more information is needed”, what it amounts to is “really just another way of saying ‘I am opposed to this vaccine, and the onus is upon you to convince me otherwise, and unless you can convince me otherwise there is an insufficiency of evidence’.”
Counsel for P (Victoria Butler-Cole) likewise said in her closing summary that CT’s position “boils down to the fact that she doesn’t accept vaccination is safe, or that it works, or that he’s likely to get ill if he doesn’t have the vaccine”.
These assessments were supported from what I discovered when searching for P’s sister online.
P’s sister online
Although her identity is protected by the transparency order, her name was freely used in the course of the hearing and so I was able to google her to see whether there was any evidence online of her stance toward vaccination.
I found that she has set herself up as a specialist in law and ethics, with a website offering legal support to members of the public.
She’s already made public the fact that her brother might be subject to a forced vaccination order. She said that her family had declined other vaccinations on his behalf “for years”.
I learnt a lot about her views on vaccinations in general, as well as on COVID-19 in particular. I’ll try to convey an accurate impression of those views, without quoting what she says directly at any length (because it could lead to her identification).
Her views are not “mainstream” (ie. they are clearly different from those adopted by the court) but nor are they purely idiosyncratic. They are shared by others who are sometimes branded “anti-vaxxers”, including some of the people I quoted in the Introduction to this blog post.
She’s “very concerned” about vaccinations for infants: for example, the single 6-in-1 vaccine that is routinely given to babies at 8, 12 and 16 weeks to protect them against diphtheria, hepatitis B, haemophilus influenzae type b, polio, tetanus and whooping cough. She’s “appalled” that parents are simply expected to have their babies vaccinated without (in her view) being given relevant information about the risks and benefits of vaccination. She sees it as “coercive”.
She’s not surprised by government policies on COVID-19 vaccine because, she says, it’s an extension of the “coercive mentality we all have to obey” that starts at birth with childhood vaccinations and has culminated with the policies put in place during this (purported) pandemic. (I think she is sceptical as to whether, in fact, there is a genuine pandemic.)
We are, she says, ground down by relentless “vaccine ideology” and propaganda about the safety and efficacy of COVID vaccination: it’s as if we are under “a spell” (she says) as we all line up obediently to be vaccinated.
She wants us to be “free of the system”, to become authentic and autonomous self-directed beings, acting according to our own inner values and to “step outside of the mass coercive society”. She advocates “critical thinking” and spiritual development.
Having researched vaccines over a period of 15 years, CT she feels equipped to take aim at a mishmash of targets which, she says, account for the current “scary”, “crazy” and “dangerous” situation that has led to compliance with a mass vaccination programme. She attributes our submissiveness variously to: capitalism, consumer culture, Western culture, postmodernism, widespread internet use, loss of connectedness with each other and loss of connection with nature. We need to “wake up”.
She also raises questions about how vaccinations are funded within the NHS. Big Pharma, she says, is raking in millions.
She repeatedly refers to her research (by which she means, reading books about vaccination), and to her credentials as someone with a bioethics degree. Her cited sources include many of the people branded as “anti-vaxxers” by their opponents. They include Judy Mikovits who claimed that a virus possibly implicated in chronic fatigue syndrome was possibly delivered through vaccines; and Ed Hooper’s book, The River: A Journey to the Source of HIV and AIDS, who advanced the theory that the origin of AIDS could be traced to oral poliovirus vaccines administered in the Belgian Congo between 1957 and 1960 (subsequently debunked).
In court, CT declined to answer the Official Solicitor’s question as to whether or not she’d been vaccinated against COVID-19 herself. But she has said online that she is “strongly” opposed to vaccination and would “never” be vaccinated.
She is however willing to accept other people’s autonomous decision to be vaccinated, and acknowledges that there may be risk factors (like being over 65, or having a respiratory condition) that might change the risk/benefit analysis for some people.
So the online evidence is that there was, as Claire Martin proposes, and as the judge found, a disjunct between CT’s ‘authentic’ views, as expressed in her online engagement with people who share her broad perspective, and the more cautious and circumlocutory position she took in this hearing.
