In a case in the Court of Protection last week, a judge authorised the use of force, if necessary, to ensure that a young woman gives birth in hospital rather than at home.
The woman (call her ‘P’) has severe agoraphobia, and has barely left her home in four years. Her doctors believe that it would be best for her to deliver her baby in hospital. But P has an overwhelming fear of leaving her home and cannot agree to this. Their particular concern is that P might develop a serious complication during her home birth, need emergency transport to hospital, but be unwilling or unable to agree to this because of the severity of her phobia.
At the conclusion of a three-day hearing, Mr Justice Holman declared that P lacked capacity to make the relevant decisions and ordered that it was lawful and in her best interests for medical staff to transfer her to hospital a few days before her estimated due date, and for medical professionals to offer her a choice of induction of labour or Caesarean Section in hospital. He also gave permission for the use of restraint, if necessary, in the event that she refuses to go to hospital voluntarily.
On the face of it, this looks like an extremely concerning infringement of a patient’s autonomy – a view that has been expressed by members of the public responding to media reports (e.g. see the blog post here). We normally think that adults should be free to make decisions about their medical care, including the freedom to refuse treatments that doctors are recommending. Decisions about place of birth and mode of birth are deeply personal decisions that can be hugely important for many women. For that reason, doctors and courts should be extremely loathe to infringe upon them.
Is it justified in this case, then, to physically restrain P and treat her against her wishes? In particular, is it justified to do this pre-emptively, before a complication develops?
One question is whether home birth is more risky than hospital birth. Large studies indicate that women who plan to deliver at home and are at low risk of complications have lower rates of medical interventions in labour, slightly lower rates of serious bleeding, and similar rates of serious newborn illness. (There are few studies specifically focused on the risk of long-term disability in the child. There is some reason to be concerned that this rare risk is potentially increased in home births.) But those reassuring statistics are based on having the option of transfer to hospital in case of emergency. That occurs in between 1 in 10 to 1 in 3 home births. (In the case of P, a higher risk was cited in the courtroom – of approximately 1 in 2, with about 1 in 100 requiring emergency “blue-light” ambulance transfer. It is not clear the basis for that higher figure). If P were to develop a complication at home and were not able to be transferred to hospital, there would be a significant risk of harm. But harm to whom?
If P were to have a complication of childbirth there would be the risk of harm to herself. But there would also be the risk of harm to the baby and future child. Some jurisdictions and health systems have compelled women to have caesarean section for the sake of safeguarding the interests of the fetus. But in UK law, the interests of the fetus are not (directly) relevant to decision-making. The only considerations relevant are the woman’s capacity to decide, and, if she lacks capacity, her best interests.
Do phobias affect capacity? “Capacity” is the technical term for an individual’s ability to make decisions. The question is whether the person can understand information relevant to the decision, whether they can remember it, whether they can weigh up the pros and cons, and whether they can communicate their decision (s. 3 Mental Capacity Act 2005).
Mild forms of ‘phobia’ (for example, fear of heights, needles or spiders) are extremely common (one estimate is that they affect 10 million people in the UK). But to be diagnosed with a phobia, that fear must be excessive or unreasonable, persistent and intense. Severe phobias can be incredibly debilitating.
Most people with phobias will still retain capacity to make decisions. Decisions that have nothing to do with their phobia will obviously be unaffected. But many people with a phobia can still make decisions affected by their phobia. For example, someone with a needle phobia could decide to have a blood test if they understand that it is particularly important for their health.
For phobias, the relevant issue is not understanding or retaining or communication. It is weighing. Being unreasonable, giving excessive weight to one choice or making an unwise decision is not enough. For someone to lack capacity they must be unable to evaluate their choices. The issue is that a severe phobia can completely undermine an individual’s ability to weigh up the different considerations. Even thinking about the possibility of leaving the home could be enough to cause severe anxiety in someone with severe agoraphobia. If someone has a severe enough phobia, there is literally no consideration that could outweigh their fear.
In P’s case, it was apparently accepted, without argument, that P lacked capacity to make decisions about delivering in hospital or at home. (She was also reported to have problems affecting her short-term memory and ability to “manage and process complex, multifaceted information”).
The question then turns to whether it is in P’s best interests to have a home birth or to give birth in hospital.
There were two main options considered. The first was for P to give birth entirely at home, even if complications were to develop (unless in that circumstance she changed her mind and agreed to transfer). The second – the option endorsed by the judge – was for P to be transferred to hospital in advance of labour to give birth in hospital. (For this blog I will not discuss the further question of the choice of mode of birth, i.e. waiting for natural labour versus induction of labour versus caesarean section).
A third option, would be for P to attempt to have a home birth and to be transported to hospital (potentially using sedation or restraint if necessary) if a complication arose.
One relevant factor for P’s best interests is the medical risks to her and her baby of the different proposed options. It seems clear that home birth (without the option of emergency transfer to hospital) would pose small but significant risks to P’s health. I earlier set aside the direct legal relevance of the interests of P’s unborn child. However, the health of the fetus/baby is relevant to P’s best interests in a different way. In the judgment it was mentioned that P “dearly wishes to give birth to a healthy baby, undamaged by the process of birth”. That strong desire would mean that the health of her child is relevant to her own interests.
But there is more to consider. It would be important to consider the effects of different options on P’s mental health. Giving birth at home (if uncomplicated) would be likely to cause least anxiety to P. But if she were to develop a serious complication and her baby were to be seriously ill or die – that would predictably have a long lasting profound negative impact on P’s mental health. If P were transferred to hospital in advance of labour (or in an emergency) that would also predictably cause her significant distress. In the judgment it was noted that this “may entrench her agoraphobia. It may damage or impair her bonding with her baby. It may give her long-term flashbacks. It may compromise her attitude to future pregnancies, or her dealings with persons in authority.”
Finally, one important consideration is P’s own wishes and values. Best interest decision-making for patients who lack capacity typically places a great deal of emphasis on the individual’s values, wishes, preferences and feelings (s. 4 Mental Capacity Act 2005). What weight then, should be placed on P’s desire for a home birth?
In other recent court cases (for example this one), patients’ long-standing desires about treatment were highly relevant, even though they were deemed to lack capacity. There could be patients with agoraphobia who also (for example), have a strong desire for a natural birth in their own home, avoiding medical intervention.
Mr Justice Holman’s view was that, in this case, P’s desire for a home birth was entirely as a consequence of her agoraphobia. “The mother herself says that she would prefer to give birth at home, but she clearly expresses that that is due to her agoraphobia and fear of going out. I am satisfied that, but for her agoraphobia, the mother herself would opt for a hospital birth,” (para 22). Without further information about P, it is difficult to evaluate this claim. But even if some weight were given to P’s desire for a home birth, the further question would be how to reconcile potentially conflicting wishes. P also strongly wishes for her baby to be healthy.
Mr Justice Holman concluded that option 2 (planned hospital birth) better promoted P’s interests than option 1 (home birth without transfer).
But the judgment did not to my mind completely settle whether option 3 (home birth with emergency transfer) would not be better still. The Official Solicitor (representing P) argued that it was not proportionate to sedate and restrain her in the absence of an emergency. An emergency occurring in labour would be unpredictable. That could obviously occur at any time of day or night. It may be more difficult to ensure that community psychiatric staff and staff with training in judicious restraint would be available. But it may be possible for some planning to occur. For example, trained staff could make themselves available to be called in an emergency. At the start of labour, midwives attending P in her home would potentially be able to pre-warn the ambulance service or community psychiatric staff. The judge referred to delays in a previous case in obtaining urgent court authorisation for restraint and emergency transfer. But that would not apply in this case, since the court was able to consider the issues in advance. There would inevitably be some increased medical risk in that plan. But it would also give P the greatest chance of being able to have a non-medicalised birth in her own home. Given that P does not have medical features that put her at particularly high risk of complicated home birth, it does seem to potentially be a reasonable compromise and the least restrictive approach to securing P’s interests.
Best interests judgments by their very nature require a complicated weighing process. There is no simple or mathematical way of balancing competing considerations, and different people may reach different conclusions (because of varying assumptions about the probability of different outcomes, or the weight placed on different values). One of the values of the Open Justice Court of Protection Project is the support it provides for observers to watch hearings, hear evidence themselves, and to better understand how the final balancing was reached. (That was not possible in this case.)
There can be rare situations where it is in a woman’s best interests to give birth in a place or via a mode of birth that is contrary to her strong preferences. But whether it is ethically justified in P’s situation, remains – for me at least – an open question.
In a previous blog I discussed a hearing before Mr Justice Hayden (COP 11919290 Re LW 29th March 2021) about a woman I called Lucy, her sister (who I called Angela) and an urgent decision about where Lucy should be discharged to, from a current inpatient stay (due to a fractured leg, sustained at her previous care home).
Although that crisis had been occasioned by the fractures, the court proceedings began back in April 2020. Angela wanted Lucy to live with her. She wanted to care for her on a full-time basis – and she wanted to be the primary decision maker, so was seeking a court-appointed Deputyship. A key aspect of decisions around Lucy’s care, as presented by Ruth Kirby QC (counsel for Angela) at the 29th March hearing, was the Local Authority suggestion that living with her sister or family would compromise Lucy’s ‘dignity as an adult’. It was submitted to the judge, by Ruth Kirby, that this interpretation of ‘dignity’ was given undue weight in assessing best interests care provision for Lucy. In the previous blog I started to wonder how the concept of ‘dignity’ is framed and operationalised in our systems of law, care and Human Rights, and this piece[1] expands on these thoughts. I am a psychologist, not a philosopher or lawmaker: these are my initial speculations and I invite commentary.
What do we mean by ‘dignity’?
The OED defines “dignity” as: “The quality of being worthy or honourable; worthiness, worth, nobleness, excellence.”
Etymologically, the word stems from the Latin ‘dignitas’, meaning “merit” and “to be worthy”. My take on this is that the origins of the word would suggest that dignity is something all humans have inherent in their humanity – it is a ‘quality’. Dignity is a given. We simply have it, just like we have a heart, and no one can take it away.
In a review of a 2017 book called Dignity: A History edited by Remy Debes, the reviewers summarise:
“At a certain moment in the history of ideas, dignity became attached to “humanity”, and acquired a foundational moral value. … Christianity taught that original sin blemished human dignity and that only Christian grace offers some restoration. For many centuries, this move rendered dignity … irrelevant as a moral property of all humans. People were expected to behave with dignity and to accept the grace of the Church and her teachings; but they did not hear about any treatment owed them solely because all human beings had dignity. … The notion of “the” or “a” dignity of man surfaced in the Renaissance … The meaning might not have always been the same, but the term has persisted. Interactions with the indigenous people of the New World required European law and theology to come to grips with the moral and legal status of real humans, a sharp departure from the medieval discourse on “monstrous” races and people. In the nineteenth century, “dignity” was a motivating theme in the Latin American struggle for independence from Spanish colonialism. In 1945, four countries mentioned “dignity” in their constitutions. In 1948, the UN Declaration of Human Rights celebrated “human dignity” as its foundational value. By the end of the millennium, over 150 countries incorporated human dignity in their constitutional law. About ten years ago, an unprecedented wave of scholarly books on human dignity in ethics, bioethics, political theory and law began rising.”
This paper by Saxena in 2015 describes more recent, 20th century, uses of dignity such that:
“it was introduced into legal frameworks in the twentieth century through the Universal Declaration of Human Rights (UDHR) in its first article which enshrined the notion of universality of human dignity in international law, by stating that, ‘All human beings are born free and equal in dignity and rights’.”
So the idea that we are born with dignity, if this is how it has come to be seen, would suggest to me that it is not something that can be removed – it can be attacked, violated, humiliated perhaps, but not removed. How, then, can it be a ‘right’? It’s leading me to think about who gets to define ‘dignity’ and the political history of its use. The review of Debe’s book, above, suggests that the Western social and political framing of dignity has become dominant – and what I have read suggests that this has then filtered into law and its interpretation, particularly in Western countries. From that, its use will filter into social practices including health and social care via case law. I wonder whether Lucy’s Local Authority was basing their idea of ‘dignity as an adult’ on any previously contested cases or on written guidelines that they adhere to?
That line – ‘dignity as an adult’ – suggests some fairly fixed criteria. It seemed, for this Local Authority, one benchmark is ‘not living with one’s parents’. They are not able to contribute to this blog – so of course this might not be how the Local Authority interprets it – it could be that the particular staff involved were of this view, and were not reflecting an organisational standpoint. However, to hold this position, especially in a court hearing, as a reason why a person should not live in a particular setting seems to be a view that is held strongly enough to prohibit consideration of that option. In short, whilst the Universal Declaration of Human Rights states that “all human beings are born free and equal in dignity and rights”, authorities and organisations have tended to qualify dignity in terms of a set of criteria. Any such qualification by definition undermines the rights of all persons to claim dignity.
For example, the qualification of dignity in relation to living independently from one’s parents normalises white, Western households. What does that principle say about people from communities who live in multi-generational households as a norm, both in the UK and around the world? Or people who (with capacity) choose to live with their parents, for whatever reason? How has the human need for care and community with other people become a criterion for assessing dignity?
Dignity in law
Dignity also seems like a very tricky concept to use in law. How can it be operationalised? I got a bit lost down the rabbit hole of the legal approach to human dignity in the UK, and legal scholars would be much better placed to discuss this than I am!
I did find an article from 2012 by Conor O’Mahony really interesting: “There is no such thing as a right to dignity.” His end point (I think!) is that the idea of ‘dignity’ as a right should be abandoned and separated from rights that can be measured and put into operation more easily – such as autonomy and equal treatment. He quotes William Binchy (an Irish lawyer): “[i]ts meaning depends greatly on the philosophical premises of those who invoke it; the range of such premises is so broad that ‘dignity’ can have completely opposing connotations.”