Implications of CT’s position for P
If an ‘anti-vaxxer’ is someone who is always, under all circumstances, opposed to vaccination for everyone, the evidence is that CT is not an “anti-vaxxer”.
She is, as far as I can tell, opposed to vaccination for herself and for her brother based on her own assessment of the risk/benefit ratios, but she’s willing to accede to other people’s wish to be vaccinated if they are in the small group of people with risk factors (in which she’s never to my knowledge included people with learning disabilities) – and if they are not simply sleep-walking into vaccination based on brainwashing from the government.
But the term “anti-vaxxer” is often used in a more inclusive manner.
According to an article in Nature, referencing the Centre for Countering Digital Hate,
“Every anti-vaxx message can be boiled down to a master narrative of three parts:
- COVID-19 isn’t dangerous;
- vaccines are dangerous;
- you can’t trust doctors or scientists.”
This is pretty much what P’s sister argued in court and in her online materials.
If this is the position you start from, it must be hard or impossible to understand why other people are of the view that it would be in your brother’s best interests to be vaccinated against COVID-19.
It makes sense to contact someone with the resources of an organisation like UKMFA to ask for support when up against a court application to vaccinate P.
It also means P’s sister had a choice between: (1) standing firm and saying what she believed to be true, challenging the mainstream; or (2) trying to ‘game the system’ by accepting the ‘best interests’ premises of the court and seeking to influence the risk/benefit analysis.
On the basis of my observation of many court hearings, I don’t think either approach would have resulted in the outcome she wanted.
For the reasons outlined earlier, it seems likely that for the vast majority of COVID vaccination hearings – at least for protected parties whose own wishes and feelings cannot be ascertained – the court will rule, on the basis of overwhelming scientific consensus, that vaccination is in P’s best interests. It increasingly feels like a foregone conclusion.
That is how impartial administration of the law works, in practice, to uphold mainstream science and government policies.
The role of the Court of Protection is thereby, inevitably and inescapably, in my view, part of the “politics of the pandemic” and not aloof from it.
4. How to refuse COVID vaccination by Celia Kitzinger
Those of us deemed to have mental capacity to make our own decisions about vaccination can decide either to consent to, or to refuse, the offer of COVID vaccination – and if we refuse there is no legal requirement (in England and Wales, or Scotland) for us to explain our reasons for doing so, or justify our decision.
It’s quite likely that enquiries might be made as to the reason for refusal, in case more information or explanation might change the decision, or in case the offer of an alternative place or mode of administration might be helpful. Seeking to understand why people refuse treatments and offering alternatives is part of supportive healthcare.
There may be also be attempts to persuade or incentivise (in New York with pizzas and Big Macs; in Austria with brothel visits).
There may be restrictions on the unvaccinated (as in Austria, Italy and Germany, and as feared in the UK).
Mandating COVID vaccination for all NHS staff who work in health and social care settings regulated by the Care Quality Commission (currently due for implementation in April 2022) is a clearly “persuasive” or “coercive” move insofar as job retention may depend on vaccination: one hospital chief said: “There’s a possibility if they choose not to be vaccinated they could be redeployed. And if we can’t find that opportunity to redeploy them then the consequence is that they will [not have a job].” But even he added “We will not make individuals be vaccinated…. ultimately it is their choice“.
What he meant, I assume, is that – after the attempts to persuade, incentivise, and encourage you to have a COVID-19 vaccination fail, and if you still refuse vaccination despite the loss of your job – nobody can lawfully physically restrain or sedate you and administer the vaccine against your will.
That is what changes when you are deemed to have lost capacity to make your own decision about vaccination.
Refusing for your future non-capacitous self
We are all potentially no more than the blink of an eye away from a stroke, a cardiac arrest, a car crash, a sporting accident – some unexpected injury which could mean that we lose capacity to make our own medical decisions.
Unless you have made a legally binding refusal of COVID vaccination in an Advance Decision to Refuse Treatment (ss. 24-26, Mental Capacity Act 2005), then once you are deemed to have lost capacity for this decision, it’s someone else’s job to decide whether or not vaccination is in your “best interests”. The decision-maker must take account of any views you may have expressed before you lost capacity (in writing or via family reports), and your present wishes and feelings, in so far as they are ascertainable. But neither your past nor present views about vaccination are determinative. They are considered as just one element of best interests decision-making in the context of mainstream scientific research.
And if there’s disagreement between the people who care for you and are concerned for your welfare (your family, friends, treating clinicians, paid care staff), then you could be “P” in the Court of Protection with a judge having to decide whether or not you should be given COVID vaccination (or any other medical treatment for that matter).
If you know now that you would want to refuse COVID vaccination if you were to lose capacity in the future, the best thing to do to ensure your wishes are respected is to make an Advance Decision to Refuse Treatment. This is legally binding on clinicians (they could not then lawfully vaccinate you) and it would avoid painful and lengthy arguments between your family and your treating clinicians about what it in your best interests (and potentially a court hearing).
You can check out Compassion in Dying for information about how to prepare these documents, but if vaccination is the ONLY medical intervention you want to refuse at this point, it’s very simple. It’s a method also used, for example, by Jehovah’s Witnesses who want to refuse blood products. You simply write something like this:
“I refuse vaccination against COVID-19 (including boosters and any variations of the vaccination not yet invented) under all circumstances. I make this refusal knowing that, according to mainstream science, my life may be shortened as a result.”
You need to sign and date it in the presence of a witness (who can be anyone you choose – all they’re doing is witnessing that they saw you sign it), and then ask your GP to put it on your medical records. That’s it. (Note that the bit about “my life may be shortened as a result” is required by law and your treatment refusal won’t be valid without it, see 25(5)(a) Mental Capacity Act 2005). You don’t have to give your reasons – though you may of course choose to, and if you do, this may make your treatment refusal more “persuasive”.
I believe it’s very important to make a formal, written, witnessed, Advance Decision to Refuse Treatment if we know for sure that we wouldn’t want COVID-19 vaccination after loss of capacity to make that decision for ourselves.
Without it, doubts will inevitably arise.
It’s not necessarily straightforward to extrapolate from the choices a person made before they lost capacity to what they would want after losing capacity.