The concept of dignity has been used variously as something which people have a human right to, and also as something on which human rights depend. It can’t be both really. My – probably simplistic – take on the subject, is that human rights are not something that just exist, out there: we organise to agree what ‘rights’ we give to one another and we invent structures to hold organisations and states to account for upholding (or not) those rights. I’m not sure how useful it is to place dignity as a right – as William Binchy says:
“As a baseline for recognizing our shared humanity, equal human dignity has a ringing appeal. But in concrete cases, human dignity will often fail to provide any specific guidance precisely because there are many different and conflicting conceptions of what dignity may require.”
Quite.
Dignity in care
What about ‘dignity’ in our systems of care? What is it meant to look like? How do we know if it’s happening?
In a quick internet search on dignity in health and social care, I could not find any principle where ‘dignity as an adult’ is conceptualised in the way it seemed to be for Lucy.
In the Health and Social Care Act 2008, ‘Regulation 10’ is entitled ‘Dignity and Respect’ and has the following guidance: “Staff must respect people’s personal preferences, lifestyle and care choices“.
The 2009 Royal College of Nursing document, Dignity in Healthcare for People with Learning Disabilities, reads like this:
So with reference to that third bullet point – not too far away from one’s family and friends, but not too close either!
Whilst it might not be known exactly what is Lucy’s personal preference for where she lives – it is likely that increasing distress, behaviour that others find challenging, and an unwillingness to eat are communications of dissatisfaction with something about her current circumstances, warranting further assessment. I would argue that it is narrow and selective that a rule or idea about what it means to be ‘an adult’ might outweigh other relevant factors in making a decision about someone’s life – such as a person’s relationships and where they evidently feel safest and most at ease.
The SCIE (Social Care Institute for Excellence) weblinks (1) here and (2) here to Defining Dignity in Care suggest dignity involves:
“ …treating [people] as equals and providing any support they might need to be autonomous, independent and involved in their local community..”
“Dignity in care means providing care that supports the self-respect of the person, recognising their capacities and ambitions, and does nothing to undermine it.”
This would suggest that, when thinking about the concept of ‘dignity’ in care settings, there is something crucial about the lens being from the perspective of the cared-for-person – when and how do they feel safe/respected as equal/autonomous? how do we know this? which relationships are key to this safety/equality/autonomy? what are the conditions to enable this person flourish in all ways possible? This might be very different for each of us. Is it possible that services/others impose a meaning of ‘dignity’ on a person, from the perspective of their own lens? So: ‘X is an adult – it’s not appropriate (dignified) for them to be living with their family’.
In older people’s services there has been contention over doll therapy for people with dementia and whether this practice compromises ‘dignified’ care. There’s a body of research around the benefits and concerns of using dolls for people with dementia as part of their care. This paper by Alander, Prescott and James highlights that: “Clearly, there is an ethical tension in doll therapy involving dignity, autonomy and benefit. … At the heart of the ethical dilemma is how other people view and respond to doll therapy within the care home settings”.
Who could argue that ‘dignity’ should not be maintained? It all feels a bit vague – and entirely subject to individual, system and cultural views on what constitutes ‘dignity’. This brought to mind Ernesto Spinelli, a psychotherapist and existential theorist, and the difficulty in defining ‘therapy’ (see Demystifying Therapy 1994). He invokes Wittgenstein’s argument for ‘open concepts’ and the example of games:
“While it may seem, at first, to be the easiest thing in the world to define a game, nevertheless, as Wittgenstein so ably showed, this is far from the case. For the concept of games is an open one in that, on closer inspection, there exist no features that are common to all games. … While all games share some properties with some other games, no games share all properties with all other games. … Similarly, it may well be far more useful and satisfactory for us to ask ‘When is therapy?’ rather than ‘What is therapy?’. For in doing so we can then begin to focus on the contextual features of therapy rather than continue with our vain attempts to eke out their definitional properties” [pp42-44]
So, might it be more helpful to query ‘When is dignity?’ rather than ‘What is dignity?’? When is dignity maintained for this person, now? When are the ‘signs’ of dignity visible (such as being treated equitably, feeling safe and respected, being able to have a ‘voice’ and be heard and exercise choice as far as it is possible, in whatever way you can communicate – embodying the ‘autonomy’ that contemporary ideas of dignity seem to hold key)? In other words, what are the ‘contextual features’? If we know when this person’s dignity is maintained we can therefore know how to recognise environments and situations when their dignity is disrespected, attacked, ignored, humiliated – and perhaps our focus should be on what those contexts are for each individual person.
It is hard to accept that Lucy’s ‘dignity’ is maintained when there are increasing incidents of distress and communications through behaviour that, for her, are indications of lack of comfort or a sense of safety (e.g. smearing faeces). If we think about Maslow’s theory of the hierarchy of our needs, we heard that in recent times, Lucy often stopped eating and drinking, her sleep was affected, and she could become dehydrated. These aspects of her experience are the most basic of needs in the hierarchy – perhaps when dignity is maintained for any of us, the foundations of our needs must come first, and arguably before any externally imposed definition of what living as an ‘adult’ entails.
The SCIE website further talks about the role of relationships in dignity in care:
“Surveys involving people who receive or provide social care frequently emphasise relationships above all: between the person needing care and their carer, within groups in residential care, and between the people receiving care and the wider community.”
Relationships and their vital importance to our healthy functioning as humans (our dignity?) are conspicuously absent in the quickly accessible literature I have found on the subject. The ideas seem to centre on autonomy, independence and self-determination. All well and good – yet we know that these aspects of our being are only possible within relationships (see, for example, Why Love Matters by Sue Gerhardt) that foster our basic needs and allow us to move up the pyramid to these more lofty ideals.
From the information at the hearing, as well as their idea of what defines ‘dignity’ as an adult, the Local Authority’s position seemed to focus on Lucy’s physical and rehabilitation needs to inform their view on a best interests’ environment. Whilst these things are, of course, important, there seemed a similar lack of weight given to her relationships, and how important they might be for her sense of safety, as foundational to facilitate engagement with physical interventions to assist daily living, let alone further rehabilitation of her injuries. In Maslow’s hierarchy, a sense of safety could be seen to be a prerequisite for Lucy to be able to engage with rehabilitation. Dignity could be seen in the psychological safety of her environment.
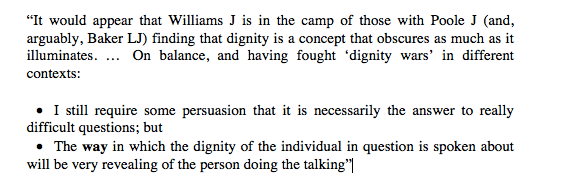
Alex Ruck Keene, barrister with expertise in the law and mental capacity, has recently blogged about the use of the concept of dignity in law:
I think I would agree with this, and further argue that an objective definition of dignity is not actually possible. As I said, I am not a philosopher, or lawyer, and have just been thinking more about this concept for this blog and for what it means in my work with older people – and I have come to an (interim) conclusion that ‘dignity’ has the potential to be such a catch-all, that everyone and anyone could invoke it to support any position, meaning (as Alex Ruck Keene notes) the concept ‘obscures as much as it illuminates’.
Claire Martin is Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a member of the Core Group of the Open Justice Court of Protection Project and has published many blog posts about hearings she’s observed (e.g. here and here). She tweets @DocCMartin
[1] With thanks to Professor Louise Amoore (@AmooreLouise), Professor of Political Geography, Department of Geography, Durham University, for comments on an earlier version of this blog post.
Two relative novices to the Court of Protection had their first experience of a hearing before Mr Justice Hayden on 20thMay 2021. They record their impressions here.
I also observed this hearing (COP 1275114): a s.21A challenge on behalf of a man in his 40s with “learning disability at the most severe end of the spectrum“, autism, and epilepsy.
It was an unusual case for a Tier 3 judge but had apparently been transferred by District Judge Eldergill because P’s mother was also his Deputy and, at some point, was refusing to accept that his placement met the best interests requirement for a Standard Authorisation. This meant that the authorisation conflicted with other existing authority for P, meaning that the ‘no refusals’ requirement was not met. This raised the question of what happens when you get a refusal from a Deputy when there’s no immediately available option – which was the legal issue warranting a Tier 3. That refusal is, however, “historic”, and the case is now, according to counsel, “a simple s.21A challenge, albeit with complicated facts”. On that basis Mr Justice Hayden disengaged from the “interesting academic question”, saying that the Court has “no time to satisfy people’s intellectual curiosity” about issues that are not of direct and immediate relevance.
My understanding is that there was an agreed order but that Mr Justice Hayden called the case in nonetheless because (in his words): “I do not on my inevitably superficial reading of the papers get a sense of a man who is being afforded the opportunity to develop his potential, whatever that might be.” The evidence from an expert witness (described by the judge as “cogent, detailed and long”) suggests that P’s current care home “is not properly attuned to, or educated in, the kind of care than will enable P to achieve of his best – or, never mind achieve anything, but be happy and enjoy life more”.
All parties seem now to accept that P’s current placement is not in his best interests, and – pending a move – there is some concern to improve life for him where he lives now. Hayden J’s focus in this hearing was on practical issues like provision of “Now and Next” cards to support P’s transition between activities, and investigation of the possibilities of enabling him to take part in more of the activities he enjoys: cycling, swimming and hydrotherapy, in addition to his current use of the gym.
P’s mother, present in court, has some concerns about sporting activities because she worries that her son’s epileptic seizures make them unsafe. Hayden J asked for a neurologist report as soon as possible, said that P should not be deprived of activities that might benefit him and added a personal note: “I’m not really much of a gym person myself, Mrs X, but I do like to get out on my bike and I suspect P might like – not quite the freedom of the open road, but getting out in the fresh air.”
I’ve watched Mr Justice Hayden in more than 30 hearings – amounting to well over 100 hours. For Emma Heron (research nurse and LLM student) and for Olwen Cockell (speech and language therapist and Registered Intermediary), this was their first exposure to him. Here’s how they found the experience.
Emma Heron: Learning to Wait
When I woke up this morning, the last thing I had on my mind was observing a Court of Protection hearing but as I logged into twitter to see my messages a post caught my eye:
Actually, I did have the time (unusually!) and I’d been hoping to observe a case for months. Maybe this would be the opportunity. I hastily copied down the email address and the case reference and sent my request to the court.
I waited and waited but got no reply – until eventually I contacted Celia who suggested emailing the Royal Courts of Justice again with the judge’s name in the subject line and the word “URGENT”. Still no reply with 15 minutes to go before the hearing, so she emailed the judge’s clerk for me and also tweeted to alert Her Majesty’s Courts and Tribunal Service (@HMCTSgovuk) that there was a problem for me of gaining access. All was well in the end – I was sent the link in time and I was able to observe.
Excitement turned to anticipation which turned to a minor panic. The seriousness of the situation suddenly hit me and once I was in the virtual court room I had a hundred questions. What if I pressed the wrong button? Was I doing the right thing and would someone tell me if I wasn’t? Was I going to be found to be in contempt of court if my microphone suddenly defied the laws of normality and came on in the middle of the hearing? Fortunately, there was a delay, as the judge was still involved in a different case. A wait and a breather were just what I needed to gather my thoughts and think about what I was hoping to get out of the hearing.
Of course, originally, I’d hoped to observe a hearing before I’d written my assignment for the last module I had done, which covered mental health law. Well, that boat had sailed. But this was a perfect opportunity to listen in and embed the knowledge from my module, seeing the practical application in “real life” as it were. I wanted to look at the attendee list to see how many people were on the call, but I kept my fingers to myself and listened patiently, waiting for the judge to arrive. There was still a little residual concern I’d press the wrong button! I’d assumed the hearing would start on time but it was about 45 minutes before the judge arrived. I’d say if you are thinking of attending, do prepare for this as a possibility (and it also means the hearing finishes later than you’d expect).
We got started. I whispered (yes, the microphone was on mute but I figured you can’t be too careful!) to ask my husband to make me a cuppa having heard him put the kettle on.
There were several reminders from the lawyers that there were members of the public present. I felt this was really good as I think it might have made sure things were explained a bit better – and there was a helpful summary at the beginning to provide some context setting for the observers.
The first thing that struck me as I listened to the summary of what had happened so far was the length of time it had taken to get to this point. The time it had taken for various services not do have done things. And, most importantly the time the person at the centre of the case was having to wait to have the issue resolved. I experienced several emotions during the first half hour. Frustration, amazement, and yes just a little bit of anger. It all just seemed to have been stretched over such a long period of time. As the judge said at one point, “I find myself wondering what has been going on in this case for so long to achieve relatively little”.
I was judging. Oh yes, indeed I was. I had so many things whirring around my head, questions I wanted to ask, objections I wanted to make. Worried that the judge might miss something, that he would fail to fully understand a certain perspective that I could see as a health care professional. What if he couldn’t? It was hard. And – I was not the judge!
Just as well really. I need not have worried. As the hearing unfolded, I was struck by the calm, unhurried pace and attitude of the judge. Nothing was going to slip him by. He was not going to make any sort of judgement until he was ready and he knew exactly what he would need in order to be ready. He had a methodical system of listening, summing up, questioning and clarifying. There was one point in the case where he wanted a piece of information, prompted by a comment that had been made by one of the participants. Various answers were given, offers of what he could have but he knew what he wanted and persisted. There was no fobbing off, no letting things slip, no lapses in attention. Every single comment and insight seemed carefully added to the story that was unfolding and he was in control of it all. All of my worries I’d had about things being missed, things not being seen fell away. This was an expert at work and it was really a privilege to see. He was able to grasp the “zoomed out” view without losing sight of the key issues and without a hint of disrespect.
It struck me as I carried on listening that although my head had been full of thoughts and judgements, his most certainly wasn’t. Not at that stage, anyway. And this is perhaps the most important thing I took away from the session. He is a judge. And yet he was not quick to pass judgment. He knew when that time would come and he wasn’t going to go anywhere near that territory until that time was there. What a lesson to learn.