Some people who refused vaccination on the basis of their own risk/benefit analysis when they were healthy and living in their own homes might make a different risk/benefit analysis and wish to receive vaccination if they were to become brain-injured, vulnerable and were now in an ICU or care home with an increased risk of contracting COVID-19 and/or becoming seriously ill as a result and/or passing on infection to others with whom they live.
Some people who consented to vaccination when they were healthy may wish to refuse vaccination (and other possible “life-prolonging” treatments) if they were to become brain-injured and no longer able to enjoy (what for them is) “quality of life”. Any opportunity for an ‘early exit’ from that scenario – even the prospect of a fairly unpleasant death from COVID-19 – might be positively valued.
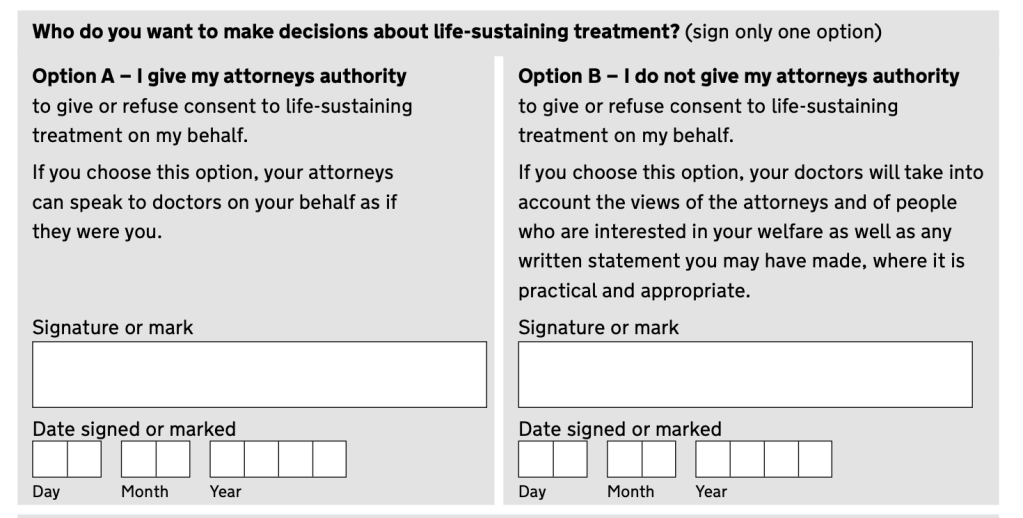
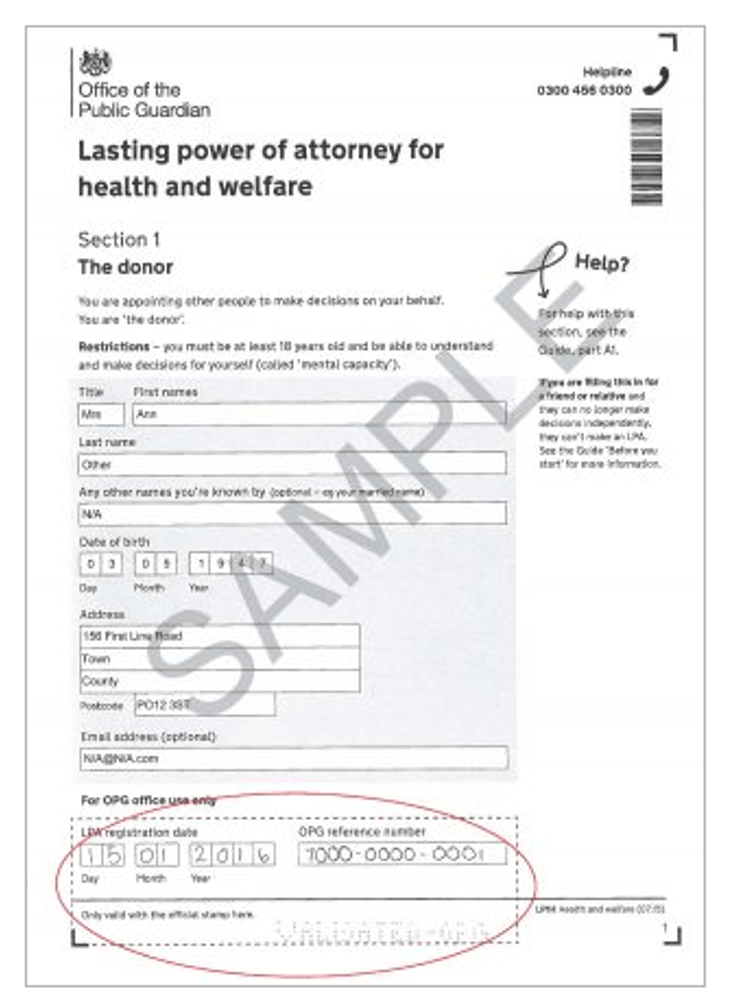
You may not know for sure whether you would want COVID vaccination or not if you were brain-injured in future and unable to decide for yourself. It might feel like there are too many unknowns. In that case, you may be content to leave it with the doctors treating you at the time to decide. Or you could discuss the matter with a trusted family member, friend or ally – someone who understands your values and beliefs and is able to be assertive in medical situations – and appoint them as your Health and Welfare Lasting Power of Attorney (ss. 9-14, Mental Capacity Act 2005) to make that decision for you (instead of the doctors) when you cannot.
But if you know for sure that you want to refuse vaccination (or any other medical interventions), you need to make that Advance Decision to Refuse Treatment now.
Refusing for an (adult) friend or family member
Unless you’ve been appointed by the person (when they had capacity to do so) as their Health and Welfare Attorney, and the documentation has been registered with the Office of the Public Guardian, it’s not your decision about whether or not your brother, spouse, mother, friend or other family member is vaccinated. That decision lies with the person with overall responsibility for the individual’s care (usually their GP) or – if there’s dispute – with the Court.