Unfortunately I had to leave the session before the end – note to self the timings are approximate! – but it was an experience I feel honoured to have had and I am sure one that will be repeated again one day.
Thank you to the Open Justice Court of Protection Project for enabling me to grasp this opportunity through sharing the knowledge and providing guidance every step of the way!
Olwen Cockell – Building a holistic profile
The hearing commenced with the court clerk reminding all parties about the various regulations about confidentiality and Mr Justice Hayden then welcomed all parties.
Mr Justice Hayden did request advocates to give a little background but this was really brief and I actually gleaned more of a sense of the purpose of the hearing from the various exchanges that went between the legal representatives before the hearing officially started.
Legal representatives had actually referred to P by his first name in their informal communications in the virtual waiting room, but I noted that they changed to use of initials when Mr Justice Hayden opened the hearing. I liked it that Mr Justice Hayden asked for P’s proper name to be used as I felt this personalised the case.
From piecing together various snippets of information given about P, I learnt that he is a man in his 40s with considerable difficulties in cognition and communication associated with a primary diagnosis of autism. He is non-verbal and he relies on routine/structure/predictability so that he can function day to day. His mother talked about how his behaviour was calmer and more manageable when he lived at home (for the first 36 years of his life) and benefitted from the very tight routine he was afforded there. For example, she described how when he had a bath, she always washed him in the same order: first his hair, then his face, then his shoulders – and the same thing when drying him. She said this kind of routine really helps him. “I tried to tell the care home this, and they didn’t pay attention to me”, she said – adding that she’s pleased that the need for routine is emphasised in the expert report.
Unfortunately, it seems that P’s residential facility is not offering the level of routine and structure that P needs nor is he being offered opportunities for sensory stimulation that he craves. This has led to his mother to be very concerned about the level of care P has been receiving at his care facility. The independent expert assessment has made a number of recommendations for how P’s needs may be met going forwards. Some of the recommendations could be very easily implemented (e.g. use of a visual timetable); others such as swimming and hydrotherapy may prove more challenging to deliver. Mr Justice Hayden also emphasised the importance of obtaining an up to date objective assessment of P’s medical/physical health to ensure that these activities would be safe for him – recognising his mother’s concerns about his safety but saying “I don’t want to have to rely on Mum because she’s Mum – which is a tribute, not a criticism“.
The hearing also touched upon P’s best interests in terms of his long-term accommodation needs (domiciliary vs residential) but Mr Justice Hayden felt P’s interests would be best served in the short term by a care plan being expedited within the residential care setting.
Mr Justice Hayden showed great humility, taking time to listen and talk to P’s mother, who clearly knows and loves her son very much, so that he could get a fuller sense of P as a person. He also was very keen to have sight of objective expert reports about P so that a comprehensive, holistic profile could be built up.
Through the course of the hearing, Mr Justice Hayden gave all participants sufficient opportunities to contribute, emphasising the importance of positively moving forwards. He closed off one line of argument with the comment: “We’re now unlocking past pain to some degree which probably is no longer productive”.
I left the hearing feeling that Mr Justice Hayden had developed a sense of who P is and that his management of the hearing was laying the necessary groundwork so that all parties can start working towards an agreed plan that will meet P’s best interests.
Emma Heron is a research nurse, currently working in South Wales and an LLM student at Cardiff University. She blogs at www.receivingconsent.com and she tweets @nyrs_emma
Olwen Cockell is a dual-qualified speech and language therapist and primary school teacher. Olwen is based in Kent and has supported children with language and learning for over 20 years. Since 2015 Olwen has worked as a Registered Intermediary and assists children with speech, language and communication needs when communicating evidence to police and to the courts. She tweets @olwenc
Editorial Update: The judgment has now been published – click here.
On 14th May 2021, BBC News and two national newspapers ran a story about a Court of Protection hearing concerning a 21-year-old woman with agoraphobia who is pregnant and wants to give birth at home. There is no published judgment available yet so these media reports are the only publicly available sources of information. I was not able to observe this hearing in court since (unusually) the public were refused permission to attend via video-link – this is itself a cause for concern which I discuss at the end of this blog.
All three headlines draw attention to the judge’s decision that she can be “forced” into hospital against her wishes. According to the Guardian, “Justice Holman concluded that it would be in the 21-year-old’s best interests to allow staff trained in restraint techniques to use minimum force if the woman refused to leave home.”
As far as I can tell from the media reports, which are short on detail, the Trust responsible for her care made an application to the Court of Protection for (1) a declaration that the woman lacks capacity to make this decision for herself, and (2) that it’s in her best interests to give birth in hospital. Apparently, her partner and family agree with the Trust.
The woman’s lack of capacity to make her own decision about place of birth is attributed (by BBC News and the Guardian) to her agoraphobia: “Justice Holman concluded that the woman’s agoraphobia meant that she did not have the mental capacity to make decisions about the birth of her baby”. The Guardian reports that she is “overwhelmed” by her agoraphobia and the BBC report says she “has an “overwhelming” fear of leaving her home”.
The Independentdoes not use the word “capacity” or indicate that any decision has been made in relation to the woman’s ability to make her own choices but simply discusses her best interests.
All three reports start with the judge’s claims about what is in the woman’s “best interests”. This is addressed prior to – or, in the case of the Independent, without – any statements about capacity, And none of them provides any evidence at all as to why the judge (or anyone else) thinks it’s in her best interests to give birth in hospital.
This naturally leads readers who understand the Mental Capacity Act 2005, and especially those who work with birthing women, to feel concerned.
Agoraphobia, as evidenced by “an overwhelming fear of leaving her home”, is surely rather a good reason for choosing to birth at home, rather than hospital. Home is a place in which she feels safe and secure.
There is no account of any particular medical condition that makes home birth inadvisable for this woman, nor any description of contra-indications for home birth (e.g. this NHS website advises against home birth as unsafe “if you’re expecting twins or if your baby is lying feet first (breech)” but there’s no indication that either is the case here.) The same website also states that for a first baby, there is a very small increased risk of negative outcomes (from 5 in 1000 for a hospital birth to 9 in 1000 for home birth) and that “if you’re having your second baby, a planned home birth is as safe as having your baby in hospital or a midwife-led unit”.
So, it’s really not clear why the judge is quoted as saying there was a risk that something could go wrong if the woman gave birth at home, and that this could result in “catastrophe” – a word used in all three articles. This same quotation is also used across all three sources:
“I think you should go to hospital and have this baby,” Justice Holman told her. “It will avoid potential risks and disaster if something goes wrong.”
This is baffling. It may be that journalists have somehow omitted to report salient health considerations that would militate against home birth – but in the absence of any such information, the judge comes across as simply ill-informed about home birth and as perpetuating a medicalised model of childbirth at the expense of women-centred care.
The media reports indicate that this woman’s legal representative (the Official Solicitor) did not challenge the finding that she lacked the mental capacity to make a decision about where to give birth, but did disagree with the use of force to compel P to go to hospital in a non-emergency situation.
“Lawyers representing hospital bosses responsible for her care had said the use of force should be approved. But lawyers representing the woman had disagreed, and said she should be allowed to give birth at home if she would not leave and could not be persuaded to leave, unless an emergency arose.” (Guardian).
Although this woman is willing it seems (from the BBC report) to go into hospital in an emergency (“She wants a home birth – unless there is an emergency”), the judgment is that force may be used to compel her to go into hospital “if she refused to leave home on a specified day near her due date” – so in advance of any potential emergency.
So, this woman seems to have agreed in principle to go into hospital if there is an emergency during her labour, but wants to start labour at home and see how it goes. But the judge has ordered – contrary to submissions from the woman’s lawyer, the Official Solicitor – that she must go into hospital a few days before her due date – i.e. prior to any emergency situation. If she does not agree to do this, and cannot be “persuaded”, he has authorised “some trained force and restraint” (Guardian) if needed, describing this scenario as “unattractive”, but her best interests.
Judges in the Court of Protection usually give a great deal of weight to the position taken by the Official Solicitor as to what is in the person’s best interests. It seems that on this occasion the judge approved a forcible transfer to hospital contrary to the opinion of the Official Solicitor as to what is in this woman’s best interests. The fact that the Official Solicitor’s position was not the one accepted by the judge does suggest to me that it is not unreasonable to have concerns about this judgment – as I do, and as do many members of the public (with the proviso, of course, that the details available to us are limited).
Public response to media reports
Overwhelmingly the public response to media reports of this judgment has been anger, fear and distress.
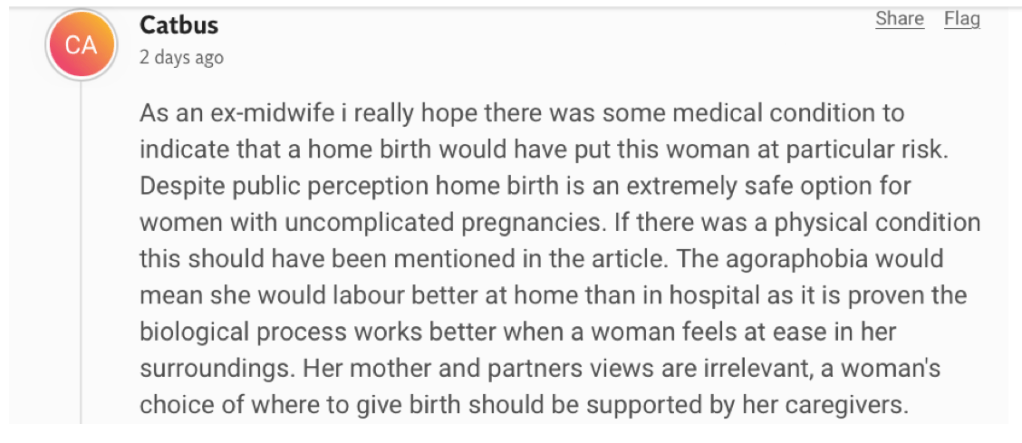
This comment from a former midwife appears below the line in the Independent, (which also features comments characterising the judgment as “medieval”, and as “violating her rights” – as well as an explicit comparison with the patriarchal dystopian world of Margaret Atwood’s Handmaid’s Tale in which women are subjugated vessels for the production of babies).
Across social media, many people working in health and social care – including childbirth educators and activists, midwives, doctors and doulas – have expressed dismay at the judgment using words like “terrifying”, “draconian”, “outrageous” and “horrific”. “Disgusting”, said one, “patriarchy and sexism in full flood”, wrote another.
Feminist psychologist, Jessica Taylor tweeted:
Childbirth activist Michelle Quashie tweets:
Also in a tweet, obstetrician, Susan Bewley described the judgment as “a shocking abuse of human rights”. And Kathryn Gutteridge, a Consultant Psychotherapist supporting women surviving sexual abuse and childbirth, said that the judgment as reported in the media “smacks of ill-informed people using the law to get what they want. As a clinician I would never want to use this sledgehammer to care for a woman”. Another health care professional tweeted:
“I find it hard to understand which staff exactly are going to be expected to lay hands on this woman and force her to do something that she doesn’t want to do. I’m waiting to see the COP report, but as a MH nurse, given what I’ve read, I would not be willing.”
According to the Birth Trauma Association:
Rob Buist, a specialist obstetrician and gynaecologist with a particular interest and extensive experience in the management of complicated pregnancies tweets:
People with agoraphobia have also expressed concern. (These tweets are used with the authors’ express written permission):
What’s the evidence that she doesn’t have capacity to make her own decision?
Capacity is a particular concern for some people who asked whether in fact -and if so on what basis – it was found that the woman lacked capacity to make her own decisions about where to give birth. This was not entirely clear from the media reports – and of course simply having a diagnosis of ‘agoraphobia’ (or any other disturbance in the functioning of the mind or brain) is not in and of itself sufficient for determining that a person lacks capacity to make a decision. The Mental Capacity Act 2005 requires a presumption that a person does have capacity to make their own decisions (s.1(2)), and claims that they do not must show that they cannot understand, retain, weigh or communicate information relevant to the decision that needs to be made (s.3). No such information was given in the press. As these two health professionals correctly say, agoraphobia is not itself evidence of lack of mental capacity
The following exchange is between a Court of Protection lawyer and a medical ethicist – who also raises the key questions he would want to see addressed.
Why is forced removal from her home and hospital birth in her best interests?
Even accepting she lacks capacity to make her own decision about her birth, it was radically unclear from the media reports why being forced into hospital was in her best interests. It was generally assumed that there must be compelling medical contra-indications for home birth – although none are mentioned. “I assume there is something medical we’re not being told” tweets a student midwife. “Is this a high-risk pregnancy with a high risk of birth complications?”, asks a medical lawyer. “What’s the medical reason why she can’t have a home birth?” tweets someone else. Obstetrican Susan Bewley worries that the judge has simply assumed that home birth is risky.
A failure of open justice
Based on my reading of the news reports, these concerns, challenges and expressions of outrage seem appropriate: there’s no evidence that the woman at the centre of this case lacks the capacity to make her own decisions, and no hint as to why a hospital birth is considered to be in her best interests. It does sound draconian.
My views, and those of other members of the public, might be different if we had more access to information about the case. At least our criticisms and our challenges would be more informed.
I have personally attended 177 hearings in the Court of Protection since the beginning of lockdown (and about two dozen before that). As an academic psychologist I also have some research background in home birth and – full disclosure – I also grew up with a mother who was a powerful advocate for home birth and women’s rights to make their own choices in pregnancy and labour. The issues raised by this case concern me deeply as a feminist and as someone with strong personal commitments to autonomy, especially in relation to medical treatments.
I was not able to attend this hearing – although it was held “in public”. The Royal Courts of Justice provide no information in their listings as to what cases are about, so although I would have chosen to attend this hearing if at all possible, since it relates to key areas I’m interested in, I didn’t know about it until part way through. Then I was told that the judge would not allow public observers to attend via the video-link (only in person). I could not justify a 5-hour journey to London to observe this hearing during a pandemic, even if I’d known about it in advance with time to travel down, which I didn’t. I have attended other so-called “hybrid” hearings via video-link, so I don’t understand why the judge in this case made the decision that observers must attend in person.
I have attended two previous cases concerning court-ordered caesareans and am in contact with childbirth experts based in London who have expressed interest in observing hearings where orders are made concerning women in childbirth. None of them was free at such short notice to attend.
If members of the public had been able to attend, we would have a much better understanding of the facts of the case, and I would understand why the judge made the judgment he did (whether or not I agreed with it).
I have now requested access to the position statements from the parties (these are the skeleton arguments barrister produce in writing before the hearing) and am planning a follow-up blog post when I have more information. I’m told the judgment will be published shortly too and will post a link to it when it appears.
What this experience clearly demonstrates is that it’s not sufficient for open justice to have to rely on reports from journalists. Media accounts are necessarily abbreviated versions of complex decision-making processes. Journalists cannot be expected to engage with these issues in the same way as a consultant obstetrician, a specialist perinatal community mental health midwife, a feminist psychologist, or an expert by experience. There are limits to the extent to which a journalist can act as the “eyes and ears of the public”.
Open justice means supporting access to the courts for members of the public too. When health and social care professionals, activists, and ‘experts by experience’ are also able to attend court hearings, the quality of the reports they produce (as evidenced by those in our blog) is often detailed, sophisticated, thoughtful and knowledgeable. By observing hearings, instead of simply reading about them in the press, people with passionate commitments to particular issues can come to appreciate the care and attention with which the Court of Protection normally proceeds, the moral dilemmas and challenges it faces, and the balancing exercises it engages in. Tweet threads about hearings have engagement indexes in excess of 3000 people; our most popular blog posts have between 4000 and 5000 reads: there is clear interest in understanding more about these hearings than is conveyed in mass media publications like those discussed here.
And whether members of the public agree or disagree with a judgment, the opportunity to develop our understanding of the way in which the decision has been reached, moment by moment, as evidence is heard, and lawyers present positions, and judges interrogate them, is an essential component of ‘open justice’ in a democratic society.
Celia Kitzinger is co-founder (with Gill Loomes-Quinn) of the Open Justice Court of the Protection Project. She tweets @kitzingercelia
We’re delighted to bring on board two new members to join the core group of the Open Justice Court of Protection Project – Claire Martin (left photo) and Kirsty Stuart (right photo). Both have already provided key inputs into the Project and are keen to continue. They will help to shape the development of the Project over the coming months. Welcome both of you!
Claire Martin is a clinical psychologist who has spent her career working with older people in the NHS. She currently leads the older people’s psychology team in Gateshead. Principally, she considers herself a jobbing clinician, and, in addition to being a clinical psychologist and a member of both the Faculties for the Psychology of Older People and Neuropsychology of the British Psychological Society, she is trained in psychological therapies of Cognitive Analytic Therapy and EMDR (Eye Movement Desensitisation and Reprocessing). She is a keen advocate for older people being able to access the same psychological support and therapies as younger people. Working with people who are in distress and finding ways to help make sense of their experiences and to address, manage or come to terms with things has been the mainstay of her working life. Most recently, she has developed an interest in the impact of psychological trauma in later life.
Part of working as a psychologist in older people’s mental health services involves providing opinions and assessments when a person’s mental capacity to make decisions about their life is in question. Day-to-day she sees first-hand the interwoven intricacies of people’s history, relationships and long lives that have an impact on the way they navigate their later years, their wishes and values. Thinking about recording one’s wishes in Advance Decisions can be part of this work and so a broad understanding of the Mental Capacity Act 2005 is needed to be a psychologist working with older people. She has always chosen to work in older people’s services because of the variety of experiences that older people bring with them and the rich complexity of working with people who have lived long lives – as well as a belief that our society does not treat older people well and that their own voices and value are often side-lined. In the end, it is just so interesting and rewarding working with older people, being alongside as an ally and champion at times that can be so difficult.
The Open Justice Court of Protection project caught her eye during the COVID pandemic as an opportunity to get involved in learning more about our justice system and mental capacity – especially as a lot of Court of Protection cases involve the rights, care and wishes of older people when they have lost capacity to make certain decisions for themselves. So, a ‘bit of CPD’ became a regular drive to observe, learn about the application of the law and then, bit by bit, join in with the wider conversation around the complex issues involved. A broad understanding of the MCA 2005 is just that – it leaves a lot to learn. So, she’s found the experience of attending hearings, and seeing the compassion and real attention to ‘P’s’ own values in life, a huge education. Being part of a growing and stimulating network of interested and engaged people who want to observe, understand and challenge their own and others’ thinking has been a ray of sunshine in an otherwise bleak and devastating year – so being able to be part of the core team and continue that conversation is exciting and a privilege.
Kirsty Stuart is an Associate Solicitor at Irwin Mitchell Solicitors. She has worked within the Court of Protection sphere for more than 5 years and represents those who are the subject of proceedings as well as family members on a regular basis. She represents in a range of matters from deputyship to capacity and best interest disputes to serious medical treatment cases. Alongside this, Kirsty also advises on community care matters and human rights act claims as well as cases in the Inherent Jurisdiction of the High Court.
Prior to working at Irwin Mitchell solicitors, Kirsty worked for several years as a Mental Health Solicitor and so uses her cross working knowledge and leads in her firm on matters for autistic people and/or those with learning disabilities detained in Assessment and Treatment Units. Kirsty has a passion for disability rights and exploring new ways of ensuring the rights of those detained in hospital are upheld and will regularly use Makaton with clients and is developing ways to ensure that the client is always at the centre of the cases and able to actively participate.
Kirsty is an active member of a campaign group called #right2home which campaigns and advocates for homes not hospitals for those who are autistic and/or have a learning disability. Through this, Kirsty has co-authored the #right2home leave guidance for those in in-patient settings, care homes and independent supported living placements as a reaction to the pandemic and regularly holds webinars and events to help empower parent carers and advocates to support those in these units as well as leading on campaign days in respect of raising awareness of human rights for those in Assessment and Treatment Units.
Kirsty has developed a network for lawyers with additional caring responsibilities. As a parent of two children with additional needs and a carer for her mum with a rare type of young onset dementia, she has first-hand experience of the pressures of balancing work and home life. Kirsty started a network for others to get together virtually and share experiences. The aim is to share experiences and understanding but also to highlight the positives and unique skill set that people like herself can bring to our clients such as using Makaton or an understanding of syndromes, rare genetic conditions and the battles that clients face.
On the morning of Tuesday 13th April 2021, we both logged on to MS Teams to observe a hearing before District Judge Ellington (COP 13715986). The listing information on the First Avenue House website – which helpfully provides advance information about the issues to be addressed in court – informed us that the case concerned s.21A of the Mental Capacity Act 2005. Such cases are quite common in the Court of Protection and we have blogged about them before (e.g. here): they are effectively reviews of whether someone is lawfully deprived of their liberty.
The person at the centre of this case is an 84-year-old man, “DM”. He joined the hearing from a hospital psychiatric ward. He has had a successful career as a journalist, to which he often refers (he’s very proud of his journalist granddaughter who has “followed in my footsteps“). Although he is now divorced, his wife and daughter are “closely involved and loving towards DM and supportive” according to the judge (although neither was in court). He has diagnoses of vascular dementia and hypomania – diagnoses, said DJ Ellington, tactfully, that DM “may disagree with”. Until recently he has lived on his own in sheltered accommodation and he wants to return home.
As DJ Ellington set out in her opening summary, DM has been living in a hospital psychiatric ward for the last six months. He was admitted under s.2 of the Mental Health Act 1983 following a deterioration in his mental health, then subsequently detained under s.3 for treatment, and then (since early February 2021) under a standard DOLS authorisation. He is not allowed to leave the ward on his own, and is only allowed to go out with care staff. The ward doors are always locked, and he’s subject to continuous control and supervision. He’s been ready for discharge for more than two months, but there is disagreement about where he should go.
The local authority contends that there is reason to believe that DM lacks capacity to make his own decisions about care and residence, so that the court should make decisions on DM’s behalf. They believe it is in his best interests to move into a residential care setting. They say he hoards at his home, gets lost when in the community, is unsafe in traffic, and has difficulty looking after himself. At a best interests meeting in February 2021, they decided that it was too much of a risk for DM to return to his sheltered housing. DM’s ex-wife and daughter are also concerned that he’ll be unable to cope if he returns to his sheltered accommodation.
DM disagrees. He does not accept that he has any mental health problems. When it was explained to him that professionals were concerned about his “getting lost”, he said, “That is completely fallacious. Sometimes my purpose is questionable, but not my intelligence behind it.”
DJ Ellington clarified from the start of the hearing that the question of where DM will live “will not be decided today” but will be deferred to another hearing in a few weeks’ time.
DM was represented by Nick O’Brien (via his litigation friend, the Official Solicitor). The local authority was represented by Thomas Jones.
Meeting DM
DM joined the hearing slightly late. From the outset he appeared very engaged with the proceedings and asked for the names and roles of all the people he could see on screen. For one of us (Evie), encountering the protected party in person in the (virtual) court was a new experience.
Evie Robson
DM was actually present in the courtroom. I could put a face to the name of a person whose personality and charisma would otherwise have been lost. From the very start, he demonstrated an avid interest in the court proceedings, clarifying the names and positions of all those with their videos turned on.
As the lawyers discussed the possibility of a move to a care home (pseudonymised here as “Elm House”), DM became increasingly agitated. He interrupted the proceedings and brought out a document he had written earlier, although it turned out that he couldn’t actually read it with his current spectacles (“I’m a two-pair-of-glasses man I’m afraid”) so he quoted snippets from memory. He was clearly quite distressed by the idea that he could possibly be sent to live in a place where he really does not want to be.
DM knew quite a bit about Elm House, having researched it on the internet and it was obvious that he resisted any suggestion that he should move there. He felt it would be degrading, and from his descriptions I could not disagree. It was quite unexpected and very moving to listen to him:
“I don’t want to go to Elm House. There is rubbish on the front drive. The hedges are not cut. It’s a tiny little room. I would be kept there until I rotted away.”
He continued in a confident outpouring of emotion which I found quite heart-breaking. Never before had I heard the thoughts and opinions of a protected party in the Court of Protection so clearly as I heard them then. He told the court “I want to fulfil the things I have not completed”, specifying “I have a wonderful novel to write”. His belief in fruitful years to come was clear when he said “I’m only 80. I have 20 years of life to live. I am going to live to 100”. He asserted “I will go into the accommodation that suits me,” adding: “Even to suggest that I should be deprived of my freedom any more and put into isolation, that really did scare me”.
However, confident as DM sounded about his plans for the future, it seemed to me that his views were slanted. Before he began his impromptu speech he said “Under Section 3, I have more rights than any other person would have, and none of the restrictions apply” – in a manner not at all spiteful but instead almost desperate. I got the impression that he did not want to be grouped together with people he perceives to lack the capacity he believes himself to have.
Whether or not he has capacity to make his own decisions about where he lives and the care he receives is not the thing that most interests me (although obviously that is important to the court process). Rather it is the power he had to command the attention of the courtroom to ensure we all heard the story completely from his perspective. Without DM’s presence in court, and the sudden passionate expression of his views, I would not have felt such strong compassion for him. His presence, articulacy and vivacity made him so much more human in a place where it easy to become just a name or some initials.
Obviously not all protected parties wish – or are able – to appear in the online courtroom, but what stood out for me here was the need to properly hear their voices and opinions and to accord them respect. DM is a man who previously exercised authority in the world. He had a successful professional career and made significant decisions in the course of it. And now other people are treating him as someone without capacity to make basic decisions about his own life. It is easy to see how he must feel vulnerable, powerless and humiliated.
Later in the hearing, DJ Ellington – who had talked with DM before the court hearing started – reported that he’d said “if you treat someone like an idiot, they will become an idiot”. That strikes me as very poignant.
Whether or not DM has the capacity to decide where he lives, he clearly has enough understanding to realise the position he has been placed in. He is, as Nick O’Brien said, “acutely aware that he has been deprived of his liberty”.
Celia Kitzinger – DM at a previous hearing before DDJ Allen
During the course of the course of the interactions Evie has described, I realised that I’d met DM before, in a telephone hearing on 24th February 2021 before Deputy District Judge Allen. In that hearing he was ebullient.
He was insistent on knowing the names and roles of all the participants in the hearing and was unfailingly courteous and complimentary towards them.
There seemed to be some persistent hearing difficulties. Several interactions ran off like this:
Various non-sequiturs were also possibly occasioned by hearing difficulties:
In the earlier hearing I watched, DM was quick to intervene when his barrister (Alison Easton) addressed the court to argue for detailed investigation of the options of returning home and of extra care accommodation (as well as the preferred option of residential care promoted by the local authority):
“I would like to congratulate that last lady speaker. What a fantastic presentation. That’s a very clear plan – the clearest I’ve ever heard put forward. I am capable of living on my own and feeding myself and going out on my own. I have a penchant nowadays for calling taxis even if it does cost a few bob. As for my appearance and dress, I can do a quick change in about ten minutes if I have to. If I’m not to go home, I’d be quite happy with the extra care accommodation at [Place] if you require it. I’m not incontinent. I don’t need spoon feeding or assistance in the bathroom. […] I would love to get back into the community. I’m not going to do a runner. We all have our little faults. I hope mine will be overlooked.”
Later he helpfully suggested to the judge that she should read about “the Bournewood Agreement” which he’d researched on the internet (perhaps here) – explaining “he was deprived of his liberty but he proved his detractors wrong and moved back into the community. That’s what inspired me in this case”.