Supporting advance refusal (ADRT) before the person loses capacity to refuse for themselves
If you are currently caring for someone (perhaps an elderly relative, a spouse, or someone with mental health issues) who has refused COVID vaccination and has capacity to do so, but might lose that capacity in the near future (e.g. because they have a dementia, or Parkinson’s), you might consider asking them whether they want to make an Advance Decision to Refuse Treatment (ADRT) relating to vaccination – and any other treatments, for that matter. Bear in mind, of course, that they might have a change of mind about vaccination if the circumstances were different, and that a current refusal doesn’t necessarily translate into a future refusal, or vice versa – but if they are certain about refusing vaccination after loss of capacity, they should do that now in an ADRT. This enables them to make an autonomous choice about their own healthcare, and relieves the future burden on you of having to explain to doctors (or the courts) what they’d want.
It’s especially important that people you care for should make an ADRT if you disagree with their position on COVID-vaccination. If they don’t make their own advance refusal, you could find yourself in a really uncomfortable position of having to tell doctors/the court what you think they’d want (not to be vaccinated) while simultaneously believing that it would be better if they were vaccinated.
If you are confident that you are able to represent the person’s views and the reasons why they want to refuse COVID vaccination (and other matters relating to their health and welfare), and if you feel able to communicate confidently with doctors, you could ask whether the person would like to appoint you as their Health and Welfare Attorney.
Representing someone’s views after they’ve lost capacity to refuse (without an ADRT)
If the person you’re caring for has already lost capacity to make or communicate their own decision about COVID vaccination, without making an ADRT or appointing you as their Health and Welfare Attorney, then you have a much harder task in representing their wish to refuse vaccination.
On the basis of what I’ve seen in vaccination hearings in the Court of Protection, I do not recommend attempts to challenge mainstream COVID science: for the reasons explained earlier in this blog, I think that’s unlikely to work.
You will need to focus on evidence about their position on vaccination (and maybe medical treatment more broadly). Have you got evidence that they refused vaccines in the past? Did they write anything expressing their views on vaccination – on social media, in letters, in emails? Can you recall conversations with them about vaccination – did they have discussions with other friends or family in which they said anything relevant to vaccination decision-making?
It doesn’t matter whether their objections to vaccination were based on challenges to the science, belief in ‘natural immunity’, fear of side-effects, scepticism about Big Pharma, revulsion at the idea of polluting their body with alien material, or anxiety about government control. They could be what others brand “anti-vaxxers” or “conspiracy theorists” (you might think them entirely misguided or delusional) but they are entitled to hold those views and to have them respected. As Hayden J said, in the one case I’m aware of in which vaccination was not imposed on the protected party: “SS’s reality is undoubtedly delusional, but that does not stop it being her reality. This has to be both recognised and respected.” (§25 Re SS [2021] EWCOP 31)
Refusing for a person who has never had capacity to refuse for themselves
If the person you care for is (as in the case this blog focusses on) someone with a learning disability who’s never had capacity to make a decision about vaccination, and who struggles to understand what COVID is, and how vaccination works, it’s very likely (in my experience of the Court) that vaccination will be found to be in their best interests.
This is because, in considering what is in their best interests, there is no ascertainable view about COVID vaccination from the person themselves to set against the overwhelming message from the mainstream scientific research that vaccination is medically indicated.
The “instinctive reaction” which may lead many people with learning disability to recoil from unpleasant or painful medical procedures does not meet the criteria for capacitous refusal nor is it seen as expressing a view on the merits or otherwise of vaccination: even if it were to be so understood, it is unlikely to weigh heavily against the medical benefits as determined by mainstream science.
In the case this blog has focussed on, attempts to elicit P’s views were unsuccessful and this clearly influenced the position taken by the Official Solicitor:
“It does not appear possible to elicit P’s views about the vaccine. It is possible that when asked about it by his solicitor he was saying he did not want an injection, but equally possible that he was asking for the WhatsApp call to end. Even on the assumption that P does not want an injection, this appears to be an instinctive reaction to a mildly unpleasant medical procedure. This has to be balanced against the potential benefits to P, which he is not able to understand or weigh.” (Counsel for P via the Official Solicitor)
In several cases I’ve observed, parties have attempted to advance arguments about what position a never-capacitous P would have taken in relation to COVID vaccination if they had capacity. These counter-factual arguments are fraught with difficulty.