At (what DM took to be) the end of the hearing he said:
“Thank you very much to all parties here today. You’ve done a great job. You’ve shown some flexibility. I’d like to commend [the extra care accommodation] which has a very good view over [open countryside]. I look forward to the result.”
The poignancy comes from seeing DM, who had once possessed power and authority in a successful professional career, who had “travelled the world” (he mentioned South Korea and Cuba) as part of his work, pleading for his liberty. Now, others make decisions on his behalf and he clearly feels himself diminished by this. “I’m compos mentis, 100%,” he said.
Amongst the older people I know, some adapt to changed life circumstances and cede power and control to others graciously, and can even be relieved to have the responsibilities of choice lifted from their shoulders. For others, autonomy and independence are core to who they are as people – central to their sense of their own dignity as human beings. I hear in what DM says a complex mix of bravado and ingratiation, as he tries to demonstrate his own capacity and assert some control over his future in the face of his “detractors”.
It’s the fundamental problem at the heart of so much of the work of the Court of Protection. How do you keep someone safe if the very requirements for doing so constitute a fundamental assault on their sense of themselves as human beings? As Mr Justice Munby famously said:
“… we must avoid the temptation always to put the physical health and safety of the elderly and the vulnerable before everything else. Often it will be appropriate to do so, but not always. Physical health and safety can sometimes be bought at too high a price in happiness and emotional welfare. The emphasis must be on sensible risk appraisal, not striving to avoid all risk, whatever the price, but instead seeking a proper balance and being willing to tolerate manageable or acceptable risks as the price appropriately to be paid in order to achieve some other good – in particular to achieve the vital good of the elderly or vulnerable person’s happiness. What good is it making someone safer if it merely makes them miserable?” (para. 120, Re MM (an adult) [2007] EWHC 2003 (Fam))
What next?
From my (Celia’s) perspective as observer, there didn’t seem to have been as much progress between the two hearings – 7 weeks apart – as I would have hoped and expected. Nick O’Brien seemed to hold the Trust partly accountable for this since they have “not been cooperative with the provision of disclosure” (which I think means they hadn’t supplied the court with DM’s medical records) and there had also been a problem with obtaining evidence about DM’s capacity to make his own decisions (via a s.49 report).
There is still no certainty about whether or not DM has capacity to make his own decisions about residence and care, nor any agreement about what kind of accommodation and care package is in DM’s best interests in the event that he does not.
Capacity
It was said that DM has “quite an unusual presentation”: he’s “complex” with a “spikey range of ability”. On capacity, there is, says Nick O’Brien, counsel for DM (via the Official Solicitor)
“…an issue as to whether DM lacks capacity to make the relevant decisions about his residence and care or whether some of his choices reflect hypomania and are better characterised as unwise decision making caused not by an inability to weigh up and use information but rather by not attributing the weight to risk factors and consequences which others would prefer.”
He gave an example of the way in which DM is “a lot less risk-averse” than the local authority – in other words, he may perfectly well understand and accept the risks, but consider it worth accepting them as the price of his freedom: “he says he won’t get lost going out into the community, and – if need be – he’ll just get a taxi home”. (The judge added that DM had also agreed to wear a security pendant.)
On behalf of DM, Nick O’Brien submitted that a report was required under s.49 of the Mental Capacity Act 2005 as to DM’s capacity to make his own decisions about where he lives and what care he receives, but he had been told that these reports were taking “at least three months”.
This has prompted those instructing me to start making enquiries of independent psychiatrists who might work on swifter timescales. We have a number of enquiries still outstanding this morning. The court effectively has two choices: either accept the delay of 3 months – which is effectively an invitation not to be asked to provide a report at all, or insist that they provide one sooner. Three months is simply unacceptable when they have a clinical relationship with DM already, but the Official Solicitor’s position is that we will probably need an independent expert.
Best Interests
In the view of the local authority, a move to Elm House – a residential care home – is in DM’s best interests. Having read the Official Solicitor’s position statement before the hearing, the local authority mooted – as a sort of ‘compromise’ solution – that DM could be moved to Elm House but with a special bolt-on package of “community access” arrangements set up with an outside care agency, amounting to 7 hours per week. This would enable, they said, “a hybrid model of community life and residential care”.
This was clearly a frustrating position from the Official Solicitor’s point of view.
We’ve been provided with a balance sheet analysis that identifies four residential care homes amongst its options, none of which is the option that is being proposed by the local authority today. And none of the four have we had the chance to investigate – let alone provide DM with the chance to look at them. He’s not had the opportunity to look at any of the four options. We have a question about what DM’s life would be like if he moved to a residential care home. One of the clear features of this case is DM’s enthusiasm for being active and out and about. One of the reasons he’s not keen on Elm House is its location. He’s familiar with that area of London and his understanding of the distance from the care home to shops and so on is right. He has plenty of skills in self-care over and above just getting washed and dressed in the morning. He can make himself a snack, breakfast, a cup of tea. Elm House does not allow residents to do this for health and safety reasons. The result would be a de-skilling – and a denial of DM’s opportunity to take part in the sorts of activities that can be important in combatting dementia. […]. We cannot be satisfied that a move to Elm House is in DM’s best interests. My client is acutely conscious of the fact that he’s been deprived of his liberty and doesn’t want to continue to be at the hospital, but the alternatives are not clear.
The Official Solicitor also made the argument – pretty much the same argument made at the hearing seven weeks earlier – that there had been no adequate exploration of the possibility of DM returning home: “there simply isn’t a plan set out as to how care would be delivered if he returned home. That cannot be excluded at the moment. It hasn’t been investigated.”
The case is supposed to be back in court on 12th May 2021. We hope there is progress and that DM will be able to move to somewhere he can be happy.
Meanwhile, DM waits, deprived of his liberty on a locked ward. By the time of the next hearing (if it happens as planned), he will have been ready for discharge for more than three months.
Evie Robson is a Year 12 student studying English Literature, French, Maths and Further Maths at Whitley Bay High School. She has contributed several other blogs to the Project (e.g. here). She tweets @evie275
Celia Kitzinger is co-director (with Gill Loomes-Quinn) of the Open Justice Court of Protection Project. She tweets @kitzingercelia
Editorial Note: We have published two previous blog posts about a covid vaccination case here and here. The judgment has now been published on BAILII – click here.
In the hearing I observed before Mr Justice Hayden (case number COP 13498835, on 30th April 2021), a decision was made that it was NOT in the person’s best interests to receive the Covid 19 vaccination. All previous judgments seem to have been in favour of vaccination, so this is a significant decision.
Part of my professional role as Deprivation of Liberty Safeguards and AMHP Manager for a local authority involves supporting others to understand and apply the Mental Capacity Act 2005 and I was involved last year in writing guidance for our local care homes on making best interests decisions in relation to the Covid-19 vaccination, so I felt very fortunate to be able to observe this hearing.
It’s rare to have any information about what a Court of Protection hearing is going to be about until the hearing actually starts, and although all of those I’ve observed have been very professionally helpful, this one was of course particularly relevant to me. As I’m not one of the people on the ground having to grapple with best interest decision making about Covid-19 vaccination for particular individuals, it was fascinating to observe this hearing and watch the way in which Mr Justice Hayden considered all the factors in this complex case.
A key aspect of this case is that (unlike – as far as I am aware – all previous cases), the judge had to make a decision in the context of significant opposition from the person themselves (not just their relatives).
Previous published best interest decisions
There have been several published judgments regarding whether or not it’s in a person’s best interests to receive a vaccination for Covid-19.
The three most widely known are two before the Vice-President of the Court of Protection, Mr Justice Hayden: E(Vaccine) [2021] EWCOP 7 and SD v Royal Borough of Kensington and Chelsea (2021 EWCOP 14. and a third before Mr Justice Butler Re C [2021] EWCOP 19. In all three cases, the person concerned was living in a care home, lacked the relevant decision-making capacity, and it was family members – rather than P themselves – who opposed vaccination. The judgement in each case was that it was in the person’s best interests to be vaccinated[1].
In his conclusion in the ‘SD’ judgment, Mr Justice Hayden states:
What it is important to emphasise here, as in so many areas of the work of the Court of Protection, is that respect for and promotion of P’s autonomy and an objective evaluation of P’s best interests will most effectively inform the ultimate decision. It is P’s voice that requires to be heard and which should never be conflated or confused with the voices of others, including family members however unimpeachable their motivations or however eloquently their own objections are advanced. (para 33, SD v Royal Borough of Kensington and Chelsea (2021 EWCOP 14)
The person at the centre of this case
The person at the centre of this case, SS, has advanced dementia and (since 2019) has been living in a large care home of currently 79 residents. She is subject to a Standard Authorisation under the Deprivation of Liberty Safeguards (DoLS) and is appealing this via s.21A proceedings. The issue of vaccination arose in the course of these proceedings as a discreet issue and it is only this issue which was before the court today.
When the GP visited the care home, SS declined the Covid-19 vaccination and has done so repeatedly. SS’s resistance to vaccinations appears to be longstanding, with 4 recorded occasions when she has explicitly refused the flu vaccination since 2010 (and no record of her ever having received it).
SS never married, does not have children, and other than someone who appears to be a cousin, ‘T’, she has no friends or family left to support her.
In her mind, SS has reverted to life in the late 1940’s, when she was living with her parents and working as a secretary in the Lyons cake factory. At 4pm every afternoon during her working life, a loud horn sounded for workers to exit the building. And now at 4pm every day, SS puts on her coat, picks up her handbag and announces she is done for the day and is off home, where her mother will have her tea waiting for her.
In the opening summary, SS was described as a lady who does not appear to need a great deal of support: she is “feistily independent”, “extremely stubborn” and someone who could become very “fixed in her ideas”.
It appears that SS read a newspaper article which she interpreted as saying most medical treatment and/or vaccinations were likely to be injurious rather than beneficial and from that point on has resolved not to cooperate with any medical treatment at all, to the extent of becoming physically aggressive when a doctor tried to examine a rash on her leg. On another occasion she told carers she had “wiped the smile off the face” of a psychiatrist who tried to speak with her.
She has consistently resisted offers of the Covid-19 vaccination and has been assessed by her GP as lacking capacity in respect of this decision, on the basis that she cannot retain the relevant information and struggles to weigh it.
Best interests, vaccination and restraint
At the beginning of the hearing, counsel took different positions as to whether or not it would be in SS’s best interests to be vaccinated.
SS’s own representative, Rebecca Hancock, said she was seeking the court’s guidance and had no definitive position.
Amelia Walker representing the CCG said that it is in the best interests of everyone, and in particular residents of care homes, to have the vaccine and that this would also apply to SS. She also reported that administering the vaccine would likely be straightforward and the GP could be assisted by two community mental health trust nurses trained to provide physical restraint. She said, “the GP’s view is that physical restraint wouldn’t be necessary – but that they could provide ‘light touch support’.” Mr Justice Hayden asked, “is that a euphemism for gentle restraint?” and added, “I don’t understand the GP saying restraint wouldn’t be needed because last time she was all for giving someone a kicking.” (In fact, it later turned out that the GP report said that restraint would be needed.)
Tony Harrop-Griffiths, representing the Local Authority, said it was a “difficult balance” but that he thought it was NOT in her best interests to have the vaccine.
There was very little known about SS’s life story and her views when she had capacity, so Mr Justice Hayden sought what information he could – including consideration of the views of SS’s parents as an indication of how she was brought up. A statement by her cousin T, told us that SS’s father was a man of medicine and would very much have encouraged her to take the vaccine, but her mother was a spiritualist and held beliefs outside those that are considered normative.
Mr Justice Hayden was keen to hear from those who knew SS now, and so (at short notice!) the team leader for the unit SS lives in and the care home manager came on the video platform for 40 minutes. In Hayden J’s words they “brought her character, personality and temperament” into his court room and “hugely impressed” him with their “compassion and care”.
The team leader talked with fondness about SS being “a very private lady”, “very independent”, “very strong willed”, and “pleasant on a one-to-one basis but someone who struggles to be on good relations with other residents”. She won’t allow staff to support her (“I don’t need help. I’m not stupid. Leave me alone.”) and doesn’t like to be touched at all (“she finds that very off-putting”). Refusal of medication for her blood pressure and cholesterol some years previously, led to attempts to covertly administer these to her in her tea, but these attempts were thwarted by her keen sense of suspicion!
Mr Justice Hayden explained he’s been asked to consider the option of a GP and two mental health nurses providing ‘light touch support’ to administer the vaccine, to which the manager replied “I hope they know kung foo!”, adding, “there will be no light touch about it, she’ll require full restraint to administer the vaccine, and it will be a difficult situation”.
Mr Justice Hayden explained to the staff he was “trying to balance risk of death against trying to protect her dignity, autonomy, who she is, her pride. She’s in a vulnerable group. That’s the dilemma the court’s being presented with”.
It had also been suggested by an independent expert that SS might be given a sedative such as lorazepam: while this wouldn’t remove the need for physical restraint, it would significantly weaken her resistance. Yet it was unclear how this could be administered given it would arouse immediate suspicion if attempts to covertly administer were made. Staff described SS as “like a sniffer dog” and as she prepares her own tea or juice, if she were given a cup of tea – she would know there was something wrong.
Care staff had initially felt SS would need to go to the GP surgery for the vaccination, but given that she is someone who never leaves the care home and becomes “overwhelmed” if she goes past the care home’s reception area when taking a walk, it was acknowledged that trying to get her into an ambulance would be distressing, both for SS and the other residents living on the unit. There was a suggestion of vaccinating her either in her bedroom or in the office where she speaks with her solicitor and Relevant Person’s Representative. Care staff however did not wish to be present, fearing erosion of the trust carefully built up between SS and some of the staff. One said, “I don’t think it would be right for me to be in the room when she’s vaccinated. She would look to me for help and I wouldn’t be able to help her.”
Final submissions
The judge gave everyone a short break to reflect on what they had heard and then they returned for closing submissions.
Having heard the evidence, Rebecca Hancock now believed that although it’s an extremely delicate balance in this case, it’s not in SS’s best interests to have the vaccination. She said that S has very few relationships of trust, but has a relationship with some staff which would be put at risk by vaccination against her wishes.
Amelia Walker, counsel for the CCG remained of the view that it was in SS’s best interests to have the vaccination – although the argument put forward was from a ‘general view’ on the basis that it’s in the best interests of everyone to have the vaccine and particularly those who are vulnerable and in care homes. She was swiftly reminded by Mr Justice Hayden that you need to look at the individual’s particular circumstances: “That’s not to engage with the relevant law. You look at the individual – not just the medical but right across the full scope of her interests and welfare”. Amelia Walker also suggested that if SS is not vaccinated she may find her activities restricted, e.g. not being able to go on trips (but, said the judge, she doesn’t anyway!).
Tony Harrop-Griffiths maintained the same position as he had initially presented; the Local Authority does not believe it is in SS’s best interests to be vaccinated. He now gave four reasons: (1) because physical restraint would be required (even if sedation was also used) and that would lead to a breakdown of trust; (2) because there is already a history of lack of engagement with medical professionals, so evidence that she has a long-standing objection to medical intervention; (3) bearing in mind the wider picture that there is a s.21A challenge in progress, another (smaller) care home has been located, and they are willing to accept her unvaccinated, so that potential move is not a reason to advocate vaccination; and (4) since SS does not engage in community activities or leave the care home, that too is not a reason to advocate for vaccination.
Judgment
In considering the factors in this case, Mr Justice Hayden spoke of how there is little doubt that if S were to be infected, she at very high risk or serious illness or death.
Although all but one of the care home residents have already been vaccinated, more than 20 of the care home staff have declined vaccination – most of those because they “object in principle to doing so”. Mr Justice Hayden said, “That is their right. But with rights of course go responsibilities. They go into the home every day. They carry risk of infection.”
The care home staff “do not need to be told how awful this insidious virus is” because they “have seen it at first hand” during the first wave of the pandemic when 27 of their residents died.
He said, “there is no doubt at all that it is in SS’s clinical best interests to receive the vaccine.”
But “analysis of best interests requires scrutiny of welfare in the widest sense not merely medical but psychological and emotional”. He quoted Baroness Hale in Aintree:
The most that can be said, therefore, is that in considering the best interests of this particular patient at this particular time, decision-makers must look at his welfare in the widest sense, not just medical but social and psychological; they must consider the nature of the medical treatment in question, what it involves and its prospects of success; they must consider what the outcome of that treatment for the patient is likely to be; they must try and put themselves in the place of the individual patient and ask what his attitude to the treatment is or would be likely to be; and they must consult others who are looking after him or interested in his welfare, in particular for their view of what his attitude would be. (para. 39 in Aintree University Hospitals NHS Foundation Trust v James)
Hayden J noted how “SS expresses strong opinions regarding medical treatment but specifically to the vaccination” and “her compromised capacity does not mean her strongly expressed wishes are rendered nugatory” (of no value or importance). “If she were capacitious and refusing this vaccination that would be the end of it, as it is for the carers in the home who decide not to have it.”
Given SS’s strong opposition to vaccination, treating her would involve restraint – either with or without sedation.
“I am not at all attracted to the restraint simpliciter or sedative restraint option. SS has very few effective interpersonal connections with the outside world. She has no doubt for her own survival had to forge some level of trust for those who care for her. This is so intrinsic to her wellbeing that to my mind it requires to be protected vigilantly. She would resist, I have no doubt, any restraint – and it would create a traumatic and disturbing scenario, for her, for the carers and the other residents”. (Hayden J)
He concluded:
“Right at front of this case and in this care home, is the scarring of loss of lives and painful deaths. The real determination is to protect SS from that. But though much of her cognitive function may have gone, her autonomy – and her own sense of it – not merely continues but flourishes, and she guards it carefully. Ultimately in my judgement, it is that which requires to be respected and is ultimately determinative of this issue[…]. So for all these reasons, it is ultimately my clear conclusion that it is not in SS’s best interests for her to receive the vaccine.”
Reflections
This is the first judgment I am aware of where the person themselves (rather than their family, on their behalf) was refusing the vaccination and in this case, clearly quite strongly.
Although I know the potential consequence for SS of contracting Covid-19 might result in the end of her life, for me, the thought of this lady being physically restrained in order to administer a vaccination that she so very clearly did not want, was just terrible. It would have surely damaged her fragile relationship with care staff irreconcilably, not just in her current care home but going forward to the new home if she moves there.
It was also really difficult for me to justify vaccinating SS against her wishes, when the care staff and relatives visiting the home – who will be the ones likely to bring the virus in – retain the ability to choose whether or not to accept it themselves.
I really wasn’t sure which decision Mr Justice Hayden was going to make as I sat through the hearing. Details of all possible options were closely examined, especially the option of using a sedative which was discussed in some depth, so I was really quite relieved when he delivered the judgment and I absolutely agree with his decision and with the reasoning behind it.
I think the most important learning for me from being able to observe this hearing, is the way it has again, allowed me to watch the Mental Capacity Act 2005 ‘in action’ and understand how a senior High Court Judge, in this case the Vice President of the Court of Protection, works through the process of reaching a best interests decision.
I’m also able to take away with me some ideas that I can incorporate into my own practice when completing best interests assessments myself in future. For example, in this case, as there was no information about SS’s past wishes, feelings, beliefs and values from when she had capacity, Mr Justice Hayden considered what SS’s parents’ views might have been as an indication of how she was brought up and therefore what factors might influence her decision. While I know my own views of the world are very different from those of my parents, in the absence of any other information I can now see how this might be helpful in some situations.
This hearing also allowed me to observe playing out in action, how respect for and promotion of S’s autonomy and an objective evaluation of her best interests informed Mr Justice Hayden’s decision. Personally, I would have loved to have seen SS express her views to Mr Justice Hayden in person and I don’t know whether she was invited to attend, or even aware that the hearing was taking place. But even without her physical presence, I do feel SS’s voice was most certainly heard and her wishes and feelings – which were articulated so clearly by the care home staff who knew her – were clearly of central importance in Mr Justice Hayden’s decision.
In my experience, there continues to be a great deal of misunderstanding of the Mental Capacity Act 2005 within both health and social care, even though the Act has been in force since 2007. This is why remote access to these Court of Protection hearings is so very important and why I’ve been a supporter of the Open Justice Court of Protection Project. It really does such wonderful and important work in continuing to educate us all. I would encourage anyone reading this blog who has not yet taken up this unique opportunity to observe a Court of Protection hearing, to please try to make time for this while hearings are still available to view on line!
Astral Heaven is the Deprivation of Liberty Safeguards and AMHP Manager for a Local Authority. She tweets @AstiHeaven
[1] To learn more about these cases (and the broader legal framework for best interests decision-making about vaccination), you can listen to a 30-minute podcast on “Vaccine hesitancy and the Court of Protection: Who decides?”, in which Rosalind English interviews Amelia Walker (who represented the CCG in this case).
My OJCOP colleague, Celia Kitzinger, and our regular contributor, Claire Martin recently observed a challenging case before the Court of Protection concerning ‘ZA’ – a woman with Schizophrenia and diabetes. Proceedings followed an application by the NHS Trust from which ZA has been receiving treatment for severe infections and other complications arising from her diabetes, to determine whether ZA lacks the capacity to decide whether or not to consent to the amputation of a leg, a treatment proposed by her treating clinicians; and, in the event she is deemed to lack capacity, whether amputation would be in her best interests. You can read in detail the facts of the case, and observations and commentary on it in Celia and Claire’s blog here. I did not observe the proceedings, but in this short piece I wish to share my response to the case (as I understand it), and my perspective on ZA’s position.
As a disabled person who has been a fulltime wheelchair user for the last four years, since the age of 33, and whose life has been changed almost beyond recognition as a consequence of the progressive impact of my multiple impairments, ZA’s apparent position – that she doesn’t “want to be in a wheelchair” as she’s “not that person” spoke to me and touched more than a few nerves.
Why is this a best interests decision at all?
My first reaction to the case is one of anger and frustration that ZA has come to find herself in a position where a fundamental decision about her health and her future has been taken out of her hands and made by a judge in consultation with medical professionals.
ZA has a history of Schizophrenia and associated fluctuating capacity, and the impact of her diabetes on her leg did not occur overnight. Indeed, it seems that ZA has repeatedly voiced her wish not to have her leg amputated over a period of years – both as a refusal of consent (when capacitous) and as an expression of values, wishes, feelings, and beliefs (when apparently lacking capacity). I am given to understand that ZA experiences ‘flattened affect’ as part of her Schizophrenia, which may be expected to dampen her response to her circumstances, but her views seem consistently held and expressed, Why, oh why then, did no one involved in her treatment suggest she set out her refusal in an Advance Decision to Refuse Treatment (ADRT), especially given her Schizophrenia? This would have enabled a disabled woman to ensure that her ‘voice’ would continue to be heard and respected in the event that she was deemed to lack capacity at the material time that a decision needed to be made about her leg. I find the fact that this opportunity was clearly not made available to her unsurprising but tragic. (I have written here about my own research on ADRT and disability, and discuss this in an interview with barrister, Alex Ruck-Keene here).
Becoming ‘that person’ (following a best interests decision)
Now that the decision is a ‘best interests’ one, I hope in the strongest terms that ZA’s wishes are upheld. I say this firstly because my general world view and personal ‘hierarchy of values’ places a strong emphasis on personal autonomy and the rights of individuals to make their own choices concerning their bodies and their lives – a position rooted without doubt in my experiences as a person disabled from birth. But I have a more practical, pragmatic reason for taking this view.
Having been disabled since birth, I have been a fulltime wheelchair user for about the last 4 years (since I was 33), and my life has been completely transformed by the impact of the progression of my impairments. I know that there is a general tendency (among both abled and some disabled people) to talk about “getting used to” and “accepting” acquired impairments, or the progression of congenital ones – and there is obviously a body of sociological literature on these phenomena. But my ‘real life’ experience is that these processes are hugely complicated – with ups and downs and lots of complex, conflicted feelings and responses. And, more relevant to ZA’s case (with the amputation ZA’s life expectancy is 5-10 years) these processes of adjustment take time.
Unlike ZA, I have always been relatively positive about my chair, and I haven’t ever seen myself as “confined” to it, or “bound” by it, or “defined” by it. I’ve even written poetry about how it changed my life for the better: life in our society as a wheelchair user can be tough, but life without one when one has chronic pain, fatigue, and mobility limitations can be totally, utterly unbearable. But even so, I have sometimes HATED my body as it is now. Sometimes I still do. It’s like being stuck in a rusty cage. And the thing about hating your body is that there is no escape. You cannot go anywhere to snap out of it and distract yourself. And along with this, learning how to accept and work with support is a process too. I know I have struggled – sometimes less than graciously – and sometimes I have been quite difficult to help as a result.
Given the reactions of abled people to my experiences, I sense that many people don’t really understand these processes of adjustment, or perhaps much about living a disabled life in our society more generally – the time it takes to access support and get things right. The endless bureaucracy, and the energy it takes to do the ‘job’ of being disabled. What happens when vital equipment breaks. How much of our physical world remains totally inaccessible if you get around on wheels rather than feet – how much you lose as a result, and how much you grieve. Four years into this process – as a relatively positive wheelie – and I’d say I am just about getting my head around what it means to be this person and to be living this life, a life I certainly did not expect to be living. And this remains very definitely a work in progress with ‘good days’ and ‘bad days’. Remember that ZA is expected to live 5-10 years following amputation.
So how would it be to have these experiences, and these feelings ‘forced’ on me as a consequence of a best interests decision? I obviously cannot (and would not wish to) speak for ZA. But for me it would be torturous. I cannot imagine the impact on my mental health, and how this would affect how I would engage with those around me and those supporting me. I have a strong desire later in my career to undertake longitudinal research around the consequences of best interests decisions, and this sort of situation highlights precisely why. For me, navigating this life that I did not expect to be living is an ongoing challenge – and one that seems surprising to many abled people in my life. I cannot imagine how it would feel to have got here via a best interests decision that did not reflect my expressed wishes.
I would hope that if a best interests decision is made on ZA’s behalf, it reflects her wishes. I would also hope that it takes into account the ‘voices’ of disabled people and organisations in situations more analogous to ZA’s to add an accurate representation of ‘adjustment’ and ‘acceptance’ to the ‘balance sheet’ of a best interests decision.
Gill Loomes-Quinn is co-director (with Celia Kitzinger) of the Open Justice Court of Protection Project. She tweets @GillLoomesQuinn
The person at the centre of this case (COP 13718293) is a 53-year-old woman we can refer to as ZA. She has been in hospital for the last 25 weeks with a chronic non-healing diabetic ulceration on her right foot and bone infection (osteomyelitis). There is no medical dispute but that, from a purely surgical perspective, amputation is the right thing to do.
ZA is adamant she doesn’t want amputation of her leg. She told the agent instructed by the Official Solicitor: “if I die, I die. We all die sometime”. When talking about people who have only one leg, she said, “I don’t want to be like that” and visibly shuddered. If her leg was amputated against her will that would be (she said) “horrible” and she would be “angry and distressed”. She repeatedly says that she wants to leave hospital and go home.
Without amputation she’s likely to die within 6-12 months, but would be able to return home to her husband and adult son – although there is some concern about “revolving door” or “cyclical” readmissions to hospital with sepsis and complications, which is what has been happening recently (11 hospital admissions since 2016). She’s not in any pain because she has diabetic neuropathy (loss of sensation in her feet), and she is able to move around – albeit with difficulty and contrary to medical advice – using her stump and holding on to furniture. She is refusing a wheelchair.