In one recent case, the mother of a young woman with “severe learning disability” suggested that her daughter would “ “almost inevitably” have “expressed the same views as her mother” if she’d had capacity to do so. Rogers J noted that there was simply no evidence at all of the young woman’s own views, and to speculate on them would not be right (blogged here).
In another case (blogged here), concerning vaccination of a fifty-year-old man (JS) with “severe learning disability”, from whom people had likewise been unable to elicit any views about vaccination, counsel for the applicant GP Practice (in favour of vaccination) speculated that “it would be unlikely for any adult to wish to be at risk of severe disease and death” and took the position that JS, if capacitous, would be that hypothetical person of legal fiction, the ‘reasonable man’:
“It is reasonable to consider that any person with capacity who was at heightened risk from COVID-19 would wish to minimise the risk of serious disease and hospitalisation through vaccination, and would be willing to accept the miniscule risk of harm from the vaccination.” (Conrad Hallin, Counsel for the GP Practice).
His parents took the opposing view that it would be reasonable for JS, if he had capacity and understood the damage that had (they believe) been caused to him as a baby by the triple vaccine, and then by the measles vaccine, to decide not to risk another vaccination with the real risk of vaccination damage.
Claims about what someone who’s never had capacity would decide if in fact they did have capacity and were acting reasonably are rather implausible and tell us more about the speaker’s own wishes, feelings, beliefs and values (and what they think ‘reasonable’) than about the views of the protected party.
I have not seen any evidence that judges use these counter-factual arguments (either from family members or from other parties) in arriving at their decisions.
This hearing raised important issues about the politics of vaccination within and beyond the court.
- How do health care professionals ensure that people who can’t consent to medical treatments receive the best possible care that (mainstream) science can offer in a timely fashion – even when family dissent?
- How do we recognise and respect diversity of opinion – for families, for clinicians, and for the vulnerable people at the centre of these cases?
- What is required to ensure that P’s voice is truly heard (where possible) and respected?
- Bearing in mind that all of us may be future Ps, what can we do to plan in advance to safeguard our own autonomy?
We’d welcome feedback and commentary on these and other issues raised in this blog post.
Celia Kitzinger is co-director (with Gill Loomes-Quinn) of the Open Justice Court of Protection Project. She tweets @KitzingerCelia
Claire Martin is a Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a member of the core group of the Open Justice Court of Protection Project and has published several blog posts for the Project about hearings she’s observed (e.g. here and here). She tweets @DocCMartin
Daniel Clark is a paid carer. He is also deputy director of Backbench: an unaffiliated, open platform, blog that publishes a range of articles about current affairs. He has recently completed an MA in Political Theory. He tweets@DanielClark132
[1] We have blogged about a number of these hearings: for example, Covid vaccination and a Christmas visit; Covid vaccination contrary to parents’ wishes; Covid vaccination in the Court of Protection; Disputes about COVID vaccination should be rapidly referred to the Court.
[2] All material quoted from oral submissions and oral evidence in court is based on notes taken contemporaneously during the course of the hearing. Quotations are as accurate as possible, but given that we are not permitted to audio-record court hearings, it is unlikely to be word perfect.
[3] According to the GMC website, checked by Celia Kitzinger in the course of posting this blog for publication, Dr Jon Rogers very recently relinquished his registration (on 12th January 2022) and may not now practise as a doctor in the UK.
[4] This was addressed by Victoria Butler Cole, counsel for the Official Solicitor, in her Position Statement: “The suggestion that people who are vaccinated are more likely to die than those who are not is based on a misunderstanding of risk. It is inevitable that as a majority of a population are vaccinated (and in particular the older members of the population), there will be more deaths among the vaccinated, measured absolutely. The relevant metric is what the rates of death are among the two groups, and the clear evidence is that the rate of death among the unvaccinated is 32 times higher than among the vaccinated. Lay explanations of this are available at: “Why most people who now die with Covid in England have had a vaccination” and “How do death rates from COVID 19 differ between people who are vaccinated and those who are not?“