With amputation she could live 5-10 years or more (depending on her level of compliance with diabetic medications, which is variable) and she’d need a lot more support with activities of daily living. It’s not certain she’d be able to return home after surgery, since this would depend on the level of care that she’d need. She might have to go to supported living. It’s unclear whether or to what extent she’d be able and willing to use a wheelchair. Her current view is: “I don’t want to be in a wheelchair. I’m not that person.”
If ZA has the mental capacity to make her own decision about amputation then the court cannot decide on her behalf: she would be free to make her own choice in accordance with the well-established principle of self-determination. Competent adults have the right to refuse medical treatment – for good reasons, bad reasons, or no reasons at all – even if that refusal will obviously be followed by their death.
There is a presumption of capacity in law (s. 1(2) MCA) and this is especially important for people, like ZA, who have impairments in the functioning of their mind or brain. ZA has chronic schizophrenia, cognitive impairment secondary to her schizophrenia, and (due to her infection) delirium. But mental impairments and mental incapacity are not synonymous – as famously demonstrated in the classic case of Re C [1994] 1 All ER 819, a 68-year-old man with chronic paranoid schizophrenia who developed gangrene in his leg and was found to have capacity to make the decision to refuse treatment.
Some previous assessments, dating back to 2019, did find that ZA had capacity to make her own decision – and it was because she has been deemed capacitous to refuse amputation (and did refuse) that surgery has not been done before now.
So, the question before the court was first whether there was sufficient evidence to displace the presumption that ZA has capacity to make her own decision about amputation, and second (if she is deemed to lack capacity) whether or not amputation is in ZA’s best interests.
The application was brought by the Trust – with Helen Mulholland as counsel – who sought a declaration that ZA lacks capacity to make her own decision about amputation, and that amputation is in her best interests.
ZA’s family (her husband and son) are not parties to the case but have been fully consulted (and her son was present in court throughout). They had initially opposed amputation, at a best interests meeting in late 2019. They are still very concerned about the impact of forcing her to have amputation against her will and worried about the sense of “betrayal” she might feel, but they do now support the Trust’s application.
Emma Sutton acted for ZA as litigation friend (via the Official Solicitor). Her position at the beginning of the hearing was that “the Official Solicitor is unable at this stage to agree with the application before the court and will consider her position following the oral evidence”.
The hearing
We didn’t meet ZA or her family in court. The hearing began an hour after the listed time because the judge spoke with ZA before members of the public were admitted. We were also excluded from court for some time after the lunch break until ZA’s husband and son had given their evidence, since they had asked to do so in private.
The hearing took place over two days (22nd and 23rd April 2021) before Mr Justice Cohen. As members of the public, we heard evidence from five doctors: (a) the treating diabetologist (b) the consultant surgeon who would actually carry out the amputation if it was authorised by the court (c) Mr Scurr, a consultant surgeon acting as expert witness (d) Dr Rebecca O’Donovan, a psychiatrist acting as expert witness and (e) the treating psychiatrist. (The Transparency Order permits naming of the independent experts but we cannot use the names of the treating clinicians.) The advocates summarised the family’s evidence in their closing submissions. What follows is not a complete report of what everyone said, but rather what struck us as salient or interesting. (Text is by Celia except for the section about Dr Rebecca O’Donovan, which Claire wrote.) Witnesses addressed questions about capacity and about best interests, as well as technical medical issues we have largely omitted here (e.g. why above-knee rather than below-knee amputation).
(a) Treating diabetologist
He described his involvement with ZA over time and was clearly concerned to convey that he did not think she had the mental capacity to make her own decision about amputation. In one conversation with her, he said, “I explained that without surgery she would die and she told me clearly that she did not want to die. She looked up at me and made eye contact and stated, ‘I don’t want to die’”[1].
This exchange took place under cross-examination from Emma Sutton:
(b) Consultant surgeon
Despite the Trust’s view that amputation was in ZA’s best interests, not all of the individual clinicians in the Trust were of this view. The surgeon who would actually carry out the amputation did not, in fact, agree. “The quality of life is not one she’d want,” he said. “She could go on for any number of years, and whether she would thank us for that I don’t know. In his view, sending her home with an advance care plan (to prevent ‘revolving door’ readmissions for future sepsis) would be preferable.
He was, however, willing to carry out surgery if the court made a best interests decision that it should be done, and “technically it’s not a difficult issue at all to remove the leg”. There was some concern about restraint in order to get her into theatre at which point this witness, rather alarmingly, said that he would not plan to tell ZA in advance that she was going to have her leg amputated.
The surgeon also, said, on several occasions, that he didn’t feel ZA had any “joy” in her life – and he also worried about the burden for her family.
(c) Mr Scurr, expert witness, consultant surgeon
This expert witness was also an expert witness in an earlier amputation case – Wye Valley NHS Trust v Mr B [2015] EWCOP 60. In that case, Mr Justice Peter Jackson decided that it was unlawful to amputate Mr B’s leg in the face of his (non-capacitous) opposition to amputation – despite the fact that Mr Scurr said that Mr B would be likely to die within a few days without amputation. It was pointed out to him by one of the lawyers in this hearing: “You expected him to succumb within a week without amputation and I think he lived 18 months.” Mr Scurr explained that this was because, in Mr B’s case, he had made his diagnosis based only on the medical records. He had, however, examined ZA and so was more confident in his view that her life expectancy without amputation would be no more than a year, with the proviso that “if she got a serious infection that didn’t respond to antibiotics she could be dead within days”.
“There is no prospect of the ulcer healing – ever. It’s difficult to manage. It smells. It will get infected and will eventually cause systemic infection. So clinically amputation is the right thing to do.”
He was clear, however, that although amputation was “clinically … the right thing to do”, this was not the same as a best interests decision for ZA. “Surgery should not simply prolong life, it should enhance it”. A best interests decision needs to take into account the person’s own wishes. “When I went to see her,” he said, “she was quite lucid. She knew where she was and what was happening, and she knew she didn’t want an amputation.”
Mr Scurr answered some questions from the judge related to the problem of “revolving door” admissions to hospital if the decision was made to allow ZA to return home without an amputation. He said: “it would be wrong to take her to intensive care – it’s a terrible place to be. She’s made the decision not to go down that route. We have patients when they’ve had enough, they’ve had enough”. He suggested there should be no active treatment. “When she starts to go downhill, encourage her to stay at home or move to a hospice until she dies.”
“We are now in a situation where we can prolong life almost indefinitely. The question must be asked: is this the right thing to do? At the end of the day, we have a responsibility to the patients – to be kind to them, and to take into account their feelings and their relatives’ feelings.”
At the end of his evidence. he said to the judge, “I’m sorry to leave you with such a problem.” The judge replied, “That’s very kind of you, thank you. It’s my job”.
(d) Rebecca O’Donovan, expert witness, psychiatrist. By Claire Martin
I attended only Day 2 of the hearing (23 April 2021) ) and was able to observe witness statements from Dr O’Donovan, forensic psychiatrist and expert witness, as well as the treating psychiatrist for ZA.
Dr O’Donovan was an expert witness for the Official Solicitor and she centred her evidence on the past, current and potential future mental health of ZA. It was clear, as noted, that ZA has experienced, over many years since a teenager, varying levels of mental ill-health and hadn’t functioned independently for, I think, at least fifteen years (we were told about episodes of significant distress since 2008).
Turning her attention to the possibility of amputation, Dr O’Donovan said she was “concerned about gaps in the care plan”. She was referring to the treating team’s plan for the process of informing and discussing with ZA that the amputation would go ahead (if this were to be the judgment), and the possibility of restraint and how this would be managed. She expressed a concern about cardio-pulmonary arrest being a risk if restraint was not handled correctly: “It would need a lot of thinking about: who? How? How will hands be put on? Graded stages”
She also talked about the potential impact on ZA, were she to feel that her family had ‘colluded’ with the plan against her wishes. Her family are her closest relationships.
However, Dr O’Donovan also expressed a view, perhaps not dissimilar to ZA’s treating surgeon’s, that, if the judge authorised amputation, then not a ‘huge’ amount of discussion ‘would be best’, because “telling her long in advance could cause distress”. Dr O’Donovan had clearly looked meticulously at ZA’s historical mental health records (such as Mental Health Act detentions) and was able to draw on those to hypothesise about ZA’s likely reaction to being subjected to treatment that she did not want.
Dr O’Donovan was very clear that ZA, over the years, has stated clearly (including when deemed to have capacity for this decision) that she did not want to have an amputation of the leg. She explained that, although ZA has cognitive impairment secondary to her diagnosis of schizophrenia, she would clearly “know that her leg is missing and the emotional and psychological impact of that should not be underestimated”. She offered a counter-view that, “due to the negative symptoms of schizophrenia … she has blunted affect … schizophrenia might protect her [from emotional distress] to some degree”. She based this latter view on the fact that, when ZA had had some toes removed, she ‘settled quickly’ despite having been very clear that she did not want them removed. The judge seemed not wholly convinced:
“We are talking about something that is so different. Her toes are one thing – how can we say that, because she wasn’t so distressed after her toes, she would not be distressed by [the removal of] her leg.”
Dr O’Donovan’s response rested on what she described as ‘significant negative symptoms of schizophrenia’ including marked lack of motivation and apathy. I wondered about this – ZA has experienced this mental health condition for a long time, though has currently been in hospital for 8 months and has a delirium. I was not sure how she was functioning in terms of her engagement with the world over the past several years, but I found myself thinking that her current inpatient hospital experience could account for, or at least contribute to, her negative symptoms, as much as her mental health diagnosis.
When discussing ZA’s understanding of death – in relation to her capacity to understand and weigh up the decision about amputation – Dr O’Donovan said:
“She does have some insight into death. For me, she’s talked about seeing people with one leg and wouldn’t want to live with that. She can’t provide depth though – what would be good or bad about that. Does she connect to the finality of death? The impact on relationships? I don’t get the sense that she’s thought this through and worked through those endings. Her capacity to do that is very limited.”
It suddenly struck me that ZA, who is currently in hospital with a delirium and infected bones of her foot, is, seemingly, being held to a much higher bar than the rest of us would be (when our capacity is not in question) in terms of needing to demonstrate an understanding of what death means to her. This feels worrying to me – at a time when we are least likely to be able to demonstrate (our previous, capacitously held, wishes) that we can understand, retain, weigh up and communicate a decision about self-determination, we need to be more able to do so. It does seem to be a huge missed opportunity that, over the years, clinicians have not discussed an ADRT with ZA when she has been assessed as capacitous to refuse amputation.
Dr O’Donovan also talked in depth about potential risk of depression and suicidality, should the amputation go ahead against ZA’s wishes – and described a situation where, should this come to pass, ZA would ‘not be able to act on them’. Counsel for ZA, Emma Sutton incisively noted: “Having suicidal thoughts and not being able to act on them – that could be very hard for her”.
This was discussed further in relation to ZA needing to use a wheelchair after an amputation and how she might feel about that and adjust to it. Dr O’Donovan explained that ZA would find it very hard to learn how to operate a wheelchair – she described ZA’s results on the Addenbrooke’s Cognitive Examination (a cognitive screening tool developed principally for use in the differential diagnosis of dementia) as being ‘poor’ for visuo-spatial functioning. Over the course of her evidence Dr O’Donovan referred to ZA’s cognitive function as ‘declining for many, many years’. Helen Mulholland asked Dr O’Donovan if she had looked at cognitive assessments from before. I got a bit lost here. Dr O’Donovan reverted to discussing ZA’s negative symptoms of schizophrenia, rather than cognition per se (although of course, at any one assessment, they will be interlinked).
ZA had a MMSE (Mini-Mental State Examination) in 2011 and got a score of 22/30 suggestive of ‘mild cognitive impairment’. Scores below 25 do suggest possible cognitive impairment, and warrant further examination. MMSE is a widely used, very short, screening test (it is used less often now since it has become copyrighted). In a meta-analysis of its utility in 2009, here, the authors concluded: “Provisionally, the MMSE had very limitedvalue in making a diagnosis of MCI [Mild Cognitive Impairment] against healthy controls.”
It’s a blunt instrument, and can be helpful in providing a pointer to the need for further, detailed neuropsychological testing and clarification of cognitive abilities over time. I am not sure whether ZA has had more extensive neuropsychological assessment over the years. It is likely that she will have repeated MMSE and/or Addenbrooke’s assessments. Even though we did not have reports of more extensive testing, the expert witness and the treating clinician both stated that ZA’s cognition had declined over the past decade or so.
Dr O’Donovan completed the Addenbrooke’s assessment with her this year, though we did not hear about the overall results. That test in itself is a screening test, covering domains of attention, orientation, memory, language, visual perceptual and visuospatial skills. She indicated that ZA did not do well on the test – though she also has a delirium which will mean that it is not possible to accurately assess her ‘true’ cognitive abilities , as her treating psychiatrist later stated in her testimony:
“I am not able to say how much delirium is contributing to her cognitive impairment and to what extent cognitive impairment is reversible. Following each episode of delirium, there can be long-term consequences for cognition. This episode is long. It is difficult to accurately assess [ZA’s] understanding and cognition …. If the delirium could be reversed then we could assess the long-term consequences of the delirium on her cognition.”
So, it’s a complex picture in terms of ZA’s ‘true’ cognitive status – but it is certain that delirium makes it impossible to accurately assess right now. ZA’s treating clinician was clear that, should the delirium clear, ZA’s cognition could improve. However, the medical view seemed to be that the only way her delirium would clear would be via amputation.
This is arguably academic though. Over the years ZA has been very clear about her wishes: she does not want her leg amputated. I did feel, at points, that there was a hint of a suggestion that, because someone has a diagnosis of schizophrenia, there is automatically a question mark hanging over whether that person can reasonably hold any view about amputation (and presumably other decisions too)– though this hint would perhaps only be put to the test if that person were to disagree with the clinical team’s view. I might be wrong about this – though as a society, I would argue that we tend to the paternalistic when it comes to self-determined health decisions.
(e) Treating psychiatrist
Given the fact that the Trust surgeon had apparently planned to amputate ZA’s leg without informing her in advance, this was the first issue the treating psychiatrist (who had known ZA since 2018) was asked to address. She said, “To me it feels very inhumane not to tell her that surgery is about to happen. It doesn’t sit comfortably with me as a human being seeing her as another human being.”
Although both the treating psychiatrist and Dr O’Donovan agreed that ZA lacks capacity to make her own decision about amputation, they disagreed about what causes this lack of capacity: for Dr O’Donovan it is the cognitive deficits associated with ZA’s schizophrenia, whereas for the treating psychiatrist it’s the delirium associated with the infection from her leg. Nonetheless, the treating psychiatrist saw ZA as lacking capacity:
“I’m not sure she understands the finality of death. Once you start that conversation about dying, it’s very difficult to explore with her what she thinks and feels about that. But whenever we have conversations about her life and her future there’s no caveat like “I might not be around by then”. For a patient who understands that death is final, you’d expect that to trickle into conversation.”
Asked about whether or not she thought amputation was in ZA’s best interests, she described it as being a decision “on a knife edge”.
(f) Family
Members of the public were excluded from court while ZA’s husband and son gave their evidence (they didn’t want us there), but in their closing submissions the two barristers gave some information about what they had said.
“The family are torn. They would like to prolong P’s life. They would like her to live as long as possible, but they don’t want her to suffer an additional mental health burden and they don’t want her to suffer feelings of betrayal. They are finding it very difficult. But on balance their submission tips in favour of amputation.” (Mulholland, counsel for the Trust)
“ZA’s family have an entirely understandable but irreconcilable wish for her to live as long as possible and for her to be happy. I was struck by the focus from the family on wanting her to be happy.” (Sutton, counsel for ZA via the Official Solicitor).
Emma Sutton also said the Official Solicitor was concerned about ZA feeling “betrayed” by her family who she may see as having colluded with doctors forcing her to have her leg amputated against her will. She pointed out that ZA’s son had raised this concern on a number of occasions.
A best interests decision should have been avoided
By the end of the hearing it seemed fairly clear that the judge will declare that ZA lacks the mental capacity to make this decision for herself. Plenty of evidence was provided by the witnesses to rebut the presumption of capacity – although whether this is caused by delirium or by progressive cognitive deficits is disputed. Intervening into the closing summary from Helen Mulholland as she rehearsed the evidence for ZA’s lack of capacity, the judge said that, having talked to ZA himself and formed a “layman’s opinion” of her capacity in relation to this decision, “I think you’ll find you’re pushing on an open door”.
Although assessments since November 2020 have found ZA to be lacking capacity, her position on amputation remains as clear as it was when she was deemed to have mental capacity to make this decision. If her foot were amputated “then it’s not worth living”. She would “rather die with her foot and dignity than have the amputation”.
So, the decision is a best interests one, meaning that ZA’s views are taken into account but are not (as when she had capacity) determinative.
From my perspective, listening to ZA’s history of engagement with the medical professionals involved in her case, this is quite simply a completely outrageous position for ZA to be in. It could and should have been avoided.
In her closing summary, Emma Sutton said: “It is somewhat regrettable that ZA did not make an advance decision to refuse treatment relating to the amputation If she’d done that, this application would not have been necessary.” I consider “somewhat regrettable” to be an understatement under the circumstances. Doctors have been discussing amputation with ZA for nearly five years and she has repeatedly clearly and consistently refused it. Earlier refusals were made at a time when she was deemed to have the mental capacity to make her own decision: in 2016, again in 2019, and twice in 2020. Given ZA’s diagnosis of schizophrenia, and given its predictable effects on her cognitive capacity in future, combined with the obvious risk of delirium from infection in the future, it must have been apparent to them, with a modicum of thought, that there would come a time when ZA would lose the mental capacity to make her own decision about amputation. This is exactly the sort of situation in which clinicians should be supporting people to make advance decisions to refuse treatment (ss. 24-26 Mental Capacity Act), so that loss of capacity does not reopen the whole question of whether or not treatment should be provided. It is utterly unacceptable to simply wait for a capacitous patient to lose capacity and then to attempt to enforce upon them the very treatment they refused when they had capacity to do so. And although Emma Sutton’s formulation of the problem seems to put the onus on ZA, it is of course the treating clinicians upon whom the responsibility lies. They should have alerted her to the possibility of making a legally binding advance refusal of amputation, and supported her to do so – or ensured that she had access to people who could so support her. (Note: Readers alerted by this blog to the importance of advance decisions refusing treatment for themselves or those they care for can get full and accurate information about how to make these advance refusals from the charity, Compassion in Dying which also provides an online template and a telephone information line.)
Official Solicitor – friend or foe
I’ve been concerned about the role of the Official Solicitor for a long time. It is often the case that the litigation friend (usually the Official Solicitor) appointed to represent the person who lacks capacity argues the opposite of what that person says they want. We’ve published several blog posts based on our observations of cases of this kind – explored most starkly in the story of “Mr G” (here) who wanted to leave the brain injury unit in which he was detained, and return home. He told the court:
“I am incarceratedin a building against my will and which prohibits me having my own volition. The removal of my free will is inequitable, unjustifiable and entirely wrong in my view”
Having been deemed to lack capacity to make his own decision about where to live, the Official Solicitor, purportedly representing him in court, argued that Mr G should not return home – an argument directly contrary to Mr G’s wishes.
It seems to me that vulnerable people are penalised when the Official Solicitor elects not to represent P’s own wishes, but rather takes a position about what P’s best interests are – which may be contrary to P’s wishes. It means that P’s wishes are not fully represented in the way that other people’s views in court are – they are filtered through a ‘best interests’ prism. There is surely a case for advocates to represent P’s wishes as effectively as possible, as would be the right of any other lawyer’s client.
In my academic research with the Coma and Disorders of Consciousness Research Centre, I’ve been horrified by the extent to which the position of the Official Solicitor (at least until very recently) has been to weigh the preservation of life very heavily in the balance against evidence that the person himself or herself would not have wanted to be maintained in their current (or likely future) condition.
“Ordinarily, a lawyer who submitted entirely the opposite of what she knew her client to wish would face, at best, professional sanctions, and at worst, a claim for negligence. In the Court of Protection, however, current practice would tend to suggest that there are circumstances where the lawyer must indeed argue against their client’s wishes. It is ironic and is (or should be) a cause for concern that they are doing so in relation to the most vulnerable of clients, and do so on the basis of instructions given by a person—a ‘litigation friend’—contending that they are acting in the best interests of the individual concerned.” (Ruck-Keene A, Bartlett P, Allen N 2016. Litigation friends or foes: Representation of P before the Court of Protection. Medical Law Review 24(3): 333-359 (open access))
Against this backdrop it was reassuring to see the thorough-going and committed attention paid to ZA’s past and current wishes by Emma Sutton, who had been instructed for ZA via the Official Solicitor, Sarah Castle – who was (she said) “directly involved in this case”.
At the beginning of the hearing the Official Solicitor did not agree with the Trust’s application that amputation was in ZA’s best interests, and wanted to consider her position after hearing the evidence.
At the end of the hearing, in her closing summary, Emma Sutton acknowledged that it was a “finely balanced” decision but came down on the side that amputation was NOT in her best interests – most especially as it went counter not only to her current wishes and feelings, but also to her clearly expressed capacitous decisions as recently as last year. The damaging psychological consequences of treating ZA against her will had been acknowledged by all parties, and could include a painful sense of betrayal and damage to her relationships with her husband and son. It’s also not clear that, after amputation, she could return to the life she had before: she’d be more significantly disabled as an amputee, and may not even be able to return home.
She quoted some of the most powerful statements that judges have made in recent years about the weight to be attached to P’s self-determination and autonomy when set against prolongation of life.
“I have concluded that as I am sure that if Mr Briggs had been sitting in my chair and heard all the evidence and argument he would, in exercise of his right of self-determination, not have consented to further CANH [Clinically Assisted Nutrition and Hydration] treatment that his best interests are promoted by the court not giving that consent on his behalf. This means that the court is doing on behalf of Mr Briggs what he would have wanted and done for himself in what he thought was his own best interests if he was able to do so”. Charles J at para 129-130, Briggs v Briggs & Ors [2016] EWCOP 53
“In a real sense this is not a case about choosing to die, it is about an adult’s capacity to shape and control the end of [their] life. This is an important facet of personal autonomy which requires to be guarded every bit as jealously for the incapacitous as for the capacitous. (Hayden J at para 47, Barnsley Hospital NHS Foundation Trust v MSP [2020] EWCOP 26).
Judgment will be handed down at 3pm on Friday 30th April and we will post a link to it from this blog.
Celia Kitzinger is co-director (with Gill Loomes-Quinn) of the Open Justice Court of Protection Project. She tweets @KitzingerCelia
Claire Martin is Consultant Clinical Psychologist, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Older People’s Clinical Psychology Department, Gateshead. She is a key contributor to the Project and as published many blog posts about hearings she’s observed (e.g. here and here). She tweets @DocCMartin
Note: We’ve previously published a number of blog posts concerning other amputation cases we’ve observed:
[1] These quotations are taken from notes made at the time of the hearing and are as close to what was said as I could make them, given that we are not allowed to record court hearings. They are unlikely to be entirely accurate.
I am a first-year social work student at Bournemouth University. I was lucky enough to hear about the Open Justice Court of Protection Project through one of our lecturers and was immediately intrigued. So, I arranged to observe a hearing as soon as I could.
The hearing I observed was on 20th April 2021 before Mr Justice Hayden at the Royal Courts of Justice via video link (Case Number COP 13663805). I was, unfortunately, only able to attend the first half of the hearing in the morning. but Celia Kitzinger (who attended the whole day) informed me of what happened in the afternoon.
At the beginning of the hearing, there was a summary from one of the barristers, Alexander Campbell (representing the local authority and the clinical commissioning group). He said P is a lady in her early 40s with a number of mental health diagnoses: she has schizoaffective disorder, autism spectrum disorder, moderate learning disabilities and a lengthy mental health history since childhood, compounded by drug use. She also “exhibits sexually disinhibited behaviour”: she has sometimes in the past evaded her carers and sought out casual sexual encounters.
She is currently living in all-female secure accommodation under s. 3 Mental Health Act, but the plan is to discharge her from s. 3 and move her to a supported living placement, which currently has only male residents. This plan was supported by the lawyer acting for P (via the Official Solicitor), Leonie Hirst. The judge was being asked to declare that it was in P’s best interests to move to this new, mixed sex, supported living placement.
He was also being asked to order that P should be given a contraceptive device (also supported by P’s own representative). This was because, due to the medication P is on (sodium valproate – a mood stabiliser), it is vital that she does not fall pregnant: this medication carries a high risk of fetal defects (check out this leaflet). It wasn’t really possible to change her medication because when this had been tried, and she’d been given a different mood stabiliser, she became very unwell.
According to a consultant in sexual and reproductive health who had assessed P and produced a section 49 report, P does not have capacity to consent to contraception or to consent to sex.
A social worker had written a witness statement (and was in court as a witness in the afternoon, which I was sadly not able to attend) saying that the recommended placement was the best of the options available. P would live in a self-contained unit and would not share facilities with any other residents. All the residents at the placement have at least one-to-one care at all times. This means that both P and one of the men would have to evade their carers at the same time for a sexual encounter to take place.
What I learnt from the hearing
I was particularly interested to attend a court hearing because it is an experience that I have missed out on due to the pandemic. Normally, during first year of our social work course, we get the opportunity to visit courts and observe some hearings, but obviously this has not been possible.
However, we have been lucky enough to have District Judge Powell take the time to speak to us and answer our questions. One of the things she explained to us was how you address judges of different levels. I noticed straight away these address terms being used, with Mr Justice Hayden (as a High Court judge) being referred to as “My Lord” or “Your Lordship” throughout. I found it interesting to see how the addressing of a judge works in practice, because when District Judge Powell told us about it I could not picture how, or why, you would use this formal title more than once or twice. I learnt that the term actually replaces “you” when addressing them. I was pleased to hear other people use these terms before having to use them myself.
Also, I was amazed that – even via video conferencing – you could still feel the power that Mr Justice Hayden possessed, yet despite this he was still incredibly compassionate. It did make me think how much more powerful High Court Judges if you were stood in front of them in a court room.
In my lectures we have been learning about the Mental Capacity Act 2005 so it was useful to see it being applied in practice. I was impressed by how thorough everything was and how every little detail is picked apart to make sure the right outcome was decided for P. It was very interesting to see how Mr Justice Hayden was considering questions beyond the direct question that was being asked of him. The case was to decide whether she could have an IUD and move to a different, less restrictive, home. Mr Justice Hayden considered questions around her capacity to consent to sexual relations and the implications that having a coil inserted would have for her.
Having heard Mr Justice Hayden’s line of questioning in the morning, I thought he would not approve the order that it was in her best interests to have contraception and the move to this new home. I thought that if P does not have the capacity to consent to sex, then putting her in a position where it was considered necessary for her to have birth control “just in case” left her vulnerable to being raped.
However, I learnt from Celia Kitzinger by the end of the day that the ruling went the other way. This was partly because Mr Justice Hayden found that the presumption of capacity in relation to sexual relations had not been rebutted. He authorised P’s contraception and move to the new placement as the least restrictive option. From this I learnt that promoting P’s autonomy is an important value in the Court of Protection.
Jasmine Thomson is a first-year social work student at Bournemouth University.